
記住我

Airway foreign bodies in older adults are often detected as a result of pneumonia or respiratory failure and need to be rapidly removed. Flexible bronchoscopy is the first choice for airway foreign body removal, with a success rate of approximately 80%–90%.1, 2 However, in some cases, removal of foreign bodies may not be achieved using flexible bronchoscopy and rigid bronchoscopy or surgery is required.1, 2 Therefore, it is clinically important to improve the technique for airway foreign body removal using a flexible bronchoscope.
Forceps, magnetic probes, snares, baskets, balloon catheters and cryoprobes are used to remove foreign bodies from the lower airway.3 The use of cryoprobes is a relatively new technique in airway foreign body removal. The utility of cryoprobes for the removal of aspirated teeth is controversial.4, 5 In this report, we demonstrate the efficacy of a cryoprobe in removing airway foreign bodies caused by dental aspiration in an older patient.
CASE REPORTAn 88-year-old man who had been in a nursing home for a long time due to consciousness disturbance caused by Alzheimer's disease had repeated episodes of fever, and when he was examined at a nearby general hospital, he was observed to have pneumonia and a bronchial foreign body. An attempt was made to remove the foreign body using a flexible bronchoscope; however, the procedure was unsuccessful, and the patient was transferred to our hospital.
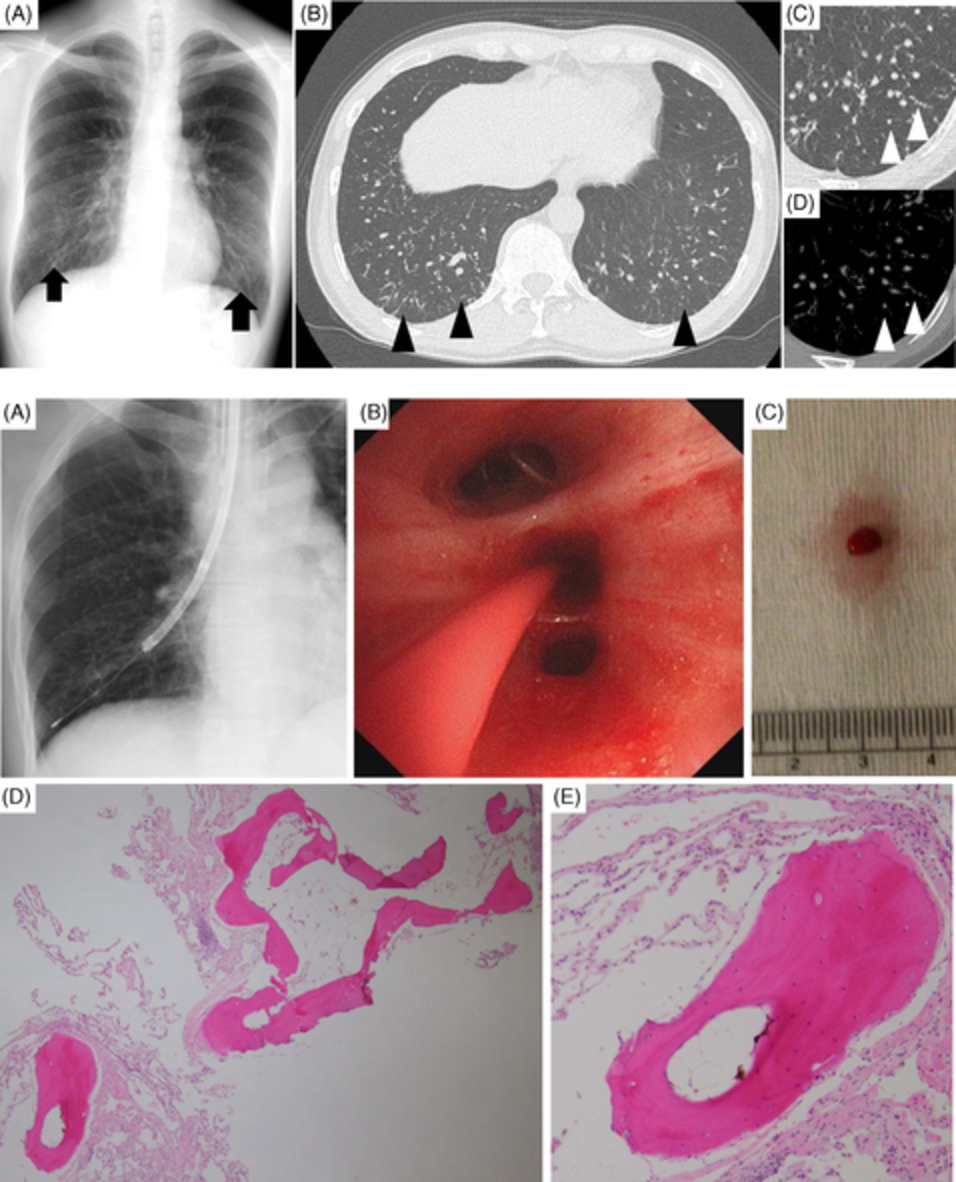
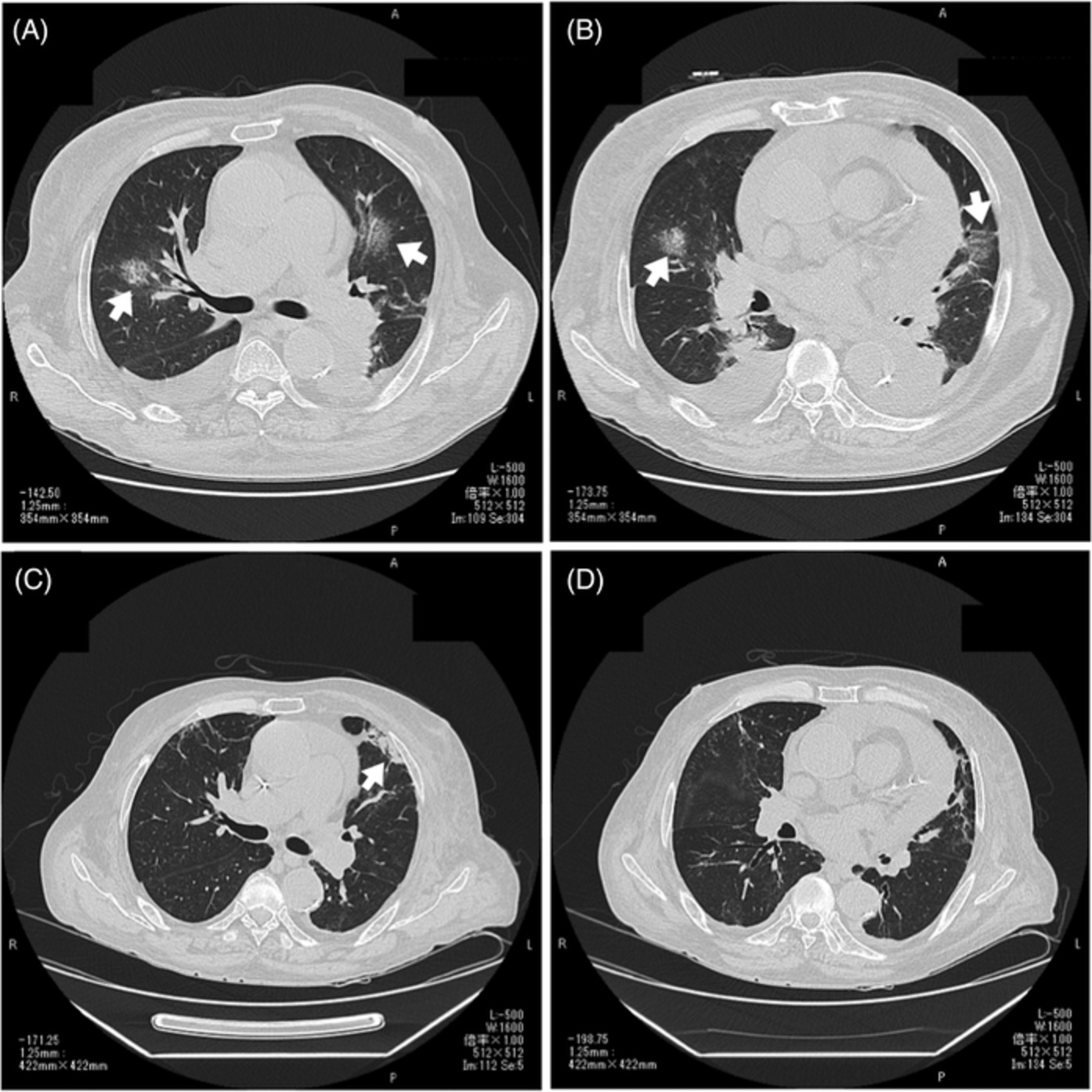
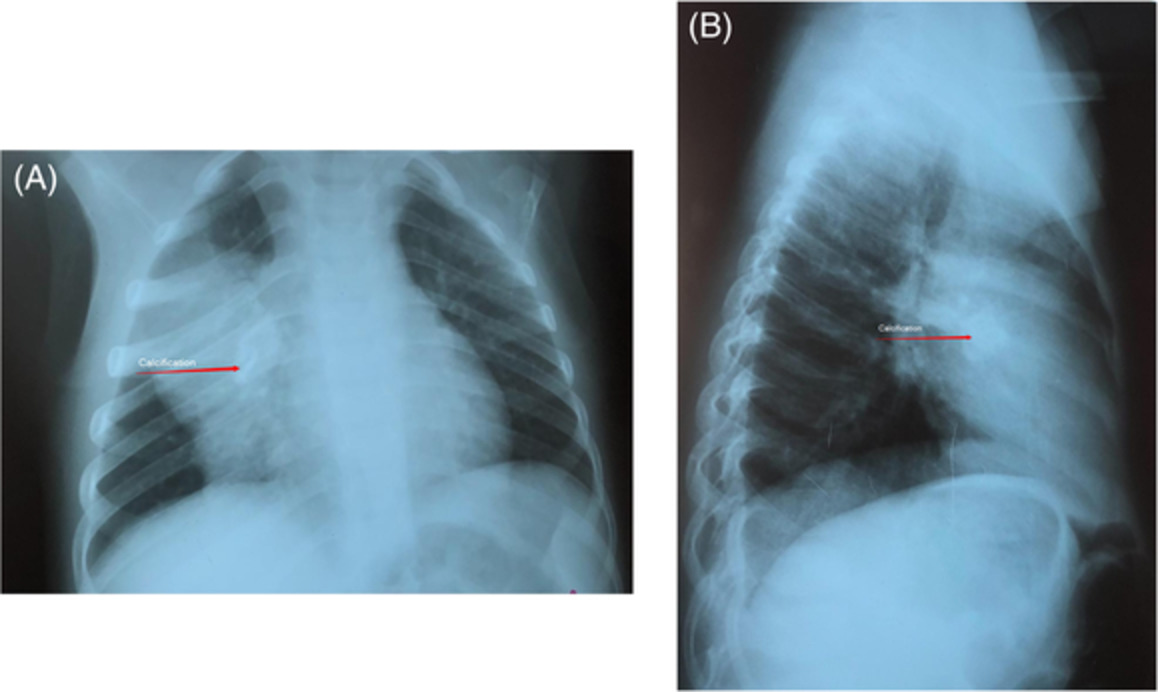
