
記住我

Axis odontoid is a bony structure in the second cervical vertebra (C2). Due to its special morphological characteristics, the narrow odontoid has an extremely high incidence of fractures, especially in elderly patients, accounting for 60% of axis fractures and more than 10% of cervical fractures1-3. Of note, the incidence of odontoid fractures among elderly individuals is growing rapidly at a higher rate than the aging population4.
Recent treatment modalities that have established their efficacy in patients with odontoid fractures include conservative management and surgical intervention. Despite significant advances in internal fixation techniques in the past few years, the best treatment regarding operative or non-operative management for elderly patients remains elusive. In particular, conservative treatment aims to stabilize neck immobilization with an orthosis, including a halo-vest and a kind of cervical collar. Conservative treatment accompanied by external immobilization possesses the benefit of avoiding the risks of surgery; however, higher nonunion rates compare with that of surgical treatment5, 6. Conversely, surgical treatment intends to stabilize the fracture using screws and rods, and indications of surgical fixation are significant displacement and nonunion7, 8. Although this treatment exhibits better outcomes concerning the fracture union, it poses the risk of postoperative complications. Some risk factors responsible for fracture nonunion include patients aged more than 40 years, fractures displaced more than 5 mm, dorsally displaced fractures, and patients with neurologic deficits8. Therefore, many factors have to be considered in order to find the right balance between the merit of fracture consolidation and risks of surgical complications. The final decision for either adopting conservative or surgical treatment is made based on the above considerations.
According to the classification of Anderson9, odontoid fractures are classified as follows: (i) type I odontoid fracture involving the apex of the odontoid peg, which is widely recognized as a stable fracture and usually provided with cervical orthosis10; (ii) type II odontoid fracture involving the base of the dens, which has a high risk of nonunion due to the weaknesses of blood supply and is the main reason of traumatic atlantoaxial instability, therefore, this type of fracture needs to be treated with surgical fixation; and (iii) type III encompasses the odontoid and the lateral mass of C2. All odontoid fracture types can occur in any age population because of high-kinetic traumatism but primarily affect the aged population. Additionally, type II odontoid fracture is further characterized into three types, namely: type IIA—transverse fracture without displacement; type IIB—transverse fracture with displacement or fracture line is front up to back down; and type IIC—comminuted fracture or fracture line is from front down to back up. Notably, type IIC refers to an unstable fracture with a high nonunion rate and patients with this type of odontoid fracture are prone to long-term complications after conservative treatment.
Surgical fixation options for odontoid fractures include anterior or posterior approaches8, 11. Those patients, whose fracture line is from front down to back up or with a small odontoid caster angle, are not suitable for anterior odontoid screw fixation, and thus are often treated with cervical posterior fixation fusion. Many posterior stabilization techniques have been used for fixation of the atlantoaxial complex, such as wiring methods, transarticular atlantoaxial (C1–C2) screw technique, axial (C2) pedicle screw technique, and C2 translaminar screws. Various techniques have been shown to exhibit different advantages and disadvantages. For example, posterior wiring methods are technically simple and safe procedures but have high failure rates in fusion12, 13. The transarticular C1–C2 and C2 pedicle screw techniques provide high fusion rates, but it is highly possible to damage important adjacent tissues and organs, such as the vertebral artery, particularly for patients with vertebral artery abnormality or atlantoaxial deformities14, 15. To provide stable internal fixation with minimal damage to the vertebral vessels, Wright proposed the C2 translaminar screw technique for adult patients, while Leonard recommended the same technique to pediatric patients16, 17. However, the Wright's technique has been associated with some complications, including partial dorsal laminar breach, spinal canal violation with screws especially for patients with small lamina, and early hardware fracture18. There have been several attempts by many researchers to address these issues. Unfortunately, no matter how much we improve Wright's technology or turn to other assistive technologies, there are still plentiful drawbacks19-23. For example, the three-dimensional fluoroscopy-based image guidance technique as an assistive technology requires expensive equipment and complex operation. In this regard, it will be of great significance to provide a simple and safe technique to modify axial translaminar screw fixation.
In this study, all patients with type II odontoid fractures were fixed with an atlas pedicle or lateral mass screw combined with a modified axial translaminar screw. We collected clinical data retrospectively. The present study aimed to: (i) describe a modified axial translaminar screw fixation to guarantee the accurate placement into lamina and avoid placement into spinal canal; (ii) evaluate the feasibility of this surgical treatment; and (iii) analyze its advantages and disadvantages.
