
記住我

In 1927, Foerster first reported the successful fusion of occipitocervical junction with autogenous fibula transplantation. Since then, occipitocervical fusion has made remarkable progress. However, considering the complex anatomic structure and adjacent significant neurovascular structure in this region, the concept and technique still have challenges1. At present, posterior segmental fusion was preferred due to desired stability2; nevertheless, complication occasionally occurs as the number of surgeries in the upper cervical region is increasing3. As reported, revisions might be more than expected due to limited improvement after initial surgery and postoperative complications, such as screw loosing, connecting rod fracture, bone graft nonunion, and secondary dislocation, among others. Under the circumstances, conventional occipital unicortical screws might lack pullout strength. In addition, revision surgery in occipitocervical area was demanding, considering objective factors including existing bone graft, scar formation, and changes in anatomical marks. Until now, there is a lack of uniform standard for revision surgery and surgeons rely more on personal experience and preference. We reviewed a cohort of successful revision surgeries utilizing the modified technique of occipital plate and bicortical screws for failed craniovertebral junction stabilization.
Materials and Methods Patient SelectionThe present study was approved by the local ethics committee. Informed consent was obtained, and all patient data were made anonymous and kept confidential.
Inclusion criteria were as follows: (i) posterior upper cervical fusion was performed preliminarily, and then was diagnosed as occipitocervical instability or failure of internal fixation after the initial operation by clinical and radiographic evaluation; (ii) CT examination was performed to measure the thickness of the external occipital protuberance and 15mm below it. The depth and feasibility of bicortical purchase were confirmed. Exclusion criteria were patients with infection, tuberculosis, or tumor. A total of 12 consecutive cases of occipitocervical revision surgery from October 2010 to May 2018 were analyzed retrospectively. All cases were followed up, including five males and seven females range from 24 to 62 years at the initial operation (average, 41.17 ± 11.42 years). The interval time between initial and revision operation was 3–156 months (average, 40.42 ± 50.79 months). All patients had varying degrees of cervical and occipital pain, of which 11 cases (91.67%) were associated with spinal cord nerve dysfunction. Nine cases had failed internal fixation (six cases of occipital screw loosening, two cases of lamina wire fracture, one case of connecting rod fracture), three cases of secondary dislocation (one case of C1-2 Brooks wire fixation, two cases of C1-2 screw rod fixation) (Table 1).
TABLE 1. Patient demographic and clinical outcome data Case no. Sex First surgery Revision surgery JOA VAS Follow-up (mo) Complication Age (yrs) Surgical protocol Surgery Interval (mo) Diagnosis Surgical protocol Preop Postop Preop Postop 1 M 34 PRW(C1-2) 156 IF+OCI+BGN PRIF(C0-3) 10 14 6 4 18 None 2 M 37 PPW(C0-4) 34 IF+OSL+OCI PRIF(C0-5) 11 13 8 3 24 None 3 M 62 PPW(C0-2) 13 IF+OSL+OCI PRIF(C0-2) 6 11 8 4 24 None 4 F 31 PRW(C1-2) 146 IF+WF+OCI+BGN PRIF(C0-4) 8 11 7 2 32 None 5 M 45 PPW(C0-5) 24 IF+OSL+OCI PRIF(C0-5) 6 12 4 0 26 None 6 F 50 PSR(C1-2) 3 IF+OSL+OCI+BGN PRIF(C0-2) 7 10 7 2 30 None 7 F 29 PPW(C0-2) 37 IF+OSL+OCI PRIF(C0-3) 10 16 5 0 24 None 8 F 52 PPW(C0-2) 12 IF+OSL+OCI PRIF(C0-2) 8 12 6 3 24 None 9 M 39 PPW(C0-3) 14 IF+CCF+OCI PRIF(C0-3) 6 13 5 3 24 None 10 F 34 PSR(C1-2) 6 BA+OCI+BGN PRIF(C0-2) 7 11 5 1 21 None 11 F 57 PSR(C1-2) 5 BA+OCI+BGN PRIF(C0-2) 9 13 6 1 14 Superficial infection 12 F 24 PRW(C1-2) 35 IF+WF+OCI+BGN PRIF(C0-4) 15 16 7 2 28 None Mean ± SD — 41.17 ± 11.42 — 40.42 ± 50.79 — — 8.58 ± 2.53 12.67 ± 1.84* 6.17 ± 1.21 2.08 ± 1.32* 24.08 ± 4.70 — AAD, atlanto-axial dislocation; BA, basilar invagination; BGN, bony graft nonunion; CCF, fracture of connecting rod; IF, instrument failure; OCI, Occipitocervical instability; OSL, occipital screws loosening; PPW, Posterior plate-screw instrument; PRIF, posterior reduction and instrumented fusion; PRW, Posterior rod-wire instrument; PSR, Posterior screw-rod instrument; WF, wire fracture. Surgery PreparationRadiological evaluations included X-ray plain films, CT with three-dimensional (3D) reconstruction, and magnetic resonance imaging (MRI). To determine the feasibility and depth of inserting bicortical screws, 3D-CT scans were used to confirm the thickness of the external occipital protuberance and 15 mm below (Table 2).