Chest radiography showed a foreign body with a maximum diameter of approximately 15 mm and a peripheral infiltrative shadow in the left lower lung field (Figure 1A). Chest computed tomography showed that the airway foreign body was located in the left lower lobe bronchus and produced halation with consolidation and pleural effusion in the peripheral part of the airway foreign body (Figure 1B,C). The patient had been intubated with an 8.0-mm inner diameter endotracheal tube at the previous hospital, and a flexible bronchoscope (outer diameter 5.9 mm, working channel 3.0 mm) was inserted through the tube to remove the airway foreign body, which was a tooth covered with a crown (Figure 2A). The 1.9-mm reusable cryoprobe was freeze-bonded to the blackened root of the tooth, and an attempt was made to pull it out; however, contact between the tip of the endotracheal tube and the tooth caused it to be dislodged from the cryoprobe and roll back into the left bronchus. The tooth was successfully removed by freeze-adhering it again with the cryoprobe, pulling it up to the front of the endotracheal tube, and then removing it in one piece with the tube, bronchoscope and cryoprobe to avoid contact with the tracheal wall or the tip of the endotracheal tube (Figure 2B). The airway foreign body was a 13 × 12 × 12 mm silver-crowned molar with a carious root (Figure 2C). After removal of the foreign body, the patient's respiratory status was stable with only oxygen inhalation, and re-intubation was not necessary. The bronchial mucosa was rough and erosive; however, there was no persistent bleeding. The patient was discharged to a nursing home after treatment of pneumonia with antibacterial agents.