Methods Patient SelectionAll patients included in the study provided informed consent. This research was approved by the Ethics Committee of The Second Affiliated Hospital of Wenzhou Medical University and was performed following the Declaration of Helsinki principles.
Eligible patients were enrolled between March 2016 and June 2018. Inclusion criteria included: (i) patients previously without neurological symptoms; (ii) patients with type II odontoid fractures; (iii) CT 3D reconstruction and MRI examination to demonstrate the feasibility and safety of the operation; (iv) received modified axial translaminar screw fixation; and (v) patients with active follow up. In addition, exclusion criteria included patients with: (i) previous cervical diseases or neurological symptoms; (ii) cervical infection or tumor; (iii) serious osteoporosis; and (iv) types I or III odontoid fractures. After applying the exclusion criteria, 23 patients were included in this study.
Surgical ProceduresSurgery was performed under general anesthesia. Patients were placed in a prone position with the head held in place using a U-shaped head holder. Then, a neutral position was maintained to expose the posterior cervical spine. From the lower margin of the occipital protuberance, a 7-cm longitudinal median incision was cut to fully separate and expose the posterior arch of the atlas and lateral mass. Meanwhile, the axial lamina, spinous processes, and zygopophysis were exposed.
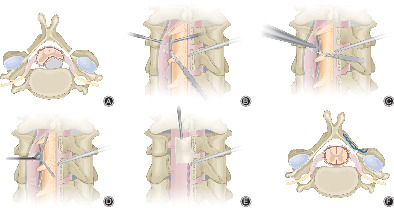
All fracture patients were fixed with atlas pedicle screws or lateral mass screws coupled with axial translaminar screws. For fixation of C2, this study applied the modified axial translaminar screws fixation technique (Fig. 1). A high-speed drill was used to generate a small “entry” cortical point at the junction of the axial spinous process and the lamina close to the rostral margin of the axial lamina. At the same time, we used the same drill to dig a small cortical “window” in the middle of the axial contralateral lamina. A curet was used to scrape cancellous bone as far as possible, but not to damage the inner plate. Subsequently, a hand drill was used from the “entry” cortical point to the contralateral lamina. Through the cortical “window” in the middle of the axial lamina, the direction of the hand drill could be adjusted reasonably, parallel to the lamina. Finally, bone screws of 26 - 30 mm in length and 3.5 mm in diameter were inserted. To achieve the interactive placement of screws, one was implanted into the upper position, while the other one was implanted into the lower position. In this technique, screws in the lamina were visualized to prevent incorrectly implanting the posterior spinal canal through the visualized “window.”

Schematic diagram of modified axial translaminar screw fixation. (A) Normal axis. (B) A high-speed drill used to generate a small “entry” cortical point at the junction of the axial spinous process and lamina. (C) A high-speed drill used to dig a small cortical “window” in the middle of the axial contralateral lamina. Cancellous bone was removed while the inner lamina was preserved. (D) Axis with an “entry” and a cortical “window.” (E) A thin pedicle finder that can be directly visualized through the unicortical “window.” (F) A screw that can be directly visualized through the unicortical “window.”
After the bone screws were successfully placed on the lamina, then they were connected and fastened by use of an appropriate connecting rod. The cortical bone of the lamina, spinous process, and posterior arch of the atlas was removed with a grinding drill, whereas the cancellous bone of the posterior superior iliac spine was cut into pieces and eventually placed on the posterior surface to achieve fusion.
