
記住我

Cervical myelopathy is a common pathology in older individuals and is characterized by compression of the cervical spinal cord from ventral or/and dorsal lesions1. There are many causes of cervical myelopathy including cervical spinal canal stenosis, cervical disc herniation (CDH), ossification of posterior longitudinal ligament (OPLL), ossification of ligamentum flavum and degenerative disc disease. Cervical myelopathy causes severe clinical symptoms and various disorders, mainly muscle weakness, upper extremity paresthesia, and gait disturbance2. Cervical myelopathy is usually progressive and responds poorly to conservative therapy. Therefore, surgical treatment is regarded as the effective method to limit progression of clinical symptoms. Due to this, a variety of surgical procedures have been developed to treat cervical myelopathy. However, there are some limitations and drawbacks with these operations; in particular, there are debates over the optimal surgical technique for the treatment of multi-segment cervical spinal stenosis (CSS) accompanied with CDH.
Anterior cervical discectomy and fusions (ACDF) has become a standard surgical procedure for CDH, since Robinson first described the anterior cervical approach in 19553, 4. Although ACDF is regard as an effective treatment option for CDH, adjacent-segment syndrome is one of the most common complications at the time of long-term follow-up5, 6. As reported, adjacent-segment syndrome, which is described as symptom deterioration due to disc degeneration at one or two adjacent cervical levels associated with ACDF, may affect more than 25% of patients who undergo this surgery7, 8. Many studies reported that adjacent cervical disc degeneration that developed after ACDF may be associated with reduced movement of fused segments and increased stress of adjacent segments9. Fraser and Härtl10 reported that ACDF was associated with plate loosening, postoperative dysphagia, and cervical soft tissue injury. In addition, the limited operational space and higher surgical risk should be considered in the process. Posterior procedures were initially employed for management of cervical myelopathy6, 11. However, many physicians consider that the technique has many potential risks, with injury of nerve function being one of them. Meanwhile, the posterior surgical outcome of CDH was not always satisfactory because of postoperative axial pain and indirect decompression of ventral lesions. Traditionally, the posterior approach with laminoplasty or laminectomy to the cervical spine may be an important part of the operative policy for cervical myelopathy caused by multilevel spondylosis, spinal stenosis, cervical ossification of ligamentum flavum and OPLL12. It is worth noting that this surgical method may lead to C5 palsy because of the indirect decompression of ventral herniated disc13.
In 1910, Taylor14 first reported a new posterior surgical technique: unilateral transdural approach which is a management of the ventral lesion of the cervical cord. For the next 30 years, transdural discectomy with laminectomy or laminoplasty is regarded as an accepted treatment for huge CDH and cervical myelopathy, the chief goals of surgical treatment including resection of vertebral plate or laminoplasty, transdural discectomy, neurologic decompression, and stabilization of cervical segments8, 15. Cervical transdural discectomy with laminoplasty (CTDL) is a type of posterior procedure and characterized with non-fusion and direct decompression of ventral lesions. CTDL technique gives patients the advantages of both ACDF and traditional posterior procedures, such as discectomy, direct decompression of the spinal cord, preservation of the cervical segment motion, less destruction to the vertebral plate, a decrease in the rate of adjacent-segment syndrome and C5 palsy5, 6, 16. For multi-segments CSS accompanied with CDH, traditional posterior procedures and ACDF approaches typically are not insufficient because the compression of spinal cord and nerve root cannot be completely released. In 1994, Fox and Onofrio17 reported that transdural discectomy with laminectomy technique was ideal for management of multi-segmental CSS with CDH. Yue et al.18 reported that one stage laminoplasty and posterior herniotomy was an effective procedure for the treatment of myelopathy, which involved the advantages of direct decompression and avoiding incision of dorsal dura mater. However, this technique is associated with intraoperative excessive stretching of the spinal cord and anterolateral dural venous plexus hemorrhage. Furthermore, with the improvement of microsurgical instruments and development of intraoperative neurophysiologic monitoring, CTDL has been accepted by an increasing number of physicians. In addition, the increasing patient demands for surgical outcomes and quality of life also contributed to the propagation of the advanced surgical method8.
