
記住我

Hyperimmunoglobulin E (IgE) syndrome (HIES) is rare disease characterized by recurrent infections, eczema and increased serum level of IgE.1 Mutation of signal transducer and activator of transcription 3 (STAT3) is one major cause of HIES. Although the prognosis of HIES is unclear, pulmonary infections and lymphoma are considered the leading causes of death. Chronic pulmonary aspergillosis (CPA) is a chronic progressive infectious disease common in patients with underlying pulmonary diseases, but there are few reports of complications due to HIES. We report a case of HIES comorbid with CPA in a teenage male.
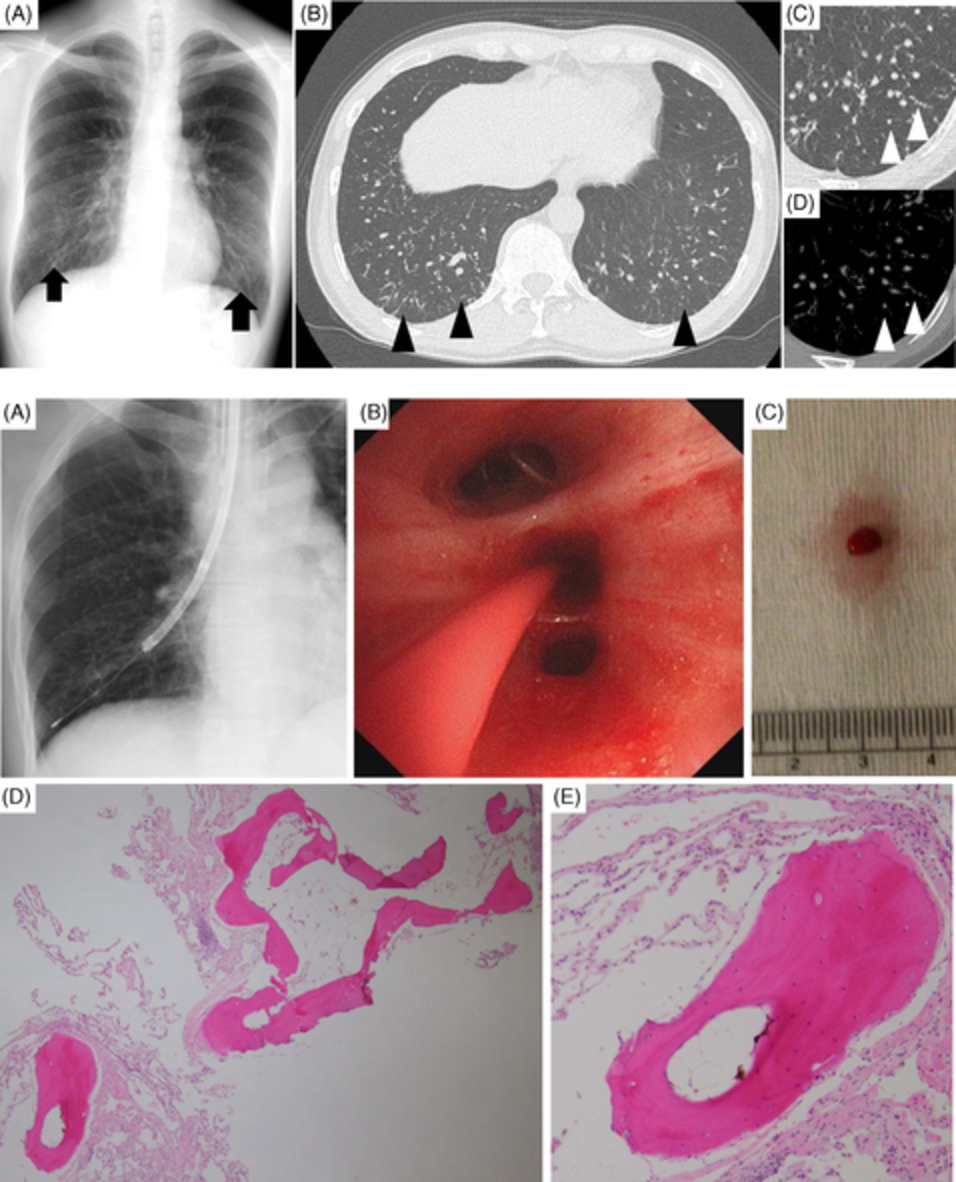
CASE REPORTA 19-year-old male was referred to our department for comprehensive assessment and holistic management of pulmonary disease. He had medical histories of recurrent bacterial pneumonia, Staphylococcus aureus skin infection, bacterial spinal abscess, oesophageal candidiasis, multiple minor trauma fractures, hyperextensibility of joints and scoliosis and failure to exfoliate primary teeth. Laboratory findings showed an elevated eosinophil count (2160/μl) and serum IgE level (4790 IU/dl). Chest x-ray and computed tomography (CT) showed a pneumatocele and bronchiectasis (Figure 1). We initially considered the possibility of congenital immunodeficiency disorders as his clinical findings were consistent with HIES. A later genetic mutation analysis revealed a mutation affecting the transactivation domain of the STAT3 gene, and he was diagnosed as having HIES. He was already being treated with oral trimethoprim/sulfamethoxazole, and erythromycin was added to prevent recurrent lung infection.