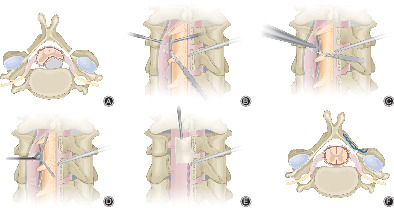
TABLE 2. Clinical symptoms Parameters Preoperative no. (%) Postoperative improvement no. (%) Occipital or neck pain 12 (100) 12 (100) Extremity weakness 11 (91.7) 10 (90.9) Sensory of paresthesia 10 (83.3) 10 (100) Bladder dysfunction 5 (41.7) 4 (80) Gait disturbance 5 (41.7) 5 (100) Operative TechniqueAll patients underwent general anesthesia in supine position. After routinely sterilized, the autogenous iliac bone was harvested and changed to prone position. A posterior midline incision was made that extended from the site 2 cm above the occipital protuberance to the target spinal process. The paraspinal muscles and previous scar tissue was dissected carefully. The initial failed internal fixation and nonunion bone graft were removed. The scar formation between the previous occipital plate and the occipital was meticulously dissected to expose the region. The occipital plate was placed on the surface of protuberance. The feasibility of screws was ascertained according to preoperative measurements. The pilot hole was created by a high-speed burr. After that, the trajectory was deepened perpendicular to the external occipital protuberance for the specified depth with a depth-limited drilling, 2 mm away from the internal bone plate; meanwhile, a probe was used to explore all the walls of the trajectory in case of penetration. Then, the trajectory was deepened at intervals of 1 mm with depth-limited drilling each time and subsequently a probe was used to explore all the walls of the trajectory, until penetrating the internal bone plate (Fig. 1) Two or three bicortical screws in vertical rows, which were determined by the thickness of the occipital region, were inserted to the occipital plate and the depth of penetration was less than 2 mm from the internal bone plate. Two appropriate titanium rods were preflexed and used for connection bilaterally. When the rods were fixed, the pull-out strength could reconstruct the alignment. An iliac crest graft was modified to implant on the posterior rim of occipital and C1-2. The conventional radiograph was used to confirm the direction of the trajectory and the occipitocervical sagittal alignment. After this period, all patients were routinely treated with anti-inflammation, detumescence, and nutritional nerve therapy. The drainage tube was removed when there was no cerebrospinal fluid leakage or the drainage fluid was less than 50 mL per 24 h. The cervical brace was maintained for at least 6 weeks.

Illustration of revision surgery: (A) Firstly, the trajectory was deepened for the specific depth with a depth-limited drilling, 2 mm away from the inner occipital table. Meanwhile, a probe was used to explore all the walls of the trajectory in case of penetration. (B) The path was drilled with depth-limited drilling at intervals of 1 mm each time until reaching the internal bone plate, and a probe was used subsequently. (C) Bicortical screws were inserted to the occipital plate and the depth of penetration was less than 2 mm from the internal bone plate. (D) Posterior view of instrument.
EvaluationX-ray, 3D-CT, and MRI examinations were performed before the operation and during the follow-up to observe the instruments, graft, reduction, and stability. VAS score (10 score)4 was used to compare the pain intensity and JOA score (17 score)5 was assessed to evaluate the improvement of neurological function. We defined bony fusion as no absorption or translucent line around graft, no instrument failure, and no movement under dynamic radiograph.
