
記住我
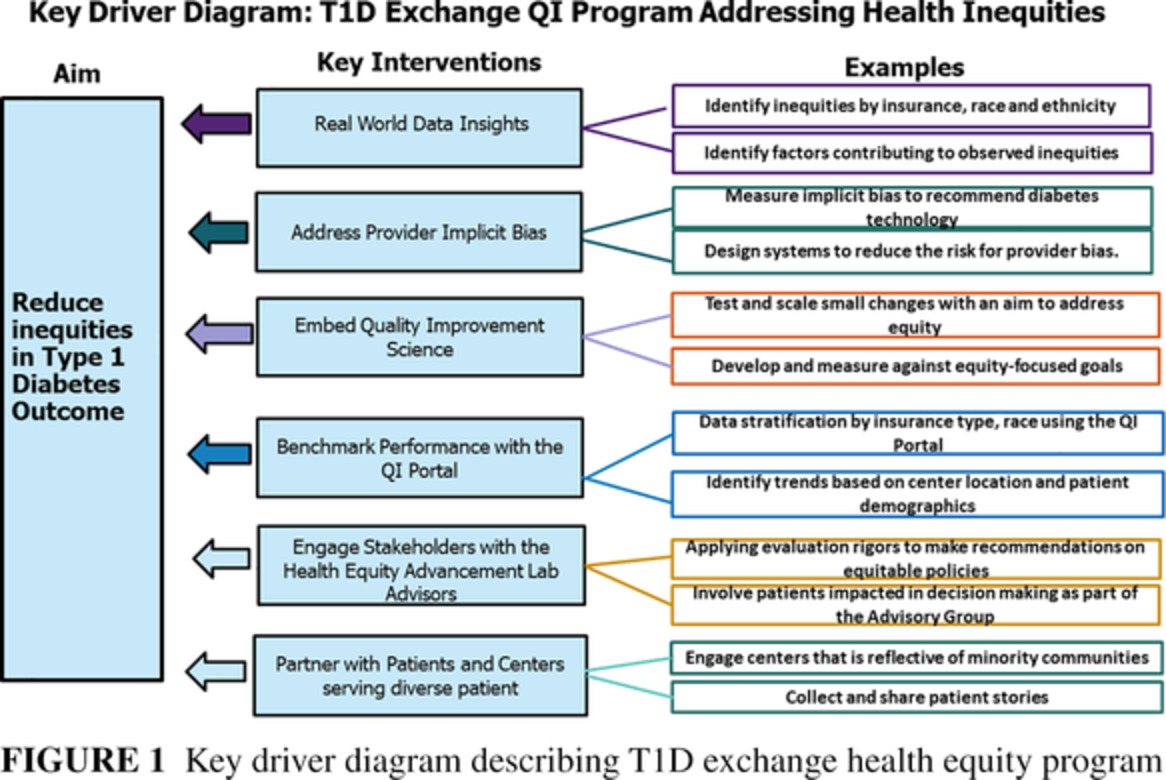

Since the discovery of insulin 100 years ago, there have been continual advances in medications and technologies for the management of type 1 diabetes (T1D). Despite these innovations, many people struggle to meet hemoglobin A1c (HbA1c) goals, and the gap is larger in individuals from minority groups1 or lower socioeconomic status. Quality improvement (QI) efforts have been shown to improve outcomes for patients with T1D.2 The T1D Exchange Quality Improvement Collaborative (T1DX-QI) was established in 2016 with 10 pilot centers, primarily consisting of pediatric sites.3, 4 The collaborative has now grown to 41 participating centers (28 pediatric and 13 adult centers) across the United States (Figure 1).

Map showing the geographic distribution of the 41 T1DX-QI centers. QI, quality improvement; T1D, type 1 diabetes; T1DX-QI, T1D Exchange Quality Improvement Collaborative
In this commentary, we describe the goals of the T1DX-QI and highlight QI and population health conference abstracts recently presented at the 2021 T1DX-QI conference.
The T1DX-QI has five core goals:
1. Collecting the right kind of data to drive real-world improvements.
2. Using data to make the best decisions for the population of people with T1D.5
3. Designing and testing initiatives to improve clinical and T1D population health outcomes.6, 7
4. Quantifying factors that are contributing to driving positive outcomes for the T1D population.8, 9
5. Generating real-world insights.5, 9
These goals are summarized by a population health improvement framework to improve diabetes clinical processes (Figure 2).