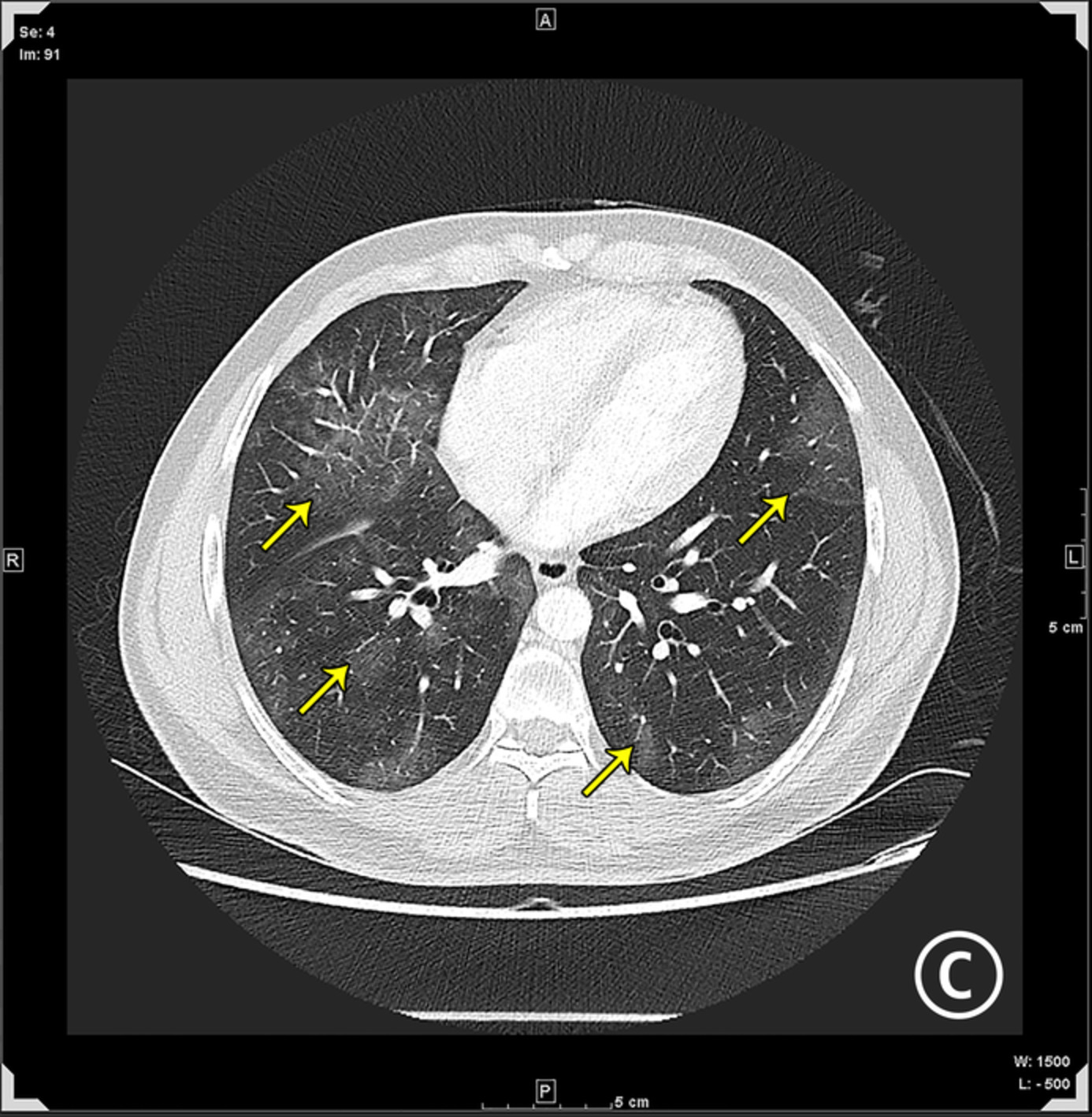
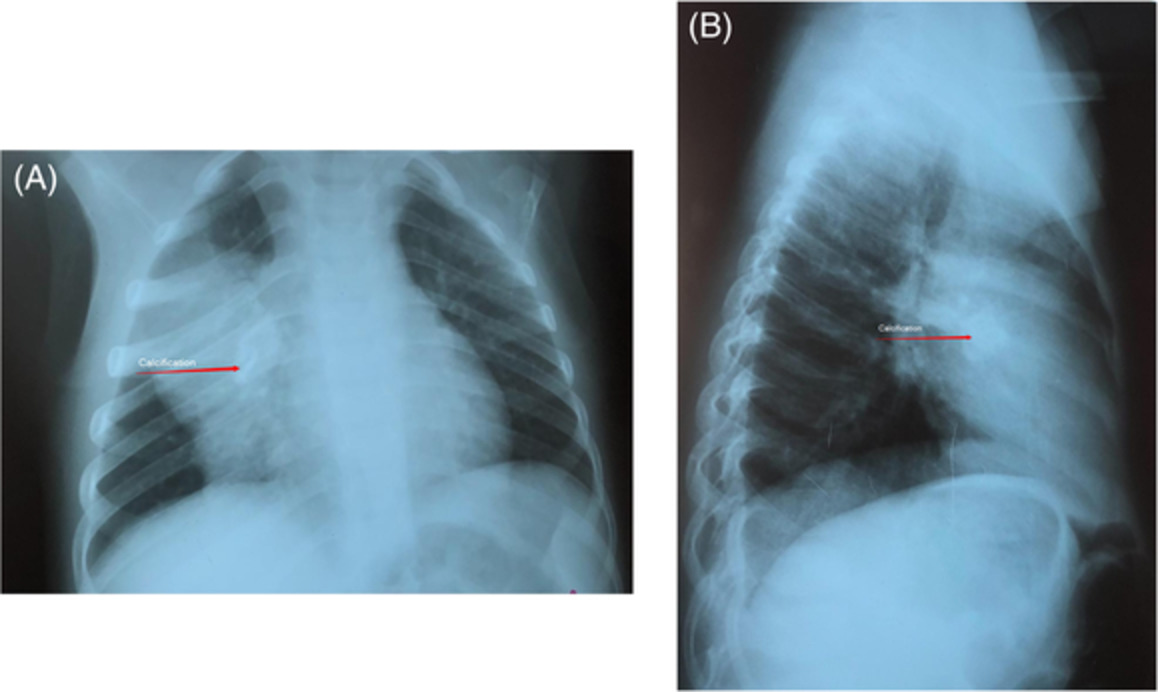
On admission, a chest x-ray showed a pneumatocele in the right lung and bronchiectasis (A), and chest computed tomography showed a pneumatocele in