Visual Analog Scores (VAS)As a common method to measure subjective pain perception of patients, VAS was used to evaluate pain intensity. A score of 0 indicates no pain at all, while 10 indicates the most excruciating pain.
Japanese Orthopaedic Association Scores (JOA)JOA score is a principal outcome measure used in the management of cervical spine disorders, and to assess functional status in routine clinical practice. The JOA score of the cervical spine includes upper limb motor function (4), lower limb motor function (4), sensory function (6), and bladder function (3), with a total score of 17. The higher the score, the better the neurological function.
Statistical AnalysisAll statistical analysis were performed using SPSS 22.0 and data were expressed as mean and standard deviation. The statistical differences among the JOA and VAS before and after revision surgery were determined by paired-sample t test. P < 0.05 was considered to have statistical significance.
ResultsAll surgeries were performed by the same senior surgeon. A total of 12 patients underwent posterior occipitocervical revision surgery with bicortical screws and occipital plate. The data showed that the occipital at the site of external occipital protuberance was the thickest. The thickest external occipital protuberance was 15.49 ± 1.47 mm and decreased gradually on the midline to 13.41 ± 1.60 mm at below 15 mm. Five cases underwent fusion level at C0-2, three at C0-3 fusion, two at C0-4, and two at C0-5. The operation time ranged from 180–320 min (average 217.50 ± 40.49 min) and the intraoperative blood loss was 400–2200 mL (average 754.16 ± 482.81 mL). All patients were followed up for 14–32 months (average 24.08 ± 4.70 months). During the follow-up period, all patients showed good internal fixation and solid bony fusion was achieved. At the final follow-up, JOA score increased from 8.58 ± 2.53 before surgery to 12.67 ± 1.84, and VAS score improved from 6.17 ± 1.21 to 2.08 ± 1.32. Significant improvements in VAS and JOA were established at the last follow-up visit (P < 0.05) (Table 1). Clinical symptoms were relieved in all patients after revision surgery (Table 2). No perioperative complications occurred, such as cerebrospinal fluid leakage, instrumentation failure, neurological deterioration, or vascular injury. However, superficial surgical site infection was observed in one patient, which healed after intermittent debridement and antibiotics.
As shown in Fig. 2, a 37-year-old man underwent posterior occipitocervical fusion and fixation surgery (C0-5) on 17 November 2014 and was admitted to our clinic on 12 September 2017. The chief complaint was sensation of soreness in occipital and neck accompanied by numbness in left forearm for 1 month. Preoperative X-ray and CT showed the occipital screws loosening. Then, a revision surgery utilizing bicortical screws and occipital plate was performed. Postoperative X-ray at 3 month follow-up showed rigid internal fixation and postoperative CT at 2-year follow-up after surgery showed rigid internal fixation and bone fusion (Figs 3, 4).

Case 2, a 37-year-old man underwent posterior occipitocervical revision surgery (C0-5) utilizing bicortical screws and occipital plate. (A–C) Preoperative X-ray and MRI showed the occipital screws loosening and compression of the spinal cord. (D) Preoperative CT showed distinct pullout purchase. (E) Postoperative X-ray showed screw position was accurate. (F–H) Postoperative CT at 2-year follow-up showed rigid internal fixation and bone fusion.

Case 5, a 45-year-old man treated with bicortical screws and occipital plate revision surgery (C0-5). (A, B) Initial surgery images showed unicortical screws was used. (C) Postoperative X-ray after initial surgery showed occiput screws loosening without spinal cord compression. (D, E) Modified technique of bicortical screws and occipital plate system and postoperative CT at last follow-up showed rigid internal fixation and complete decompression of spinal cord.

Case 9, a 39-year-old man treated with bicortical screws and occipital plate revision surgery (C0-3). (A, B) CT scan showed an occipital protuberance with sufficient thickness and a relatively thin occipital squama. (C–E) Preoperative CT showed fracture of connecting rod after initial surgery with unicortical screws. (F) Modified technique in postoperative CT at last follow-up and screw was in ideal position.