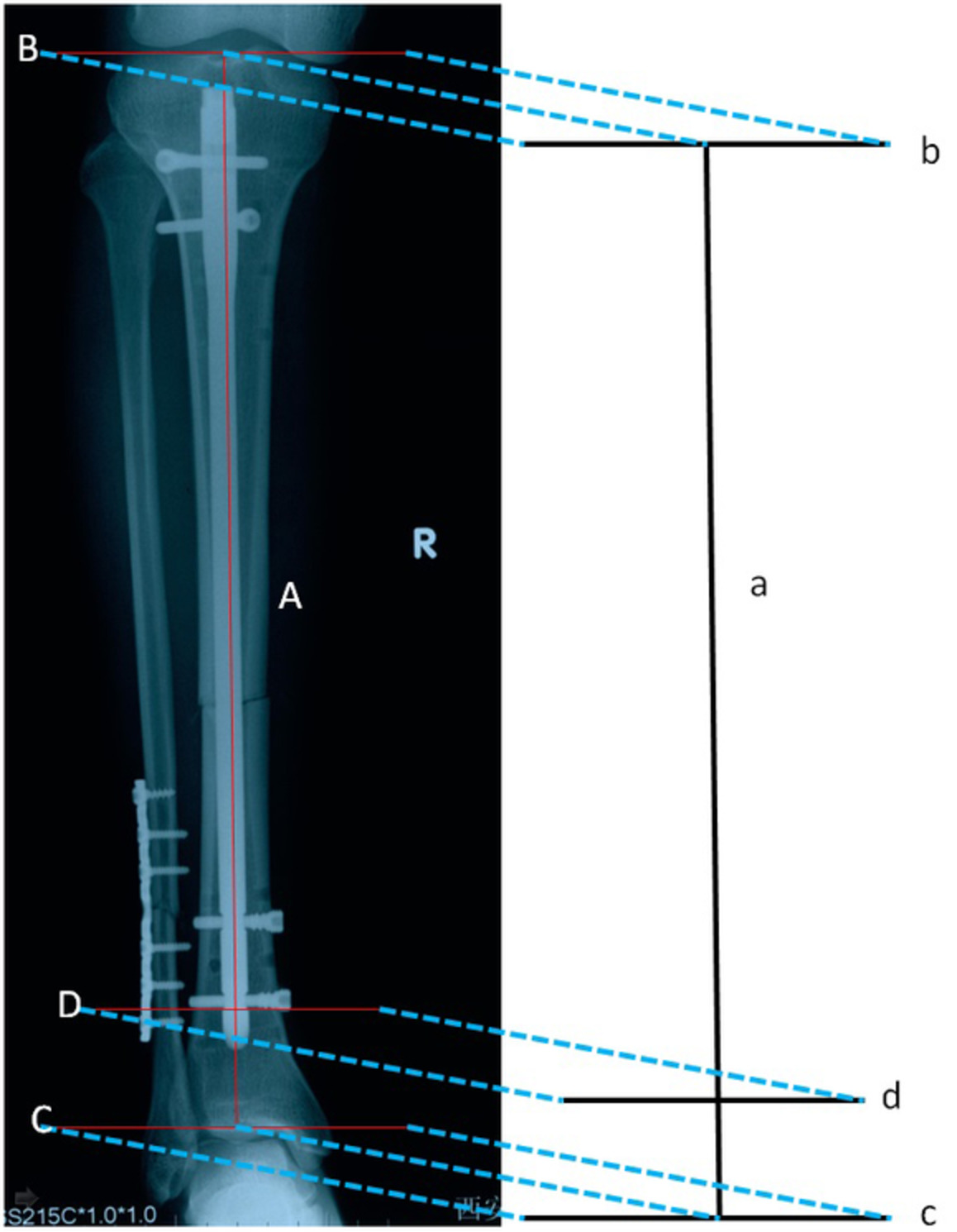
Parameter Measurement and Clinical Assessment Screw Angle (SA)Using a modified technique, the screw angle (SA) was measured for screw placement, which was similar to that of Wright's technique. The SA for the modified technique was traced on both sides, with one of the lines inside the C2 lamina parallel to the screw, while the other passed through the spinous process and odontoid process, dividing the vertebrae into two hemivertebrae (Fig. 2). The purpose of SA was to guide the direction of screws for the modified technique. Participants were asked to complete two related questionnaires before surgery and during follow-up.

Screw placement of modified Wright's technique. (A) The measurement of screw angle in the preoperative imaging. (B) The screw placement in postoperative imaging.
Neck Disability Index (NDI)Neck Disability Index (NDI), a self-report questionnaire, was designed to examine neck pain and the effects of functional activities. Specifically, the questionnaire consisted of 10 sections, including clinical features and daily living: pain intensity, personal care, lifting, reading, headaches, concentration, work, driving, sleeping, and recreation. Each item is scored from 0 (no disability) to 5 (total disability).
Visual Analogue Scale (VAS)For this study, the VAS score system was used to measure neck pain levels24. The items of VAS pain scores range from 0 to 10 as follows: 0 mean painless; 1–3 (mild pain); 4–6 (patients can tolerate pain); and 7–10 (the pain cannot be endured).
The above questionnaires were assessed in preoperatively and at 1, 6, and 12 months postoperatively. Additionally, estimated blood loss, operative time, length of stay, wound infection, and hemoglobin were documented.
Statistical MethodsStatistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). All P-values are two-sided; P values <0.05 were considered statistically significant.