To our best knowledge, there were a limited number of studies that have evaluated the clinical outcome of the transdural approach for the treatment of CSS and CDH. Due to this, surgeons lack references relating with CTDL technique and clinical experiences of evaluating preliminary surgical outcome. In recent years, we have treated some cases of multi-segments CSS accompanied with CDH by CTDL. In addition, the data of those cases were collected and analyzed retrospectively. Thus, the aim of this study was to: (i) demonstrate the surgical technique of CTDL; (ii) investigate the preliminary surgical outcome and complication of CTDL for multi-segment CSS accompanied with CDH; and (iii) share preliminary clinical experience to provide surgeons and patients with a relevant theoretical basis for the choice of this operative method.
Materials and MethodsFrom 2012 to 2018, a total of 31 patients (13 males, 18 females) who underwent CTDL were included in the study according to the screening criteria retrospectively. All diagnoses were based on clinical symptoms and radiological imaging manifestations and confirmed by more than one spinal surgeon. The procedures were approved by the ethics committee of the Affiliated Hospital of Qingdao University. Written informed consent was obtained from all participants.
Inclusion and Exclusion CriteriaThe clinical indications of CTDL and inclusion criteria were defined as follows: (i) multi-segment CSS (over two cervical segments) accompanied with huge CDH; and (ii) with neural symptoms such as sensory disturbance.
The exclusion criteria were defined as follows: (i) serious systemic diseases including trauma, infection, and spinal metastasis; (ii) intolerable to operation; (iii) previous lumbar surgery; and (iv) incomplete clinical data.
Surgical TechniqueAfter general anesthesia, the patient was placed in the prone position on the table. Head was stabilized by a perspective head holder and flexed to reduce the overlap of the laminae and facet joints. Arms were placed at sides and stabilized by tapes. Spinal cord monitoring was performed during the procedure to prevent unexpected nerve injury. The location of the exact skin incision was determined and marked according to preoperative imaging features.
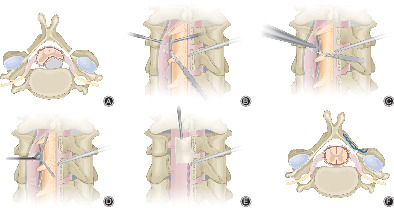
LaminoplastyA standard posterior cervical median longitudinal incision was made, the spinous processes, laminae, and articular facets were separated and exposed by electric surgical knife. The V-groove should be created at the junction of laminar and lateral mass by a high-speed burr, and the structure of the inner cortex bone should be preserved as greenstick hinge. For better decompressive effects, the process is generally performed on the side with milder clinical symptoms. It is worthy to note that the bone burr should be perpendicular to the lamina in the process, rather than perpendicular to the facet joint19. The gutter on the “open side” was created on the opposite side. A 2-mm laminectomy rongeur was used to create the “open side” trough at the lamina border and cut off the ligamentum flavum. Different from the side of the hinge, all cortex bone and cancellous bone were removed on the “open side.” By carefully lifting the lamina from the “open side” to the side of hinge with a curette, the dural sac was fully exposed (Fig. 1A).

(A) Laminoplasty. (B) Transection of the lateral dentate ligament. (C) Longitudinal incision of the ventral dura. (D) Herniated disc was removed with a nucleus pulposus forceps. (E) Stitching the dorsal dura and artificial dura mater was wrapped. (F) ARCH plate was fixed with titanium screw on each segment.
Transdural DiscectomyWhile the arachnoid membrane was preserved, the dorsal dura mater at the level of huge herniated intervertebral disc was longitudinally incised at about a 1.5 cm length. After incision, the bilateral dura maters of incision were fixed with sutures, respectively. With or without the assistance of an operation microscope, the dura mater was gently pulled bilaterally with silk thread to expose the surgical space and dentate ligament. Dentate ligaments are connective tissues attached to dura mater and spinal cord, the function of it is the suspension and stabilization of the spinal cord (Fig. 1B). After transection of the dentate ligament, the spinal cord was protected with dural separator, meanwhile, the dural separator was gently rotated to clockwise to slowly shift the spinal cord from the surgical site to the opposite side until the midline of the ventral dura mater was exposed. The bulging of the ventral dura mater caused by huge CDH could be observed clearly. The ventral dura mater was further incised longitudinally to expose herniated cervical intervertebral disc and ossification of posterior longitudinal ligament (Fig. 1C). The procedure was operated according to the method and technique described by Fujimoto8. Nucleus pulposus forceps were used to remove the herniated disc fragments and ossification (Fig. 1D).