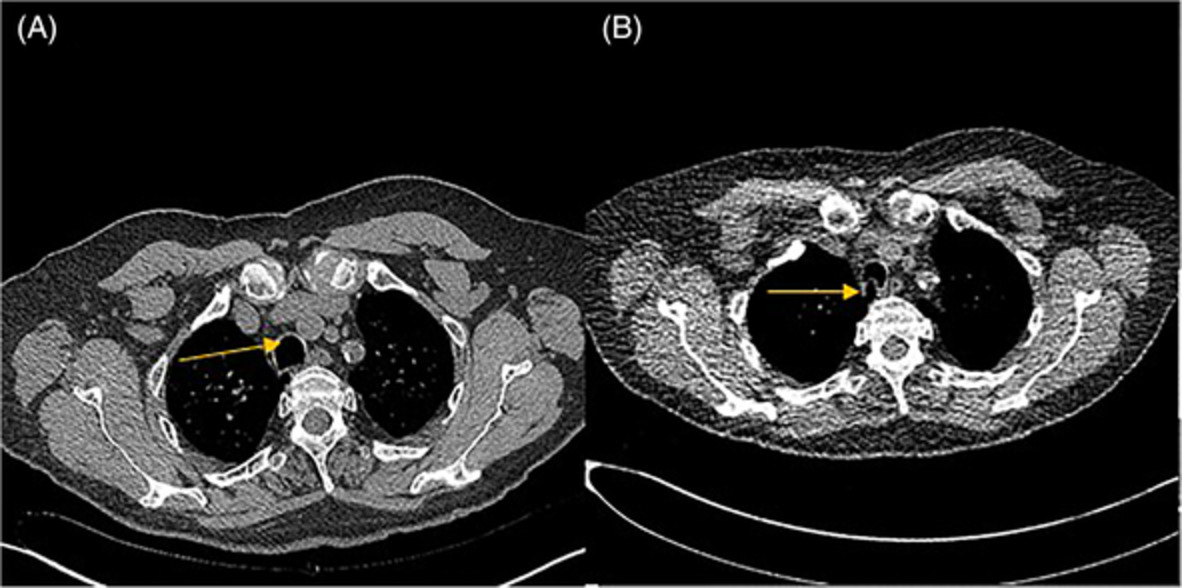
Chest radiography and computed tomography (CT) findings. A chest radiograph (A) shows a foreign body of approximately 15 mm diameter in the left pulmonary hilum. There is an infiltrative shadow in the left lower lung field and positive silhouette signs of the descending aorta and left diaphragm. On chest CT (B, C), there is an airway foreign body with halation in the left lower lobe bronchus, with consolidation in its obliteration, and pleural effusion

Bronchoscopic findings. A molar with black discolouration of the root embedded in the left lower lobe branch entrance (A). The airway foreign body was freeze-bonded with a cryoprobe and pulled up (B). Removed airway foreign body was a 13 × 12 × 12 mm silver-crowned molar with a carious root. Scales are in 1 mm increments (C)
DISCUSSIONForeign bodies of aspirated tooth account for about 15%–20% of airway foreign bodies in adults.1, 2 But the removal of aspirated teeth, especially molars lodged in the bronchi, is technically difficult. Grasping forceps cannot grasp airway foreign bodies that do not have a projection, are too wide or are round in shape, such as an aspirated molar. Furthermore, airway foreign bodies that have become lodged in the bronchi are often difficult to retrieve into the basket forceps because the wires of the basket forceps extend only to the diameter of