Results Demographic DataA total of 23 patients with type II odontoid fracture received the modified axial translaminar screw fixation in this study. The mean age and BMI were 54.3 ± 11.1 years and 22.6 ± 2.4 kg/m2, respectively (Table 1). The number of male patients was almost equal to that of female patients (12 men to 11 women). Coronary disease, hypertension, and diabetes mellitus accounted for 3.1%, 30.4%, and 13.0%, respectively. Most notably, there were no patients with neurological deficiency.
TABLE 1. Demographic characteristics and surgery-related factors of patients with odontoid fracture Characteristics Value Subjects (cases) 23 Age (years, mean ± SD) 54.3 ± 11.1 Sex (male/female) 12/11 BMI (kg/m2, mean ± SD) 22.6 ± 2.4 Coronary disease (cases [%]) 2 (3.1) Hypertension (cases [%]) 7 (30.4) Diabetes mellitus (cases [%]) 3 (13.0) Neurological deficiency (cases [%]) 0 (0.0) Parameters Measurement and Clinical Assessment Parameters MeasurementDuring the operation, screws (length, 26 - 30 mm) were inserted accurately in all patients without bony breach. The mean screw angle was 56.1° ± 3.0° (Table 2).
TABLE 2. Operative and postoperative features of patients with odontoid fracture Characteristics Value Screw angle (°) 56.1 ± 3.0 Operative time (min, mean ± SD) 102 ± 28 Operative EBL (mL, mean ± SD) 50 ± 25 Operative hemoglobin (g/dL, mean ± SD) 12.0 ± 1.4 Bony breach 0 Wound infection 0 Length of stay (days, mean ± SD) 10.4 ± 3.4 EBL, estimated blood loss. Operative AssessmentThe modified internal fixation technique was completed successfully without using fluoroscopy. More importantly, we observed no significant surgical and technical complications, such as bony breach, spinal cord injuries, vertebral vascular injury, and nerve root injuries. Estimated blood loss and operative time were 50 ± 25 mL and 102 ± 28 min, respectively (Table 2).
Postoperative AssessmentThe length of stay and postoperative hemoglobin were 10.4 ± 3.4 days and 12.0 ± 1.4 g/dL, respectively (Table 2). Since the surgical time was similar to that of the traditional technique, no wound infection occurred among patients. Moreover, patients were followed up for 12 to 32 months, with an average time of 14.7 months. Postoperative roentgenographs showed that the fixation screws were all accurately located in the lamina with no internal fixation displacement, loosening, or breakage. With the increase of follow-up time, NDI and VAS revealed that the symptoms of neck pain and the limitations of functional disability were significantly improved (Fig. 3).

Measurements of visual analog scale (VAS) scores (A) and neck disability index (NDI) scores (B) for patients with modified axial translaminar screw fixation during follow-up. * = P < 0.05 compared with the previous follow-up time.