Repair of Dura Mater and ARCH Plate FixationThen, under direct vision, watertight closure of the incision of ventral dura mater was performed using 6–0 nylon suture. A suitable size artificial dura mater was wrapped around the ventral spinal cord to cover the ventral defect of the dura mater. Before stitching the dorsal dura mater, decompression effect of the spinal cord and nerve root, excision effect of herniated disc and ossification, and complete hemostasis were confirmed again. The incision of dorsal dura mater was also stitched with 6–0 nylon suture and covered with a piece of trimmed artificial dura mater (Fig. 1E). ARCH plate (Johnson & Johnson Inc., NJ, America) with suitable size and shape was placed and fixed with four titanium screws (two screws in the lateral mass, and two in the lamina, length of 6 and 8 mm) on each segment (Fig. 1F). The incision was rinsed with more than 2500 mL normal saline. Finally, we routinely place a subfascial drainage tube at the wound and close the wound in the standard method in three layers.
Postoperative ManagementPainkillers, antibiotics, methylprednisolone, and mannitol were routinely used for 48 h postoperatively. Postoperatively, cerebrospinal fluid (CSF) was drained within 200 mL every day until the drainage was clear. The subfascial drainage tube was routinely removed at 2–3 days postoperatively. If there was CSF leakage, the drainage tube was retained until the volume of drainage was less than 50 mL/24 h. Meanwhile, patients with CSF leakage were managed by extending extubation time, local compression bandage, and prolonged courses of antibiotics to prevent infection. In addition, postoperative flat bed rest is beneficial to the healing of dura mater and surgical incision. Patients were suggested to ambulation under the protection of neck brace, after the drainage tube was pulled out. Neck brace was required for immobilization for 1 month.
Outcome EvaluationsThe average follow-up period was 65.03 months (ranging from 24 to 126 months). Demographic and baseline characteristics of patients in the study were collected, such as age, sex, operative level, operative time, estimated blood loss, ambulation time, and operative complications. Complications of the operation were also recorded. The patients were reviewed 24 months after surgery, and radiographic improvement was observed by X-ray imaging, 3D computerized tomography (CT) examination and scan, and magnetic resonance imaging (MRI). Preoperative JOA score as well as postoperative JOA score, JOA score at the final follow-up, and clinical improvement were evaluated.
Visual Analog Scale (VAS)Neck pain and arm pain were evaluated using VAS preoperatively, at 24 months postoperatively, and at the final follow-up. The VAS is a continuous scale comprised of a 10-cm horizontal line, usually used to measure the quantification of pain. The scale of pain intensity is most commonly divided: no pain (0–2), mild pain (3–5), moderate pain (6–8), and severe pain (8–10).
Japanese Orthopaedic Association (JOA) scoreThe postoperative improvement of symptoms was evaluated by recovery rate of the JOA scoring system. Its total score is 17 points. Recovery rate (%) = (postoperative JOA score – preoperative JOA score)/(17 – preoperative JOA score) × 100%. According to the score, the recovery rate was classified into four grades: excellent (75% to 100%), good (50% to 74%), fair (25% to 49%), and poor (0% to 24%).
Sagittal Maximum Spinal Cord Compression (SMSCC)According to the method reported20, 21, SMSCC was described based on diameter of the most compressed spinal cord diameter (b), diameters of the nearest normal level above (a), and, below (c), the level of sagittal most compressed on the midsagittal MRI. SMSCC = [1 − b/[(a + c)/2]] × 100% (Fig. 2A).

MRI of a 48-year-old man with multi-segment CSS accompanied with huge CDH shown: (A) The preoperative and (B) postoperative midsagittal MRI; (C) The preoperative (D) and postoperative axial MRI; (E) The preoperative and (G) postoperative CT images; (G) The preoperative and (H) postoperative CT images (bony window); (A) Three diameters used to describe SMSCC. (C) Anteroposterior and transverse diameters of spinal cord used to measure compression ratio.
Compression RatioCompression ratio was measured based on anteroposterior diameter and transverse diameter of the cervical spinal cord on MR axial imaging at the most compressed level. As described by Gu et al.22, compression ratio = anteroposterior diameter/transverse diameter ×100% (Fig. 2C).