the bronchi. Airway foreign bodies lodged in the bronchi are often removed using both a Fogarty catheter and grasping or basket forceps. The Fogarty catheter is used to withdraw the foreign body from the airway in front of the bronchus, and grasping or basket forceps are used to remove the foreign body.3 Cryoprobes have also been reported as useful for airway foreign body removal.3 The ability to remove a foreign body using a cryoprobe depends on its cryoadhesive properties, which depend on the water content of the foreign body material.5 In vitro experimental studies on various foreign bodies have shown that teeth and crowns cannot be cryo-grasped.5 However, in this clinical experience, the cryoprobe was effective for removal of an aspirated tooth. Owing to the patient's impaired consciousness, we were unable to establish the exact time of the aspiration of the tooth. The tooth was probably covered with mucus for a long time, which allowed it to be frozen and grasped with a cryoprobe, as reported by Schumann et al.4 Therefore, if the time since the foreign body aspiration has been prolonged, the application of a cryoprobe is worth considering even if the airway foreign body is an aspirated tooth.
On the other hand, the freezing power of the cryoprobe against airway foreign bodies with low water content is not strong, and the foreign body and probe are easily dislodged during the removal process. In the present case, as the airway foreign body was pulled up, the freezing grip came off in contact with the tip of the endotracheal tube, and the airway foreign body fell into the bronchus again. It is important to manipulate the bronchoscope and cryoprobe such that they do not contact the walls of the bronchi or the entrance of the endotracheal tube.
