
記住我

Aseptic necrosis of the lunate bone is one of the most common diseases that contribute to wrist pain. This was first discovered by Peste in 1843, and was reported in detail by Kienböck in 1910. Hence, it was also called Kienböck's disease1. The main symptoms of this disease include pain, attenuation of grip strength, and limited range of motion of the wrist joint. In particular, its early symptoms are often atypical, which easily leads to misdiagnosis.
The cause of this disease remains unclear. Academic scholars in this field can be divided into two camps: internal theory and external theory. It has been generally considered that the combined effects of internal and external factors lead to the disruption of the peripheral venous return or destruction of the blood microcirculation in the bone, and is followed by arterial insufficiency, which leads to malnutrition and aseptic bone necrosis2, 3.
Recent studies have shown that the treatment of osteonecrosis of the lunate should protect wrist function as much as possible. For adolescent patients, the treatment is mainly to prolong the fixed time. When this method cannot achieve the desired effect, minimally invasive surgery is used to relieve symptoms. For adult patients, the preferred treatment is also fixed. If the condition continues to worsen, it can be repaired surgically. If the lunate is no longer possible to be reconstructed, treatment should also focus on maximizing the preservation of wrist function4. The treatments of this disease in the late stages include shortening of the radius, distal radial or carpal osteotomy, proximal row carpectomy, partial carpal arthrodesis, wrist arthrodesis, vascularized bone graft, lunate bone extirpation, and artificial lunate bone replacement5-13. Different treatment methods have different effects on wrist joint function. Thus, the exploration and innovation of treatment methods can continuously improve the therapeutic effect of lunate osteonecrosis.
With the continuous development of minimally invasive surgical techniques, technological innovations are largely revolutionizing the form of surgery and improving the effectiveness of treatment. As an innovation in wrist surgery, wrist arthroscopy has gradually changed from a diagnostic tool to an auxiliary surgical method in the treatment of a variety of wrist diseases. With the continuous development of technology, there are more and more types of wrist diseases suitable for arthroscopic treatment14. In recent years, with the development of the arthroscopic assisted technique, wrist arthroscopic-assisted extirpation for the treatment of aseptic necrosis of lunate bone has some advantages over open surgery. As we know, arthroscopy can comprehensively and accurately reflect the state of intra-articular. At the same time, the wound is small, the complications are less, and the recovery is fast. Now, it has become a common surgical technique in the diagnosis and treatment of joint diseases. According to one report, postoperative analgesic effect, the range of motion of the joint, and functional scores were improved in different degrees through this method, and the incidence of complications such as infection and nonunion decreased15.
As mentioned earlier, the treatment of lunate bone injury should maximize the preservation of wrist function. The degree of wrist function preservation is closely related to the choice of treatment methods. Compared with traditional surgery, arthroscopic surgery may have greater advantages in preserving joint function, but no study has evaluated the efficacy of wrist arthroscopy in the treatment of lunar osteonecrosis. Therefore, this study was followed up to achieve the following purposes: (i) Comparison of wrist arthroscopy surgery and traditional wrist surgery; (ii) evaluate the therapeutic effect of wrist arthroscope on aseptic necrosis of lunate bone; and (iii) innovate the method of treating aseptic necrosis of lunate bone by wrist arthroscope. We believe that this technique is worthy of clinical promotion.
Materials and Methods Inclusion and Exclusion criteriaInclusion criteria: (i) diagnosis of aseptic necrosis of composite lunate; (ii) patients with stage IIIA or IIIB (Lichtman stage [3]); and (iii) patients treated with arthroscopic assisted fusion of the head and boat joint.
Exclusion criteria: (i) patients with stage I, II or IV of aseptic osteonecrosis; and (ii) patients with less than half a year follow-up time or incomplete data.
General InformationFrom March 2012 to January 2016, 12 patients were enrolled into this study. Patients ranged in age from 25 to 42 years, with a mean age of 32 years. Among these patients, 10 patients were male and two patients were female. The age of these patients ranged between 25–42 years old, with an average age of 32 years old. These lesions were located in the right hand in eight patients, and in the left hand in four patients. Lichtman stage: stage IIIA in two patients, and stage IIIB in 10 patients. All patients were diagnosed by anterior lateral radiographs and magnetic resonance imaging (MRI). Patients were followed up for at least half a year. The procedures of this study were approved by the ethics committee, and informed consents were obtained from all patients.