Cervical Range of Motion (ROM) and AlignmentPre- and postoperative ROMs were used to evaluate the effect of the cervical stability in the study. Lateral radiographs in full flexion and full extension were taken before and 24 months after the surgery. According to the Penning method23, the ROM between C3–C7 was measured based on lateral flexion and extension radiograms. As described by Ishihara24, alignment was classified as lordotic, straight, and kyphotic.
Statistical AnalysisStatistical analysis was performed using the SPSS 22.0 statistical software package (SPSS Inc., Chicago, IL, USA). Continuous variables were shown as mean ± standard deviation (x ± s) and categorical variables were shown as a percentage (%). The preoperative and postoperative follow-up parameters (JOA, transverse compression ratio, and SMSCC) were assessed with paired t test. A P-value <0.05 was considered statistically significant.
Result General ResultsThe mean age of the 31 patients was 55.23 ± 10.97 years, and there were 13 males and 18 females. The mean operative time was 192.45 ± 24.17 min (ranging from 150 to 245 min), and intraoperative blood loss was 322.58 ± 129.00 mL (ranging from 150 to 600 mL). The mean length of time to ambulation was 2.80 ± 1.11 days. In addition, the most common laminectomy level was C3–7 (18 patients, 58.06%), followed by C3–6 (eight patients, 25.80%) and C4–7 (five patients, 16.13%).
Recovery RateThe results of recovery rate at 24 months postoperatively demonstrated that excellent results were observed in 17 patients (54.84%), good in 11 patients (35.48%), fair in two patients (6.45%), and poor in one patient (3.23%). One of the patients with fair results was observed for improvement of recovery rate at the final follow-up examination (from 46.43% to 64.29%). The recovery rate of one patient with poor result raise was 14.29% at midterm follow-up, but it was raised to 71.43% finally. In addition, the mean recovery rate of all patients at 24 months postoperatively was 72.95 ± 20.41% and the mean recovery rate of all patients at final follow-up was 77.15 ± 16.61%.
Visual Analog Scale (VAS)As shown in Table 1, the mean preoperative VAS neck pain was 5.94 ± 1.18, the mean VAS neck pain at 24 months postoperatively was 1.87 ± 0.67, and the last follow-up VAS neck pain was 1.68 ± 0.48. The VAS neck pain was improved significantly over the follow-up period (P < 0.05). The VAS arm pain improved significantly from 6.26 ± 0.93 preoperatively to 1.74 ± 0.63 at 24 months postoperatively (P < 0.001). There was no significant difference in improvement of VAS arm pain between 24 months postoperatively and final follow-up (P = 0.180).
TABLE 1. VAS, JOA, and radiographic parameter Indexes Value (x ± s) t value P value VAS (neck pain) Preoperative 5.94 ± 1.18 Postoperative 1.87 ± 0.67 25.37 <0.001a Final follow-up 1.68 ± 0.48 2.26 0.032a,b VAS (arm pain) Preoperative 6.26 ± 0.93 Postoperative 1.74 ± 0.63 31.00 <0.001a Final follow-up 1.65 ± 0.61 1.36 0.184 JOA score Preoperative 9.66 ± 2.81 Postoperative 14.79 ± 1.84 −14.00 <0.001a Final follow-up 15.06 ± 1.71 −2.03 0.051 Compression ratio 18.86 <0.001a Preoperative 27.17 ± 3.89 Postoperative 58.30 ± 8.51 SMSCC 11.53 <0.001a Preoperative 33.66 ± 5.38 Postoperative 25.12 ± 5.67 ROM 1.85 0.740 Preoperative 31.12 ± 2.84 Postoperative 30.40 ± 2.92 JOA score, Japanese Orthopaedic Association Scores; ROM, cervical range of motion; SMSCC, sagittal maximum spinal cord compression; VAS, Visual Analog Scale. Japanese Orthopaedic Association (JOA) scorePreoperative and postoperative JOA scores, and recovery rate of the JOA scoring system were used to evaluate the postoperative improvement of symptoms. The mean preoperative JOA score of the 31 patients was 9.66 ± 2.81 (ranging from 3.5 to 14.5), and the mean postoperative JOA score was 14.79 ± 1.84 (ranging from 10 to 17) in follow-up period of 24 months. In final follow-up, the mean postoperative JOA score was 15.06 ± 1.71 (ranging from 10 to 17). Comparing with preoperative JOA score, JOA score were significantly improved at 24 months postoperatively (P < 0.001). Meanwhile, there were no statistically significant differences between the final follow-up and the postoperative JOA scores (P = 0.051).