T1DX-QI population health improvement model. QI, quality improvement; T1D, type 1 diabetes
At the T1DX-QI 2021 conference, 21 QI and population health abstracts were shared that highlight how endocrinology centers are addressing the five goals of the T1DX-QI network. Common themes from the abstracts involved infrastructural support of QI, developing population health initiatives, improving psychosocial support, and closing inequities in diabetes technology access and use.
A strong QI culture is important for implementing and sustaining change. A QI culture self-assessment completed during the orientation phase of joining T1DX-QI provided the framework for T1DX-QI to develop center-specific QI coaching and support skill growth.10
At the cornerstone of T1DX-QI is an electronic medical record (EMR) database used for collecting and benchmarking population health real-world data. Benchmarking reports help identify areas for center-specific QI efforts.11
The data shared from benchmarking reports help individual centers identify needs at their institutions and implement QI initiatives to improve diabetes care. These initiatives are supported by improvement coaches, and the outcomes are shared frequently with all the centers, contributing to more rapid success.
EMR-based flowsheets can be used by diabetes team members to help standardize diabetes care and collect database metrics. The collected data are mapped from each centerʼs EMR to the T1DX-QI database, following a unified data schema. The quality of data within the EMR database is dependent on validation of data at the site level. An open-source lightweight schema and data validation framework was added to the data extraction, mapping, and validation pipeline by one center to reduce the number of errors in the submitted data.12 By sharing successful learnings such as these, new centers can more rapidly map their data to the T1DX-QI database and more fully participate in QI initiatives.
The sharing of data in the T1DX-QI database informs QI-based population health interventions to improve outcomes. Examples include the 4T Program (Teamwork, Targets, Technology, and Tight Control), which incorporated technology and intensified education to improve outcomes during the first year after diabetes diagnosis in a pediatric population,13 and the report from Nudrat Noor et al that described obesity trends over 5 years for people with T1D.14
In addition to using these data to provide insights for designing QI interventions, T1DX-QI QI teams also use them to support policy changes, for example, Medicaid coverage of continuous glucose monitors (CGMs) in Texas as reported by McCann-Crosby et al15 and to predict HbA1c rise in a pediatric population using a machine learning algorithm.16 These learnings and successes can be used by other centers to support people with newly diagnosed or established diabetes.
T1D is associated with greater psychosocial challenges.17 The presence of depression, anxiety, and diabetes distress can affect the individualʼs ability to self-manage their diabetes. The American Diabetes Association Standards of Medical Care recommend routine screening for depression.18 One of the early projects of the T1DX-QI was to assess and improve rates of depression screening. Centers have used the Patient Health Questionnaire screening tools with EMR-based tracking and have successfully increased the percent of their T1D population who receive annual depression screening.19 Because diabetes-specific psychosocial distress is associated with increased rates of diabetic ketoacidosis (DKA), Dei-Tutu et al20 implemented annual depression screening along with an EMR-based risk score for DKA admission for their pediatric population. Those who met criteria were enrolled in an extra-care program to prevent DKA admissions. This QI intervention reduced DKA admissions from baseline 9.5% to 6.02% in 2020.
One of the biggest challenges facing youth with T1D is the transition from pediatric care to adult care.21 This transition is associated with an increased incidence of acute complications.22 Given the importance of transition education and preparation, several centers have implemented QI efforts to improve transition discussions and readiness. Standardizing and documenting the processes, including incorporating transition assessments, individualized education sessions, and action plans, led to significant improvements in the number of transition discussions and identification of knowledge gaps with adolescents in the centers to improve diabetes self-management.23
Advances in diabetes technology, such as the availability and use of CGMs, have greatly improved the lives of people with T1D. Unfortunately, there are inequities in the use of and access to these devices.24, 25 In the T1DX-QI EMR database, individuals who identified as Hispanic or Non-Hispanic Black had lower rates of pump usage compared to individuals who identified as Non-Hispanic White.26 Several centers have benchmarked rates of CGM and insulin pump use in their own center and found similar trends. These data show the need for identifying factors associated with technology use by individuals of minority status and developing targeted interventions to close these gaps. One of the barriers to technology access is the absence of insurance coverage for those on public insurance. McCann-Crosby et al15 used QI methodology to track CGM usage and presented the data to state Medicaid to obtain CGM coverage for those with public insurance. Other sites conducted semistructured interviews with parents of Non-Hispanic Black youth with T1D to understand barriers to technology use. A pediatric center developed interventions to increase provider education, patient support, and advocacy to increase CGM uptake in those with Medicaid and those with HbA1c > 9%. An adult center increased CGM use by developing provider training in CGMs and inequity in access while streamlining prescribing workflows. The gaps identified by these centers and the interventions to improve equity can be used by other clinics to bolster QI efforts.
2 CONCLUSIONBenchmarking of T1D quality metrics identifies gaps in diabetes care that are important targets for QI interventions. T1DX-QI data examined by race and ethnicity exposed inequities in care. This has led to site-specific data analyses and implementation of QI interventions focused on decreasing inequities in care by implementing interventions including increasing use of CGMs, improving psychosocial support, and assessing their effectiveness with frequent data collection and analyses. Sharing of these data in the context of a learning health system can accelerate improvements in diabetes care and health equity.
ACKNOWLEDGEMENTWe appreciate all members of the T1DX-QI Collaborative, patients, and partners. We are grateful to the Helmsley Charitable Trust that funds the T1DX-QI Collaborative.
DISCLOSURESRR is associate editor for the Journal of Diabetes. RSW participates in multicenter clinical trials, through her institution, sponsored by Medtronic, Insulet, Eli Lilly, Novo Nordisk, Boehringer Ingelheim, and Kowa. Dexcom has contributed CGMs for other studies. OE is a member of the Medtronic Diabetes Health Equity Advisory Board; He is the principal investigator for research projects funded by Eli Lilly, Medtronic Diabetes, Abbot, and Dexcom. All the funds for these industry-funded projects and board roles are paid directly through his organization, T1D Exchange. All other authors report no conflicts.
留言 (0)