In addition, in this study, all patients achieved fracture healing within 9–12 weeks after surgery, with an average healing time of 10 weeks. The follow-up period in this study was 6–14 months, with an average duration of 8 months.
Surgical Procedure Anesthesia and PositionRoutine brachial plexus anesthesia was carried out for patients, and patients lay in the supine position. The pressure of the upper arm tourniquet was set at approximately 350 mmHg. The upper limbs were fixed with a Linvatec traction frame, and traction was carried out after the forefinger and middle finger were fixed by the fingertips. The traction weight was 5 kg, and the gravity perfusion system was perfused with flushing fluid.
Approach and ExposureThe 3–4 and 4–5 approaches at the radiocarpal joint, radio-midcarpal approach, ulno-carpal approach and scaphotrapezium-trapezoid (STT, scaphoid bone) approach were marked with a marking pen. A 2.7-mm arthroscope was used in the surgery. First, the arthroscope was inserted into the radiocarpal space via the 3–4 approach, and intra-articular drainage was carried out at the 6-U site using a type-4 needle. The radiocarpal joint was checked, and attention was given on the presence of hyperplasia, degrees of cartilage softening and degrees of defect in the synovial tissue. A planer was inserted via the 4–5 approach to remove synovial tissue. Then, an arthroscope was inserted from the space of the radio-midcarpal joint. Drainage for the space of the triquetro-hamate joint was carried out using a type-4 needle to observe whether there was a collapse of the lunate bone and whether the scapho-lunate gap widened.