DiscussionOccipitocervical instability is a life-threatening structural instability of the region followed by a series of neurological deficiencies, which could be caused by various pathological conditions such as congenital malformation, trauma, infection, tumor, rheumatoid arthritis, and degenerative diseases. It is crucial to reconstruct the normal anatomical relationship of occipitocervical junction and restore its stability as soon as possible6. As the most complex spinal structure, the occipitocervical junction has the maximum activity and remains stable simultaneously, not to mention the significant location adjacent to the medulla oblongata. Besides, the medial side of the occipital bone is adjacent to the dura mater, dural sinus, and occipital lobe. Based on this, it was once known as the “surgical restricted area,” which was difficult to operate on. Researcher proposed that the ideal craniocervical stabilization system should meet the following conditions7: (i) to provide rigid segmental stability; (ii) to avoid invasion of the spinal canal; (iii) to provide orthopaedic stability until bone fusion without the assist of an external fixator; (iv) to provide stability even when the posterior tissue and occipital plate are defective or injured. With the development of internal instruments, wires, screws, rods, and plates had been used with their respective characteristics8-10. However, a few complications occurred, such as failure of internal fixation, bone graft nonunion, and poor prognosis. At present, there is a lack of studies concerning revision surgery for failed craniovertebral junction stabilization.
Grob11 first proposed and applied the inverted Y-shaped plate, which achieved effective 3D fixation in biomechanics. Additionally, occipital plate-screw system was proved to be the most reliable fixation technique12, 13 with diverse failure rate of 6.7%–26.67%2, 14 in previous studies. Notably, the commonly used occipital monocortical purchase available was 12 mm, mostly considering the thickness of the occipital plate and the safety in depth of occipital screws. Nonetheless, shorter occipital screws and longer connecting rods compared to other techniques tended to produce greater shear force, which may disperse the fixation points and cause a risk of internal fixation failure, especially for the long length of implant. Thus, clinical efficacy and safety of the modified technique utilizing the occipital bicortical screws and plate approach were evaluated. In this study, all patients were treated with two or three bicortical screws and the inverted Y-shaped plate, combined with subaxial pedicle screws fixation. During the follow-up period, bone fusion was found in all cases and there were no complications such as failure of internal fixation and vascular injury. Previous study showed that the mean bone thickness of the external occipital protuberance was 14 mm, which was the thickest in this region adjacent to the superior nuchal line. The thickness decreases sequentially from the external occipital protuberance to the upper and inferior regions, and the thinnest part was about 5.7 mm15. Therefore, several scholars advocated the use of unicortical screws in the site of external occipital protuberance and the trajectory was the best in stability and safety perpendicular to the surface of the protuberance16. To avoid damaging the cerebral tissue and occipital venous sinuses, Ebraheim16 suggested that the direction of the trajectory should be towards the center of the protuberance. In the present study, the instruments failed to achieve long-term stability for the initial operation. The consensus is that the pullout strength was positive correlative to the screw length biomechanically. Consideringthe requirement for more rigid fixation of resurgery and insufficient resistance to pull out of unicortical screws, we recommended the vertical placement of bicortical screws with superior pull-out strength in revision surgery. During the procedure, depth-limited drilling was utilized for the sectional drilling and the trajectory was deepened 2 mm away from the internal bone plate during the first stage, and then drilled at an interval of 1 mm until reaching the internal bone plate. Meanwhile, a probe was used to explore all the walls of the trajectory. The above procedure mostly guaranteed the safety of the operation. Based on our clinical experience, the depth of the screw could penetrate the inner occipital plate within 2 mm, owing to the interval space between the inner occipital table and the skull periosteum. Additionally, the skull periosteum has a degree of toughness. In the process, the operation should be conducted gently and meticulously to ensure safety.
Generally, the main reason for the instrument failure came from persistent segmental instability17, in which the downward shift of stress caused by long segment fixation may be one of the significant reasons. Until now, it there has been a consensus that bony fusion was the goal of occipitocervical surgery17. In the present study, bony fusion was not achieved after initial surgery in six cases, which may be an important cause of instability. Similarly, the internal fixation system without bone graft made it hard to achieve bone fusion in the real sense, and the stability depending on metal implant, which inevitably had a higher risk of fixation fatigue. It was well-accepted that the role of the internal fixation instrument contributed within a few weeks after the operation, after which the role of the graft in stabilizing the area was replaced by bone fusion.