Compression Ratio and Sagittal Maximum Spinal Cord Compression (SMSCC)The postoperative SMSCC ranged from 5.67 to 38.51 and showed significantly milder compression than preoperative SMSCC (25.12 ± 5.67 vs 33.66 ± 5.38, P < 0.001). Patients had significantly higher postoperative index of compression ratio than preoperative ratio (58.30 ± 8.51 vs 27.17 ± 3.89, P < 0.001).
Cervical Range of Motion (ROM) and AlignmentAt 24 months after operation, the mean cervical ROM had decreased from 31.12 to 30.40. But the result showed that preoperative and postoperative cervical ROMs were not significantly different during the 24-month follow-up period (P = 0.740). Meanwhile, there was no kyphotic deformity, cervical axis symptoms, and postoperatively segmental instability observed on lateral cervical radiographs after surgery.
ComplicationsAll patients were followed up for more than 24 months (range 24–126 months). However, one patient observed postoperative symptom of C6 nerve root injury, possibly related to intraoperative excessive surgical manipulation and stretching of the nerve roots, which was resolved within 12 months after the surgery. Intraoperative neurological monitoring reflected the stretching of the C6 nerve root (Fig. 5). Spinal cord injury, infection, hinge fracture, and C5 palsy were not observed in present study. There were two cases involving postoperative CSF, possibly related to laceration of dura mater. For the two patients with CSF, the drainage was controlled within 150–200 mL every day. In 5 days after surgery, the drainage was less than 50 mL/24 h, and the drainage tube was pulled out. Meanwhile, the courses of antibiotics were also prolonged to 5 days after surgery to prevent infection. The two patients were discharged at postoperative 1 week, no fever and infection were found during out-patient reviews. The functional scores and radiographic parameter reached average value, which showed the clinical results were satisfactory.
Discussion Advantages of CTDLACDF technique is one of the most common cervical procedures and is associated with less intraoperative blood loss, shorter ambulation time, and excellent surgical outcome, but with high incidence of postoperative adjacent-segment syndrome25, 26. Goffin et al.27 reported that adjacent segment degeneration was observed in 92% of patients after ACDF. Therefore, if patients with CSS accompanied with CDH want to get long-term satisfactory outcomes, the problem with the adjacent intervertebral segment must be solved8, 26. But ACDF and laminoplasty cannot achieve satisfactory results for those patients. The CTDL technique was evolved from posterior laminoplasty and has become an effective treatment for multi-segment CSS accompanied with CDH15. Although this technique is a posterior procedure, it still can achieve direct decompression of ventral herniated disc by transdural discectomy. The significant improvement of radiographs (SMSCC and the index of compression ratio) reflects the efficient decompression of the spinal cord so that the clinical surgical indications were strictly defined: multi-segment CSS (over two cervical segments) accompanied with huge CDH.
In addition, as a non-fusion surgical technique, CTDL technique avoids reduction of vertebral mobility and adjacent-segment syndrome effectively. The spinal canal expansion was maintained firmly with titanium plates, which was beneficial for high fusion rate and improving cervical stability and activity. The lateral flexion and extension radiogram showed that there was not significant difference between the preoperative and postoperative cervical ROMs. Meanwhile, kyphotic deformity, cervical axis symptom and postoperatively segmental instability were not observed in all patients followed for 24 months. The significant improvement of JOA score and recovery rate (mean JOA score: from 9.66 to 15.06; recovery rate: from 72.95 to 77.15) reflect the persisted improvement of symptoms and function of patients during the follow-up period. Therefore, the lesser dissection of normal structures, lower incidence of complications, and relatively complete preservation of cervical functions may support the selection of the CTDL8.