Extraction of Lunate BoneThen, a planer was inserted into the space of the ulno-carpal joint to remove synovial tissue, and the lunate bone was ground using a grinding head to gradually remove the necrotic lunate bone. Intraoperative C-arm fluoroscopy was carried out to confirm whether the lunate bone has been removed.
Removing cartilage and fixing scaphocapitate jointNext, grinding heads were inserted via the ulno-carpal space and the STT approach, respectively, in order to grind off the cartilage on the contact surface between the capitate bone and the scaphoid, until bleeding was found on the bone surface. Second, C-arm fluoroscopy was carried out to guide the implantation of two 2.0-mm hollow double-threaded compression screws to fix the scaphocapitate joint. Finally, the incision was sutured, and the hand was fixed with a short arm plaster cast. Typical surgical procedures are shown in Fig. 1, and diagrams for key point of the surgery are shown in Fig. 2.

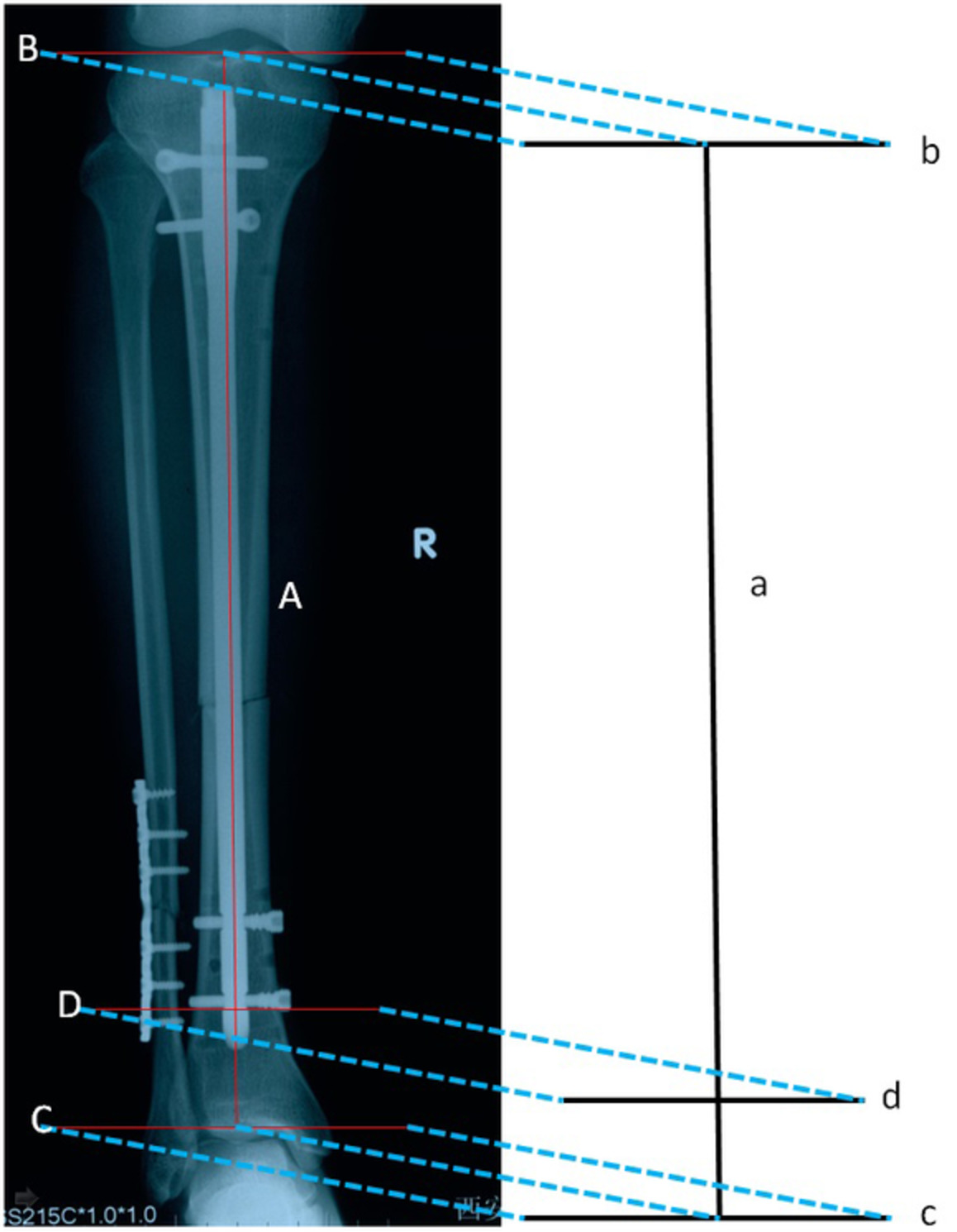
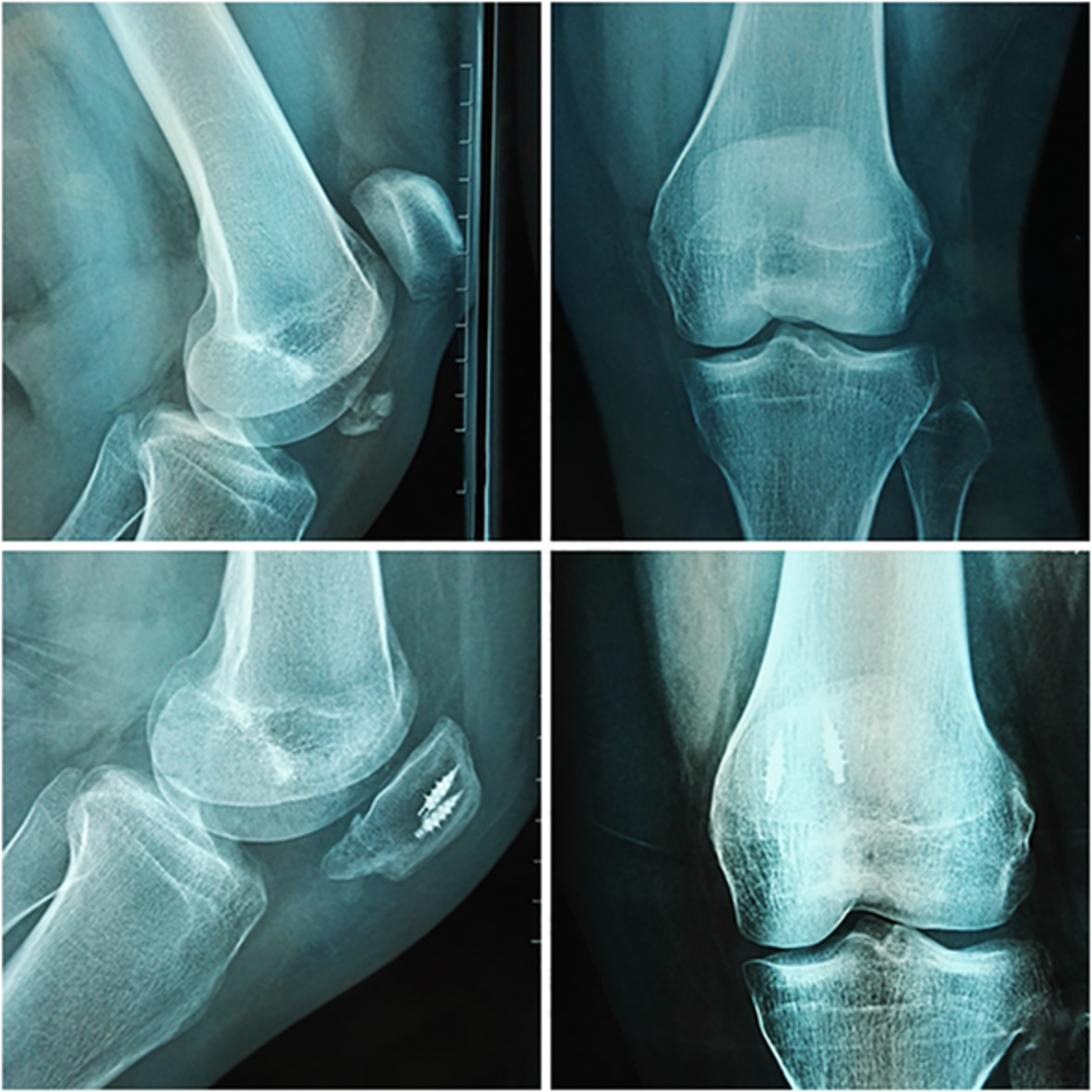
Operation of scaphoid arthrodesis internal fixation in a 28 year-old male patient with right wrist aseptic necrosis of lunate bone (Lichtman stage IIIB). (A) preoperative MRI image; (B) surface markings of the wrist joint dissection; (C) grinding of the cartilage on the contact surface between the capitate bone and lunate bone under an arthroscope; (D) X-ray film after removal of the lunate bone; (E, F) and (G) X-ray films for the fusion-stabilization of the scaphocapitate joint using double-threaded compression screws guided by the C-arm X-ray machine; H: wound of the dorsal wrist.