Postoperative ComplicationsWe identified no serious surgical complications and atlantoaxial instability during the follow-up (Figs 4-6). Although cervical rotation was slightly limited, flexion and extension were not significantly limited. Lastly, all patients were satisfied with the treatment outcome.

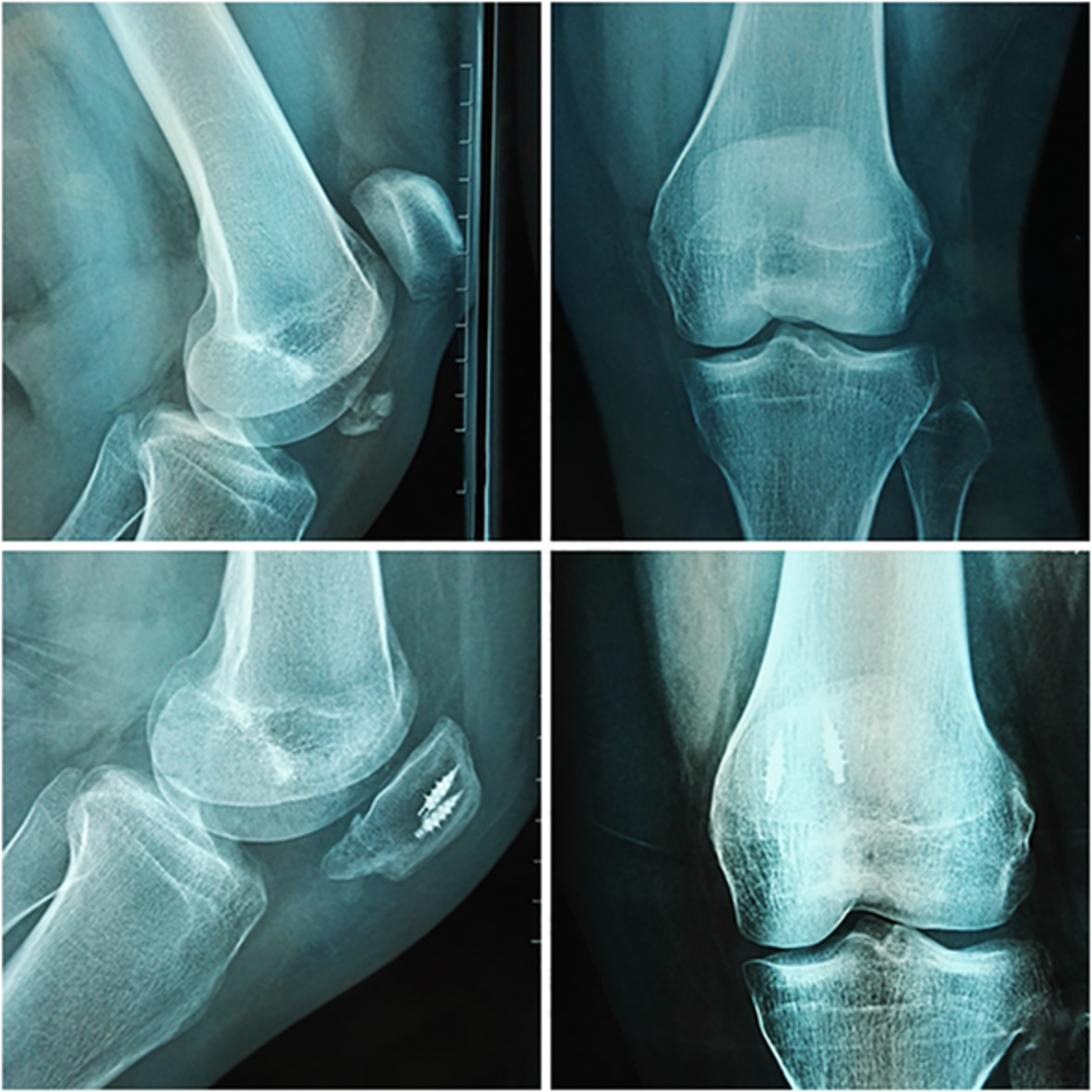
Imaging data of a typical case. Male, 51 years old, with Anderson II A odontoid fracture, treated with atlantal lateral mass screw combined with bilateral modified axial translaminar screws and bone graft fusion. (A, B) Preoperative X-ray and CT showed odontoid fracture type II A. (C, D) Postoperative roentgenographs showed screws were in good position. (E) Postoperative CT showing that odontoid fracture healed after 3 months postoperatively.

Male, 50 years old, with Anderson II B odontoid fracture, treated with atlantal lateral mass screw combined with modified bilateral axial translaminar screws. (A) Preoperative CT showed type II B odontoid fracture. (B, C) Postoperative X-ray demonstrated that screws were in good position. (D) Intraoperative imaging. (E) Postoperative CT showed odontoid fracture healed after 3 months postoperatively.

A 45-year-old woman with Anderson II A odontoid fracture. (A) Preoperative CT showed odontoid fracture II A. (B, C) Postoperative roentgenographs showed screws were in good position. (D) Postoperative CT indicating that the odontoid fracture healed after 3 months postoperatively.
DiscussionThe morphological characteristic of the odontoid is long and narrow, and the thin cortical bone exhibits a high risk of fracture. The incidence of odontoid fractures in the elderly population has been estimated to account for 50% of cervical fractures25. According to Grauer–Anderson classification9, 26, odontoid fractures can be classified into three types, namely, types I, II, and III. In particular, types I and III are stable fractures, whereas type II is recommended for surgery due to a higher incidence of odontoid fractures, up to 65%27.
Technical NoteFor this study, 23 patients with type II odontoid fracture treated with modified axial translaminar screw fixation were selected. We subsequently designed a surgical treatment method of atlas pedicle screws or lateral mass screws integrated with modified axial translaminar screws. There was no special technique for atlas screw fixation. The screw direction and placement were similar to those of the traditional technique. We only added a small cortical “visualize” window in the midpoint of the lamina, and thus translaminar screws in the lamina were visualized to prevent incorrectly implanting the posterior spinal canal through the visualized “window.”