the right upper lobe and bronchiectasis in the left lower lobe (B, C)
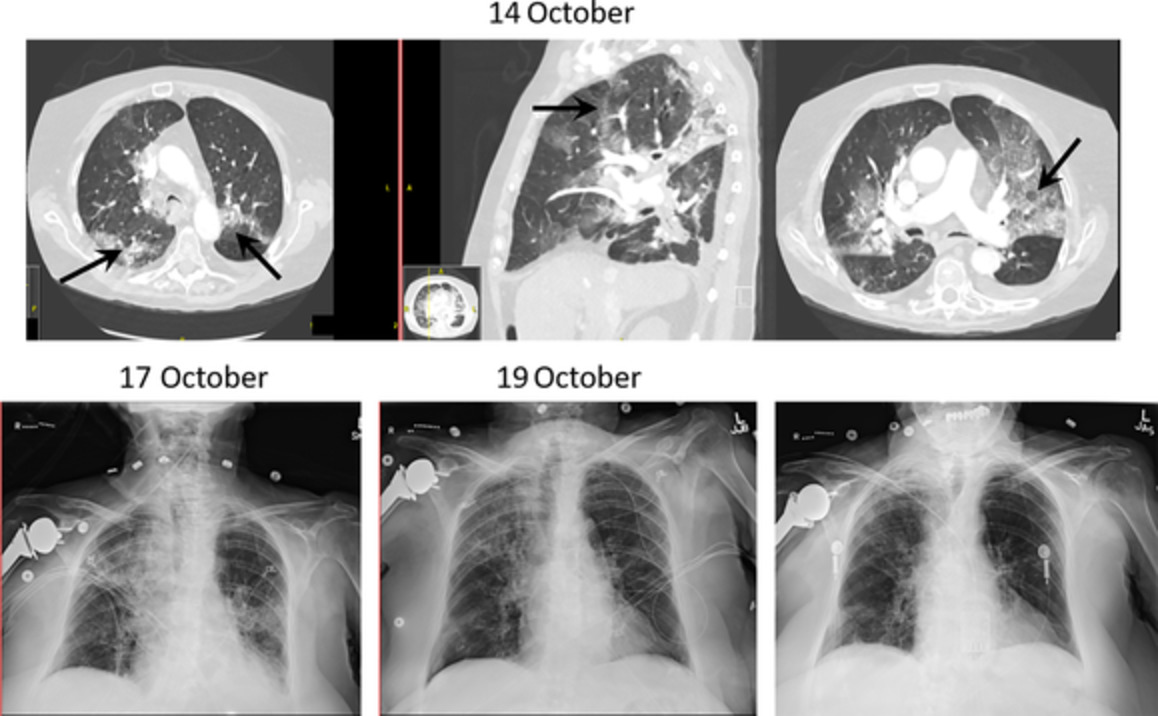
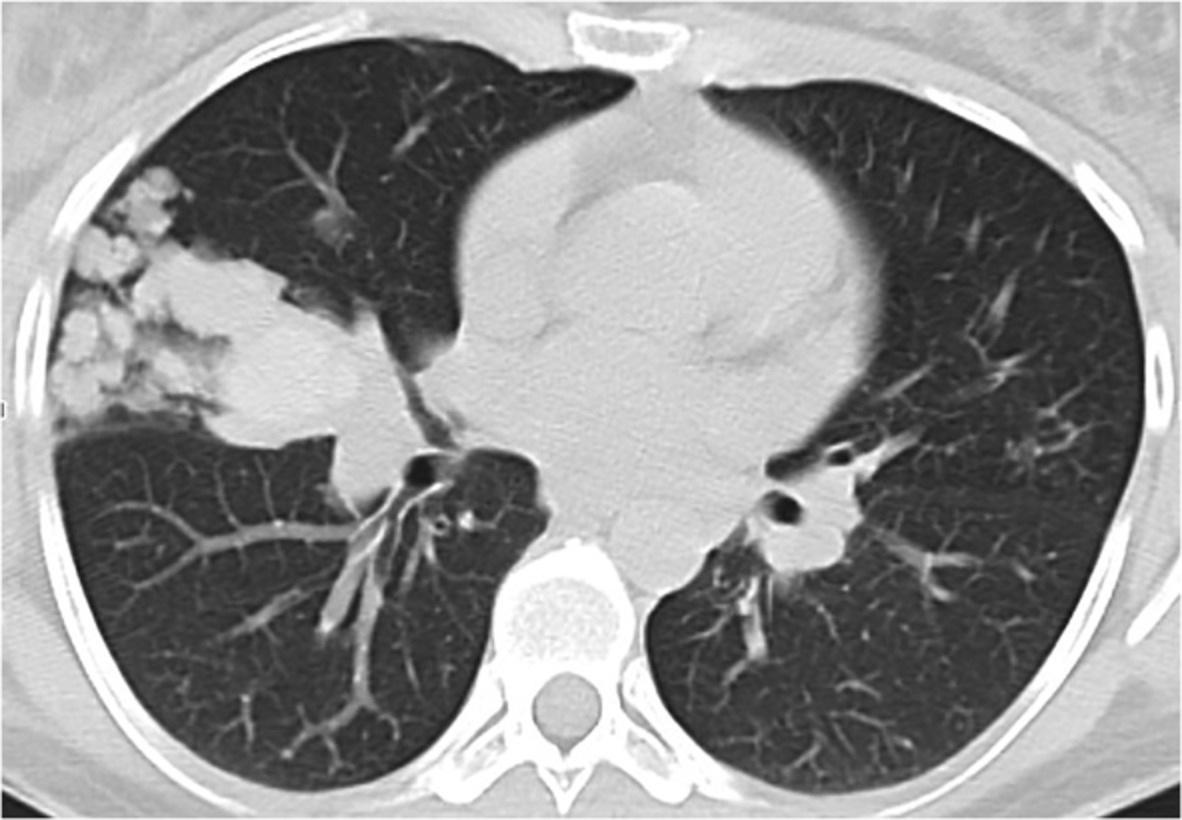
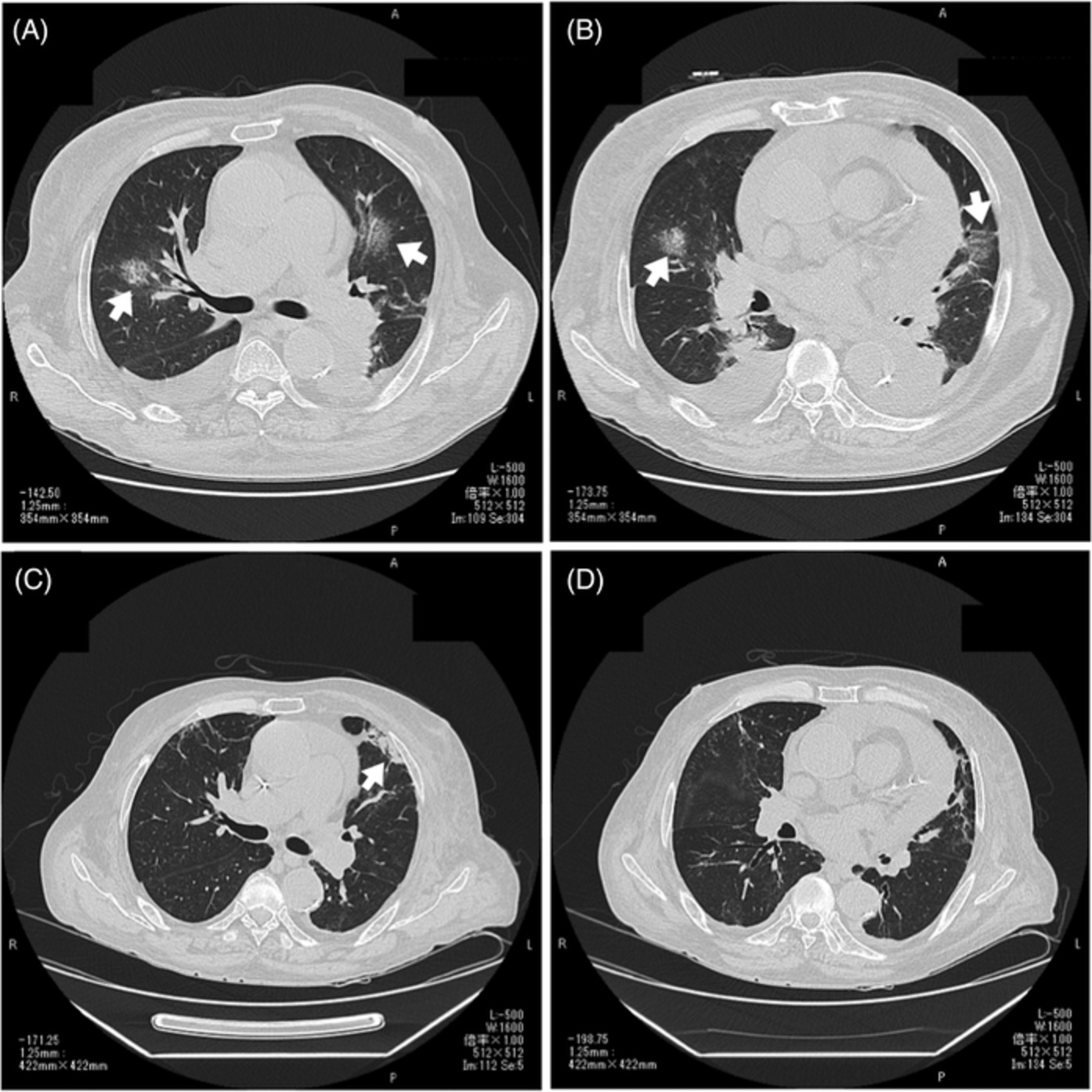
Fourteen months after consultation, he complained of blood-tinged sputum and haemoptysis that had continued for several weeks. Chest x-ray showed a consolidation in the right lung (Figure 2A), and chest CT showed wall thickening of the pneumatocele, a fungus ball and consolidation around the pneumatocele and bronchiectasis (Figure 2B,C). He was positive for serum Aspergillus precipitating antibody and serum galactomannan Aspergillus antigen, and Aspergillus fumigatus was detected in his sputum.