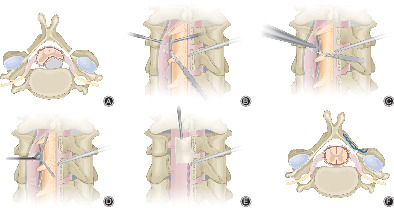
The diagrams for key point of the surgery. (A) Two channels (observation channel and operation channel) in the middle carpal joint. (B) After the lunate bone was removed under arthroscopy, the scaphoid and capitate joints were decorticated. (C) Two double screw compression screws were used to fuse and fix the scaphoid and capitate after cartilage removal.
Postoperative Care and Follow-upsFrom the second day after the surgery, patients underwent active motion for the metacarpophalangeal joint and interphalangeal joints. Stitch removal was performed 2 weeks after surgery, and 3 weeks after surgery the plaster cast was removed. Then, patients underwent limited wrist active exercise. When the X-ray film indicated that the fracture had healed, patients began to resume their daily activities and work. After surgery, the plain films of all planes, including the axial plane of the scaphoid, were taken every month, until the fracture had healed.
In terms of follow-up methods, we informed patients to come to the hospital outpatient clinic by regular telephone calls every month and obtained systematic follow-up data through physical examination, X-ray examination, and wrist function evaluation.
Outcome MeasuresThe operation time and hospitalization days were recorded.