EvaluationOverall, 46 bone screws were accurately inserted into the axial lamina without fluoroscopy in this work. The length of all axial laminar screws was between 26 and 30 mm. During the operation, the vertebral artery and spinal cord were uninjured. Likewise, the rear structures such as the spinous process, posterior ligament of the spinous process, and interplate of the lamina were undamaged. These findings suggest that there are no serious complications associated with this technology during the study period. Postoperative follow-up showed no atlantoaxial joint instability, screw fracture, or dislocation. More interestingly, fracture healing was satisfactory in all patients. Cervical rotation was slightly limited, but flexion and extension were not significantly limited.
AdvantagesCervical posterior fixation fusion for odontoid fractures includes pedicle screw fixation, Wright's technique, and modified Wright's technique. Pedicle screw fixation requires a high level of surgical skills because of its complex anatomic structure. For some patients with abnormal pedicle or vertebral artery variation, this technique is more likely to damage the vertebral artery, and thus it may be no longer applicable. To avoid this possible risk during screw placement, Wright et al. first proposed a relatively simple axial translaminar screw fixation technique in 200417. They used this technique to complete all posterior operations without any complication related to the operation and technique, such as vertebral artery injury or spinal cord injury. This technique has recently been widely advocated by spinal surgeons, but it is difficult to overcome the risk of invasion of the spinal canal and even the cervical spinal cord21.
In order to effectively avoid these risks and accomplish accurate screw placement, several studies have tried to modify this technique. For instance, Jea et al. (2008) argued that to achieve directly visualized screw placement, a cortical “exit” window needs to be added based on Wright's technology, but the entry point remained unchanged21. However, the length of bone screws required by this technique was significantly shorter compared with that of Wright's method, and the overall stability point of the axis was slightly shifted backward, changing the original stability of the vertebral body. In addition to adding “exit” windows at the facet-laminar junction, there was an inevitable risk of damage to the dorsal cortex during screw channel preparation or screw placement. Kabir et al. subsequently proposed another modified technique that could effectively avoid cortical destruction, which required removing the spinous process of the axis and then using the base of the removed spinous process as the entry point to complete screw placement22. Following this technique, it was suitable for patients with the destruction of the lateral mass of the axis and also those with a unilateral high-riding vertebral artery. Nevertheless, this technique was accompanied by two disadvantages. First, it inevitably destroyed important structures at the back of the spinous process (including ligaments) in the axial vertebra, leading to a significant reduction in biomechanical properties. Second, the narrow spinous process was unable to accommodate the two lamina screws, hence bilateral translaminar screw placement was impossible. Elsewhere, some scholars used some auxiliary equipment and new technologies to reduce the risk of screw invasion into the spinal canal. Nottmeier et al. reported their experience with placement of axial laminar screws using three-dimensional (3D) fluoroscopy-based image-guidance19. Although to some extent this image guidance technology can assist the surgeon to place the screws accurately, it extended both operation and radiation exposure time, while at the same time, the expensive equipment and complex operation made it difficult to popularize. Sai Kiran et al. and Englert et al. purported to place axial screws under the guidance of intraoperative fluoroscopy. Even though this technique was effective with only off-the-shelf equipment, radiation exposure to operators and patients was still inevitable23, 28.
In summary, many studies have attempted to modify the axial translaminar screw fixation or use auxiliary equipment, but the drawbacks are plentiful.
LimitationsDespite these promising results, the present study has some limitations. First, due to a limited number of cases, we were unable to compare the clinical data between modified surgery and traditional surgery, which need rigorous controlled studies to be performed. Second, this modified technique required a cortical window in the middle of the lamina, which would inevitably damage a small part of the lamina cortex; thus, whether the biomechanical properties would be affected needs further inquiry. Third, more cases and long-term clinical follow-up are necessary to assess the long-term stability of the hardware and fusion rates. Fourth, our new technique was not exclusively investigated for some special patients, such as those with unilateral high-riding vertebral artery or advanced rheumatoid arthritis undergoing occipitocervical fusion, which should be considered in future research.
ConclusionThe findings of this study indicate that the modified axial translaminar screw fixation for odontoid fracture exhibits the disadvantage of accurate screw placement. Compared with the previous modified technique, it possesses the benefits of less soft tissue dissection, simple operation, and no fluoroscopy. Moreover, compared with Wright's technique with the help of auxiliary equipment, this technique has less time of operation and needs no expensive devices and cumbersome technologies.
DeclarationAll authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors and all authors are in agreement with the manuscript.
AcknowledgmentsThis work is supported by grants from the National Nature Foundation of China (Grant no. 81871806).
留言 (0)