
記住我

Atlantoaxial dislocation is the most common severe injury in the upper cervical spine. If timely treatment is not provided, the degree of dislocation is often progressively aggravated, leading to compression of the spinal cord and life-threatening side effects. The atlantoaxial joint is an interlocking configuration. The odontoid process prevents backward dislocation of the atlas on the axis. Therefore, posterior atlantoaxial dislocation (PAAD) is usually associated with odontoid process fracture or a congenital deformity1, 2. PAAD without fracture of the odontoid process is extremely rare. In 1969, Haralson and Boyd3 reported the first case of such an injury. Although a few isolated cases have been reported subsequently, the ideal treatment strategy remains controversial, and the prognosis is unclear.
We present a case of PAAD without associated fracture or a significant change in spinal cord signal. Closed manual reduction was performed after applying general anesthesia, and pedicle screw internal fixation via the posterior approach was applied to maintain stability. To our knowledge, this is the first case of reduction of a PAAD without fracture of the odontoid process by manual traction. During the procedure, we developed a new method, the atlantoaxial dynamic test to confirm the integrity of the transverse ligament.
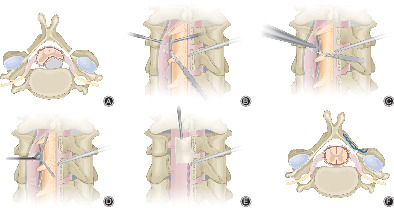
Case ReportA 54-year-old female was riding in the passenger seat when her vehicle was rear-ended by a car on the highway. She had a transient loss of consciousness, and the patient complained of headache and considerable pain and stiffness in the neck after recovery of consciousness. Her vital signs were normal, but the neurological examinations showed mild neurological deficits in her right extremities with grade 4/5 power. PAAD without an associated fracture was diagnosed using computed tomography (CT) (Fig. 1A–C). Preoperative examinations and magnetic resonance imaging (Fig. 1D, E) were performed following admission. No abnormalities were found on head CT. After admission, surgery was arranged for the next day. Sober intubation was performed to avoid potential aggravation of the spinal cord injury by cervical extension. After induction of general anesthesia, closed manual reduction under C-arm fluoroscopy was performed with the patient in the supine position (Figs 2A, 3A, B). The surgeon stood above the patient's head, with one hand on the patient's occipital space and the other hand encircling the patient's jaw. The assistant stood next to the patient and put his hands on the patient's shoulders for counterpressure. The surgeon applied a force first, and the assistant gave a counterforce as the situation required. The surgeon maintained a light force so as to stretch the neck, When the distraction of the anterior arch of the atlas had reached a level closer to the tip of odontoid process, the surgeon applied a little force and gently flexed the cervical spine. and the dislocation was reduced, making an audible snap.

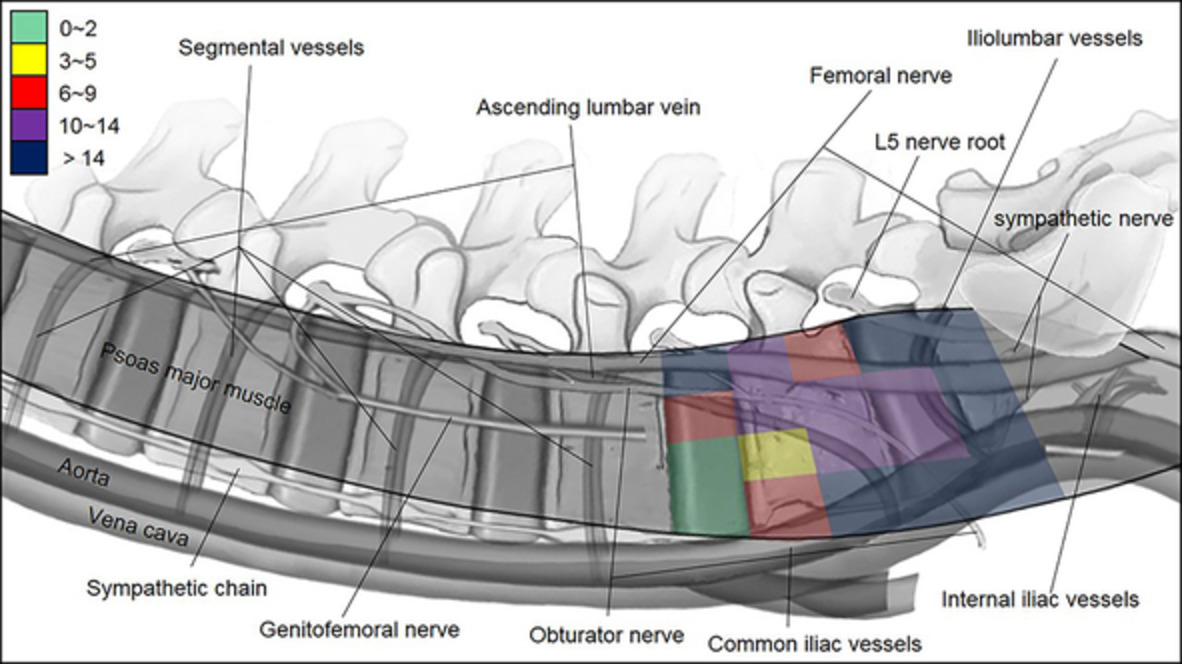
Sagittal and axial planes of the atlas (A, B) and 3D-CT (C) show posterior dislocation of the atlas without associated fracture. MRI (D, E) demonstrated no cord compression or intramedullary cord signal abnormality at the level of atlantoaxial dislocation.