Evaluation of Wrist FunctionWe also analyzed patients' wrist before and after surgery for dorsiflexion (the patient had wrist dorsiflexion, and the angle was measured), palmar flexion (the patient's wrist was flexed and the angle was measured), ulnar deviation (the wrist joint of the patient deviated to the ulnar side and the angle was measured), radial deviation (the patient's wrist deflected radially and the angle was measured), and grip (the patient gripped hard and the grip strength was measured using a dynamometer).
Mayo Wrist ScoreThe Mayo wrist score was used to assess the range of motion of the wrist joint and grip force during the follow-ups for objective function evaluation16. Including deformity (0–3 points), subjective evaluation (0–6 points), objective evaluation (0–6 points), complications (0–5 points). Excellent: 0–2 points, good: 3–8 points, fair: 9–20 points, poor: 21 points or more.
StatisticsGraphpad Prism 6.01 (GraphPad Software Inc., San Diego, CA, USA) was used for statistical analysis. Paired t-test was used to assess wrist function changes, just like operation time, hospitalization days, Mayo wrist score, dorsiflexion, palmar flexion, ulnar deviation, and grip, before and after surgery. The data were expressed as Mean ± SEM. P < 0.05 was used as the criterion for statistically significant difference.
Results Operative Time and Hospital StayTo evaluate the therapeutic effect of wrist arthroscopic surgery, we first evaluated the operative time and hospital stay of wrist arthroscopic surgery. Referring to our previous clinical experience, we found that the operation time and hospitalization days of patients were significantly shorter than those of traditional surgical methods. This indicates that wrist arthroscopic surgery can significantly improve the recovery efficiency of patients.
Wrist FunctionThere were significant improvements in dorsiflexion (from 33.25 ± 3.794 to 57.58 ± 4.001), palm flexion (from 17.33 ± 2.937 to 31.00 ± 2.686), ulnar deviation (from 30.08 ± 1.649 to 50.75 ± 2.415) and grip strength (from 12.60 ± 1.961 to 40.00 ± 1.703) (P < 0.0001, Table 1).
TABLE 1. Comparison of wrist joint activity before and after the operation Dorsiflexion (°) Palmar flexion (°) Ulnar deviation (°) Radial deviation (°) Grip (Kg) Before 33.25 ± 3.794 17.33 ± 2.937 30.08 ± 1.649 3.333 ± 0.4975 12.60 ± 1.961 After 57.58 ± 4.001 31.00 ± 2.686 50.75 ± 2.415 4.250 ± 0.4787 40.00 ± 1.703 P <0.0001 <0.0001 <0.0001 0.084 <0.0001 The values in the table represent “mean value ± standard deviation.” Mayo Wrist ScoreThe flexion and extension range of the wrist joint on the operated side was found to be 40°–110°, with an average of 105°, which was 80% of the healthy side. Radioulnar deviation was 45°–80°, with an average of 55°, which was 82% of the healthy side. The grip strength was 25–48 kg, with an average of 40 kg, which was 84% of the healthy side. The modified Mayo Wrist Score improved significantly in patients after surgery compared with before surgery (before vs. after, 66.58 ± 2.506 vs. 80.00 ± 2.332, P < 0.0001). The modified Mayo wrist score was good in eight patients, acceptable in three patients, and poor in one patient.
DiscussionFor aseptic necrosis of lunate bone, the most widely used classification standard is the image classification method proposed by Lichtman et al. in 1977, which was revised in 20012, 3. However, the credibility of this standard has also been questioned, especially because it is prone to error in distinguishing between stage IIIA (simple collapse of the articular surface of lunate bone) and stage IIIB (on the basis of stage IIIA patients, these are accompanied with volar flexion deformity of the scaphoid, movement of the capitate bone towards the proximal end, or height loss), which influences the selection of operation procedures and prognosis17. The application of arthroscopy can evaluate the cartilage condition of adjacent joints of lunate bone, and it is a minimally invasive treatment, which can reduce surgical complications. Watanabe et al.18 first used an arthroscope in the observation and staging of the nonunion of lunate bones. They revealed that patients in stage III or higher were prone to osteoarthritis. Based on arthroscopy, Bain and Begg proposed the use of the classification standard of nonunion of lunate bone19 to stage the disease according to the number of function-free joint surfaces among the four joint surfaces of the radio-luno-capitate joint. When all of the joint surfaces have function, but synovitis exists, the disease is classified as grade 0; and when one nonfunctional joint surface is found, the disease is classified as grade 1, and so on.