Methods for removal of airway foreign bodies are limited. The expanded use of cryoprobes may contribute to the success rate of airway foreign body removal.
ACKNOWLEDGMENTThe authors thank Editage (www.editage.jp) for English language editing.
CONFLICT OF INTERESTNone declared.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
Data sharing is not applicable to this article as no data sets were generated or analysed during the current study.
REFERENCES
1Sehgal IS, Dhooria S, Ram B, Singh N, Aggarwal AN, Gupta D, et al. Foreign body inhalation in the adult population: experience of 25,998 bronchoscopies and systematic review of the literature. Respir Care. 2015; 60: 1438– 48. 2Ng J, Kim S, Chang B, Lee K, Um SW, Kim H, et al. Clinical features and treatment outcomes of airway foreign body aspiration in adults. J Thorac Dis. 2019; 11: 1056– 64. 3Hewlett JC, Rickman OB, Lentz RJ, Prakash UB, Maldonado F. Foreign body aspiration in adult airways: therapeutic approach. J Thorac Dis. 2017; 9: 3398– 409. 4Schumann C, Kropf C, Rüdiger S, Wibmer T, Stoiber KM, Lepper PM. Removal of an aspirated foreign body with a flexible cryoprobe. Respir Care. 2010; 55: 1097– 9. 5Fruchter O, Kramer MR. Retrieval of various aspirated foreign bodies by flexible cryoprobe: in vitro feasibility study. Clin Respir J. 2015; 9: 176– 9.
留言 (0)