The Technique of Transection of the Dentate LigamentComparing with single laminoplasty with herniotomy technique, transection of the dentate ligament is one of the key steps of the procedure. On the one hand, this process can reduce the damage to the bilateral facet joints and vein plexus, and the intraoperative blood loss; On the other hand, it can increase the range of motion of the spinal cord, expose and remove the herniated intervertebral disc easily, and avoid excess nerve stretch. But special care should be taken to avoid unnecessary incision of dentate ligament in other cervical surgeries. Ceylan et al.28 reported that resection of dentate ligament may lead to spinal cord instability within the spinal canal, which exposes the cord to trauma. Meanwhile, the range of motion of spinal cord will increase in theory after the transection of dentate ligaments, which may have some impact to the function of the spinal cord. Many studies reported that increased cord movement may be the possible reason for Hirayama disease: the increased laxity permits anterior displacement of the spinal cord causing microcirculatory disturbances of the anterior portion of the spinal cord, and eventually leads to myelopathy and degeneration29, 30.
Complications and Management C5 PalsyThe theoretical basis of laminoplasty is that through enlarged cervical canal and drift, the spinal cord moves away from anterior lesions to achieve indirect decompression of anterior lesions. However, some patients with huge herniated intervertebral disc were difficult to gain satisfied surgical results of laminoplasty because the herniated disc and endplate may not easily be absorbed31, 32. For laminoplasty, deficient decompression of ventral lesions may the main causes of excessive drift of nerve root and C5 palsy. Comparing with laminoplasty, CTDL has access to direct decompression of ventral compression of spinal cord such as CDH and OPLL. Radiographic findings in cases of cervical disc herniation suggested increased tension on nerve roots outside the dural sac. Application of longitudinal durotomy in CTDL resulted in the decrease of the tension of nerve root (Figs 3 and 4). Therefore, C5 palsy was not observed in our study because of the complete resection of huge herniated intervertebral disc and prevention of postoperative spinal cord shift. Direct decompression of the spinal cord and non-fusion procedure can be achieved by transdural discectomy with laminoplasty.

Radiographs of a 57-year-old woman. (A, B) The preoperative MRI. (C, D) The postoperative MRI. (E, F) The postoperative radiographic image.

Radiographs of a 63-year-old woman. (A, B) The preoperative MRI. (C, D) The postoperative MRI. (E, F) The postoperative radiographic image.

(A) The stimulation of C6 nerve root was recorded by electrode needles that were inserted in bilateral deltoids and biceps. The detection mode was to be set to Free-EMG. (B) The stimulation of the C6 nerve root was detected (The normal Free-EMG should be a linear resting waveform).
Nerve Root InjuryEvery operation method may be accompanied by several complications. In our study, cervical nerve root injury was observed in one patient with huge CDH after surgery, which appears to be caused by intraoperative stretching of the nerve roots. Hasegawa et al.33 reported that cervical spinal cord reperfusion injury is also associated with the complication. Neurological monitoring and operation microscope not only can prevent intraoperative injury of nerve root and spinal cord but also improve the clinical effect and safety of this procedure34. In addition, the transection of the dentate ligament can provide space for transdural discectomy and reduce intraoperative nerve injury.
CSF LeakageThe risk of postoperative CSF is inevitable on cervical transdural discectomy. The tight suture technique of dorsal dura mater, application of artificial dura mater, and short length of the dural incision can effectively prevent postoperative CSF35. Intraoperative mass saline irrigation, extending extubation time, local compression bandage and prolonged courses of antibiotics are the most effective measures to prevent infection for patients with CSF leakage.
RecurrenceNo recurrence was found in our study. We conclude that the remaining intervertebral disc tissue that remained after removing the herniated disc maybe not be enough to form compression. In addition, the pressure on the cervical intervertebral disc is much less than that of the lumbar intervertebral disc; therefore, the remaining intervertebral disc tissue rarely protrudes again.
Limitation of the StudyThere are some limitations to the present study. First, the study lacked a comparison to ACDF or pure laminoplasty, and the evaluation index system of surgical outcome has not been unified. Second, CTDL technique not has been widely used in the clinic, so that the number of patients were relatively small. Finally, the follow-up period was not long enough. A larger sample with a longer follow-up time is needed to draw definitive clinical conclusions.
ConclusionsIn the present study, CTDL technique has shown great advantages in terms of the curative effect in patients with multi-segmental CSS with CDH. Therefore, this technique is a safe and effective surgical method for selected patients. In addition, the indications of the procedure are relatively limited, the patients need to be selected strictly.
留言 (0)