Clinically, dozens of surgical procedures for aseptic necrosis of lunate bone have been applied, which can be broadly divided into six categories: revascularization, biomechanical correction, simple resection, autologous bone or prosthesis replacement, wrist arthrodesis, and denervation. The guidelines for treatment drawn by Beredjiklian20 according to a large number of studies have received recognition from most of the peers (Table 2).
TABLE 2. Treatment of aseptic necrosis of lunate bone according to Lichtman stage Aseptic necrosis of lunate bone according to Lichtman stage Treatment advice I Gypsum fixed for 3 months II-III A, ulnar negative change Radial shortening, ulnar lengthening, capitate bone shortening II-III A, ulnar positive change Vascularized bone graft +external fixator, radial wedge osteotomy or enarthrodial osteotomy, capitate bone shortening III B Capitate bone adjacent joint fusion (scaphoid-trapezium-multangulum minus, scaphoid-capitate bone), lunate bone extirpated, radial shortening, proximal row carpectomy IV Proximal row carpectomy, wrist joint fusion, wrist joint denervationIn the field of arthroscopic treatment of aseptic necrosis of the lunate bone, Menth-Chiari et al.21 were the first to carry out a study on the arthroscopic removal of stage III lunate bone necrosis, and have harvested good effects. In all seven patients in their study, rest pain disappeared and the range of motion of the wrist joint improved, compared with preoperative status. However, some patients (2/7) still had active pain after the operation. The team of Leblebicioğlu22 carried out a comparison between arthroscopic and open surgical treatments for stage III lunate bone necrosis (in arthroscopic surgery, scapho-capitate arthrodesis and proximal capitate osteotomy were applied, while in open surgery, scapho-capitate arthrodesis and vascularized bone flap graft were applied). Results revealed that arthroscopic surgery could shorten operation time, and accelerate the turnover rate of hospitalization and postoperative recovery rate. However, differences in the prognostic range of motion and grip strength test results were not statistically significant. The surgical procedure used in this study absorbed the advantages of the Beredjiklian guidelines and the achievements drawn by Leblebicioğlu et al. in the application of arthroscopy, which has the following characteristics: (i) it causes small trauma, prevents damage to the wrist joint capsule, and preserves the ligament structure of the wrist joint as far as possible, thereby reducing iatrogenic damage. In addition, it allows the early rehabilitation training of the wrist joint, increases the speed of functional recovery of the wrist joint, and accelerates the turnover rate of hospitalization. (ii) The local scaphocapitate joint arthrodesis under arthroscopy has a certain degree of difficulty when carry out, but the advantages are significant: it allows the direct observation of the articular surfaces of the entire carpal bone during scaphocapitate joint arthrodesis, allowing the full removal of the contact surface cartilage, and is good for bone healing and stability. (iii) Arthroscopic extirpation of the necrotic lunate bone is very difficult when carried out. It is not always possible to completely remove the lunate bone, and a small part of the bone tissue may remain, especially the dorsal part of the lunate bone. However, according to the follow-up results, no adverse reactions induced by this operation were found. (iv) Scapho-capitate arthrodesis was carried out using a countersunk double-threaded screw, which is firm and convenient, and can also avoid secondary removal. (v) It allows concurrent arthroscopic debridement. According to a number of reports23, 24, aseptic necrosis of the lunate bone is easily associated with traumatic arthritis, and hyperplastic synovial tissue can be thoroughly removed by arthroscopic debridement, which can reduce the incidence of postoperative wrist arthritis. In the present study, good results were achieved: the pain of all patients improved compared with that before the operation, and wrist pain symptoms disappeared in eight patients, while mild rest pain remained in four patients; grip force and joint mobility were significantly improved compared with preoperative status; no complications occurred. However, this study also has some shortcomings: the sample size was small, and follow-up duration was short. Hence, statistical bias was difficult to avoid, which led to the decline in credibility.
ConclusionIn summary, wrist arthroscopy is an effective and feasible tool for the treatment of aseptic necrosis of the lunate bone.
留言 (0)