At 14 months after consultation, a chest x-ray showed consolidation around the pneumatocele in the right lung and bronchiectasis in the bilateral lungs (A). Chest computed tomography showed thickening of the pneumatocele wall, a fungus ball, consolidation around the pneumatocele in the right upper lobe and consolidation around the bronchiectasis in the left lower lobe (B, C)
We diagnosed CPA and hospitalized him for treatment. Infusion therapy with micafungin was initiated and later switched to orally administered voriconazole (VRCZ). During hospitalization, his haemoptysis worsened and he subsequently underwent interventional angiography and right bronchial artery embolization that improved his symptoms, and he was discharged.
DISCUSSIONWe experienced a patient with HIES and CPA that improved with appropriate treatment. HIES, formerly called Job's syndrome, was first reported in 1966.2 A main cause of HIES is the STAT3 mutation, which results in multi-organ disease with abnormalities in the immune system, bone, teeth and soft tissues. STAT3 is reported to be involved in signalling of several cytokines, growth factors and hormones, and its mutations are thought to cause a variety of clinical manifestations of HIES such as impaired Th17 cell differentiation.3 Human keratinocytes and bronchial epithelial cells are deeply dependent on the synergistic action of Th17 cytokines and classical proinflammatory cytokines for their production of antistaphylococcal factors, including neutrophil-recruiting chemokines and antimicrobial peptides. These findings suggest that bacterial infections selectively occur in the skin and lungs of patients with HIES.
In contrast, CPA often develops in patients with existing pulmonary diseases such as previous pulmonary tuberculosis, chronic obstructive pulmonary disease, interstitial pneumonia and non-tuberculous mycobacteriosis.4 However, as HIES is a very rare disease, it was not mentioned in the review of CPA, which is diagnosed by combined evaluation of symptoms, imaging findings, bacterial detection and laboratory findings. Its prognosis is not good, and treatment is often difficult.
Staphylococcus aureus and Candida albicans are well-known causes of infectious diseases associated with HIES,1 but Aspergillus infections have also been reported. Duréault et al. reported that 13 of 74 STAT-3-deficient patients with HIES (17.5%) were identified as having pulmonary aspergillosis,5 of whom 90% had previous bronchiectasis or cavitation. The present patient also had a huge pneumatocele and bronchiectasis on chest CT before diagnosis and was diagnosed as having CPA because of the subsequent appearance of symptoms, detection of Aspergillus in sputum and positive Aspergillus antigen and precipitating antibody tests.
In general, the main treatment for CPA is antifungal agents, and surgery can also be considered. In previous reports on CPA with HIES, administration of antifungal agents and also surgery were commonly performed.5 Specifically, among the patients with aspergilloma, three patients received VRCZ and two underwent surgery. Among those with chronic cavitary pulmonary aspergillosis, seven patients received VRCZ or liposomal amphotericin B, and five surgeries were performed in four patients.
It is common to treat HIES with trimethoprim/sulfamethoxazole to prevent cutaneous staphylococcal infection and pneumonia. However, there is no consensus on treatment with antifungal agents. In Duréault et al.'s report, only three of the 13 patients with HIES and CPA were treated prophylactically with antifungal agents.5 This low treatment number may have been due to concerns about adverse events such as hepatic disorders.
After admission, the present patient was first treated with micafungin and was then switched to VRCZ. Then, following an episode of haemoptysis, bronchial artery embolization was performed. Although there is no consensus on the duration of treatment, this patient may require long-term oral administration of VRCZ due to the presence of multiple lesions. Surgery may be considered in the future if treatment can reduce the active lesions to one.
Our patient also had mild hepatic disorder because he took trimethoprim/sulfamethoxazole, so the prophylactic administration of antifungal agents was not performed. However, if the patient had had a lung structure that could develop into CPA, the advantages of administering this agent might outweigh its disadvantages. Further accumulation and analysis of cases are needed in the future.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
留言 (0)