Manual reduction (A): after induction of general anesthesia,the surgeon stood above the patient's head, with one hand on the patient's occipital space and the other hand encircling the patient's jaw. The surgeon applied force first, and the assistant gave counterforce as the situation required. The surgeon maintained proper force so as to stretch the neck, then he applied a little force and gently flexed the cervical spine, then the dislocation was reduced. Atlantoaxial dynamic test (B, C, D): the occipital bone was gradually raised with a height of 5, 10 and 15 cm separately to enable cervical flexion, then C-arm fluoroscopy was used to confirmed whether there was an anterior atlas dislocation (AAD) at each height.

Successful reduction was done by manual reduction showed in (A, B), then atlantoaxial dynamic test was performed. The occipital bone was gradually raised with a height of 5, 10 and 15 cm seperaterly to enable cervical flexion, C-arm fluoroscopy was used to confirmed whether there was an anterior atlas dislocation (AAD) at each height (C–E). Then, the patient was placed in a prone position with a neck collar, and the reduction was confirmed again by C-arm fluoroscopy (F).
After successful reduction, the atlantoaxial dynamic test was performed to confirm whether the transverse ligmant was intact(Fig. 2B–D). We gradually raised the occipital bone with a height of 5,10 and 15 cm separately to enable cervical flexion, C-arm fluoroscopy was used to confirmed whether there was an anterior atlas dislocation (AAD) at each height (Fig. 3C–E), no AAD was found in this patient which indicated that her transverse ligament was intact. Then, a neck collar was fitted, and the patient was placed in a prone position. Pedicle screw internal fixation was performed via a posterior approach without fusion. The procedure was performed successfully, and the patient was able to move out of bed on the first day after surgery with a Philadelphia cervical collar. During a 2-year follow-up period, lateral cervical spine radiography and sagittal reconstructions of CT scans (Fig. 4) demonstrated no instability of the atlantoaxial complex. The patient had no complaints of discomfort and refused to undergo surgical removal of the internal fixation.

Intraoperative lateral cervical spine radiography (A) and sagittal reconstructions of CT scans (B–D) 2 years after the operation demonstrated stability of the atlantoaxial complex.
DiscussionAtlantoaxial dislocation caused by odontoid process fracture accounts for approximately 10% ~ 15% of adult cervical spine fracture dislocations. Dislocation usually results from hyperextension trauma and is almost always accompanied by odontoid fracture and neurological symptoms. In most cases, patients with atlantoaxial dislocation die instantly4, 5. PAAD with intact odontoid processes, transverse atlas ligaments and atlases is very rare; the odontoid is angled posteriorly, and a mean of 13° makes such a posterior slip anatomically possible6, 7. Dislocation is usually caused by a high-energy injury. Most patients have a transient loss of consciousness. Patients present with or without pain and stiffness of the neck in Haralson dislocation3, 8. The mechanism is considered to involve hyperextension of the neck. Most patients are directly struck from the front, resulting in extreme hyperextension of the neck3, 8-12. Considering the course of injury in this case, it is suggested that the mechanism may be severe cervical hyperextension due to violence, accompanied by excessive longitudinal traction and upward displacement of the atlas. The anterior arch of the atlas was displaced posteriorly above the apex of the odontoid following injury of the ligament of the odontoid caused by rotational force.
There are two major methods for treating posterior atlantoaxial dislocation: closed reduction through skull traction and open reduction by operation. Compared with open reduction, closed reduction is more acceptable, and closed reduction for this kind of case is effective but dangerous due to the risk of neurological deficit and immediate death caused by overdistraction of the C1–C2 complex12-16. Song et al17 successfully reduced dislocations with occipital-mandibular leash traction without anesthesia. When skull traction fails, an odontoidectomy should be performed to reduce the dislocation9, 16, 18, 19. In some cases, skull traction and partial odontoidectomy were combined to reduce PAAD18, 20. Hu et al.18 reported that continuous skull traction results in symptoms of hypotension and bradycardia, so a transoral partial odontoidectomy was performed.
We chose to perform a manual reduction under general anesthesia because we have had successful experiences with more than 50 cases of manual reduction of lower cervical spine dislocations without neurologic deficits. We supposed that the reduction of dislocations is equivalent to a playback of the injury process, and if the spinal cord can withstand the traction of dislocations, it should be able to withstand the traction of reductions. The muscles relax after general anesthesia, and manual traction can provide greater forces and allow good control of the direction of force. Due to severe soft tissue and ligament damage, immediate intraoperative reduction can be easily performed without force.
After successful reduction, we developed a new method: the atlantoaxial dynamic test under general anesthesia to confirm the integrity of the transverse ligament. In this case, after successful reduction, we gradually raised the occipital bone from 5 to 15 cm to enable cervical flexion, and C-arm fluoroscopy was used to confirm whether there was an AAD, which indicated the integrity of the transverse ligament, which plays an important role in atlantoaxial stabilization. Rupture of the transverse ligament can lead to an AAD of 5 mm to 10 mm, and the dislocation will be greater when combined with other odontoid ligament injuries. Although MRI is a sensitive method for detecting the integrity of the transverse ligament, it is still difficult to determine the integrity of the ligament after trauma. If transverse ligament rupture is found, we are more inclined to consider fusion surgery instead of simple internal fixation. Our patient underwent pedicle screw fixation surgery without fusion. During a 2-year follow-up period, imaging data (Fig. 3) demonstrated no instability of the atlantoaxial complex. We recommended removal of the internal fixation for better range of cervical motion, but the patient had no complaint of discomfort and refused to undergo removal surgery.
ConclusionWe described a rare case of PAAD with mild neurologic deficits. It is suggested that closed manual reduction under C-arm fluoroscopy is a successful and safe method. Pedicle screw internal fixation via the posterior approach can provide sufficient stability. We confirm the integrity of the transverse ligament through the atlantoaxial dynamic test under general anesthesia has important significance for guiding the surgical plan.
留言 (0)