Cappuccio et al.18 suggested the segment fixation irrespective of the range of motion should be considered in adult patients with spinal degeneration. In fact, the range of motion of the upper cervical spine, especially extending activity, was significantly decreased with increasing age19. Thus, there would be no significant clinical difference owing to the decrease of postoperative range of motion. Furthermore, considering the risk of instability, the difficulty of revision surgery, and the complex physical conditions of elderly patients, posterior plate-screw technique with desired biological performance was preferred20, 21. On the contrary, wire technique or short segment fixation preserving activity was more suitable for the pediatric population22. In summary, rigid internal fixation was the primary consideration. In our study, two patients with atlantoaxial segmental fixation had secondary dislocation, which indicated that the previous treatment of occipitocervical instability with basilar invagination was inadequate, resulting in incomplete reduction and potential risk of vertical dislocation23, 24. Although the underlying pathological mechanism of basilar invagination remained to be further studied, it was well-described that patients with basilar invagination may encounter secondary vertical dislocation of odontoid process due to atlantoaxial reduction and fixation alone3. As such, occipitocervical fusion extending to occipital bone is necessary.
The status of the graft could be determined directly in terms of radiology; however, revision surgery still requires comprehensive consideration of clinical symptoms and neurological function. In this study, all patients had varying degrees of cervical and occipital pain, of which 11 cases (91.67%) were associated with spinal cord nerve dysfunction. Combined with radiological instability factors, there were clear indications for revision surgery. Of note, Goel17 reported 30 cases of craniovertebral revision, among which 17 cases were accompanied with progressive neurological symptoms, had no graft failure or abnormal dynamic radiographs, and the symptoms were improved after posterior fusion. This suggested that neurological symptoms may be related to persistent minor instability without explicit evidence from radiology25.
Revision surgery in the occipitocervical region was demanded due to existing graft, adhesions, and scar formations. Artificial anatomic changes caused by decompression and bone transplantation also led to plenty of problems in surgical exposure, separation and placement of new fixations. Besides, the longer the interval between operations, the more difficult the operation wound be. Overall, surgeons must have rich experience in upper cervical spine surgery and revision techniques to make them as effective, simple, and safe as possible. In recent years, occipital plate-screw and occipital condylar screw were discussed widely. Among them, the new technology of integrated occipital plate and connecting rod had been applied. However, it required more complex bending for adapting to the shape of the skull. The larger occipital plate might even hinder the placement of the atlantoaxial screws. Furthermore, the occipital screw placement is located on both sides of the midline where the bone is thinner compared with the external occipital protuberance; thus, there may be a slight deficiency in biomechanical properties. Occipital condylar screws have been reported on in the last few years as directly fusing the joints with short segmental fixation, and the biomechanical properties were seen as satisfactory17, 26. Moreover, the technique permitted a large space for bone graft. However, the depth of intraoperative exposure was rather deep, which resulted in the resection of C2 nerve root and the unilateral placement of screws frequently. Besides, the patients with atlantoaxial dislocation accompanied with basilar invagination tended to have a high rate of vertebral artery variation, which may have a higher risk of vertebral artery injury in the operation. Therefore, occipital condylar screws might have more difficulty and risk in revision operation, and there has tended to be an alternative of occipital plate27, 28, especially for the cases who were not suitable for the placement of occipital plates due to occipital defects caused by tumors, congenital dysplasia, or iatrogenic factors. In summary, the occipital plate-screw system was still preferred for occipitocervical revision surgery, while preoperative CT scan could not be ignored to evaluate the thickness of the occipital12. Previous studies reported that plate-screw technology had a high risk of infection3 and one postoperative infection occurred in this cohort of patients. Nevertheless, we believed that perioperative antibiotic treatment, strict intraoperative aseptic operation, and timely dressing change might avoid the occurrence of infection to a certain extent.
There were several limitations in the present study. Chief among them was a lack of patients who had undergone revision surgery and relatively short-term follow-up. This was mainly due to the paucity of patients necessitating revision surgery of the craniocervical region. Another limitation was the study's retrospective nature. Further large control studies are warranted and may have more standardized outcome measures.
ConclusionPosterior occipital plate and bicortical screws provided rigid segmental fixation, relief from symptoms, and improvement in neurologic deficits with relatively simple procedure without excessive tissue release or intraspinal manipulation. Thus, it was shown to be a valuable modified technique for occipitocervical revision surgery.
AcknowledgmentsThe authors acknowledge the staff in this study (China–Japan Friendship Hospital, Beijing, China) for their collaboration involved in this work.
留言 (0)