
記住我

Oesophageal intramural pseudodiverticulosis (EIP) is a rare benign disease characterized by multiple small outpouching lesions on the oesophageal wall. This condition was described by Mendl et al. in 1960 and the cases present with dysphagia and food impaction that usually resolve spontaneously.1 It is a very rare entity that there are only about 200 reports published all around the world.2
Here, we report a patient who suffered from a non-resolving pneumonia and was ultimately diagnosed as EIP leading to a chest infection.
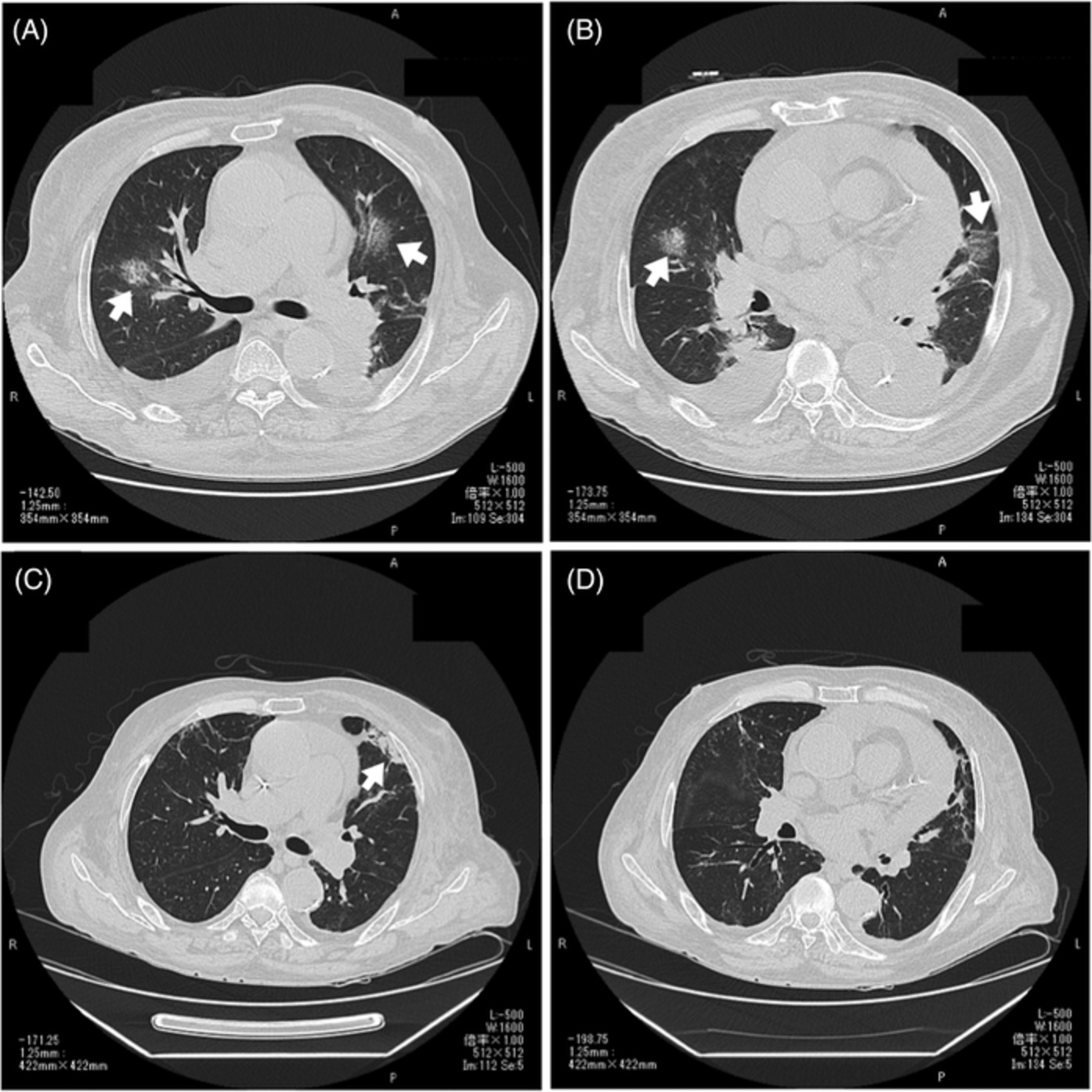
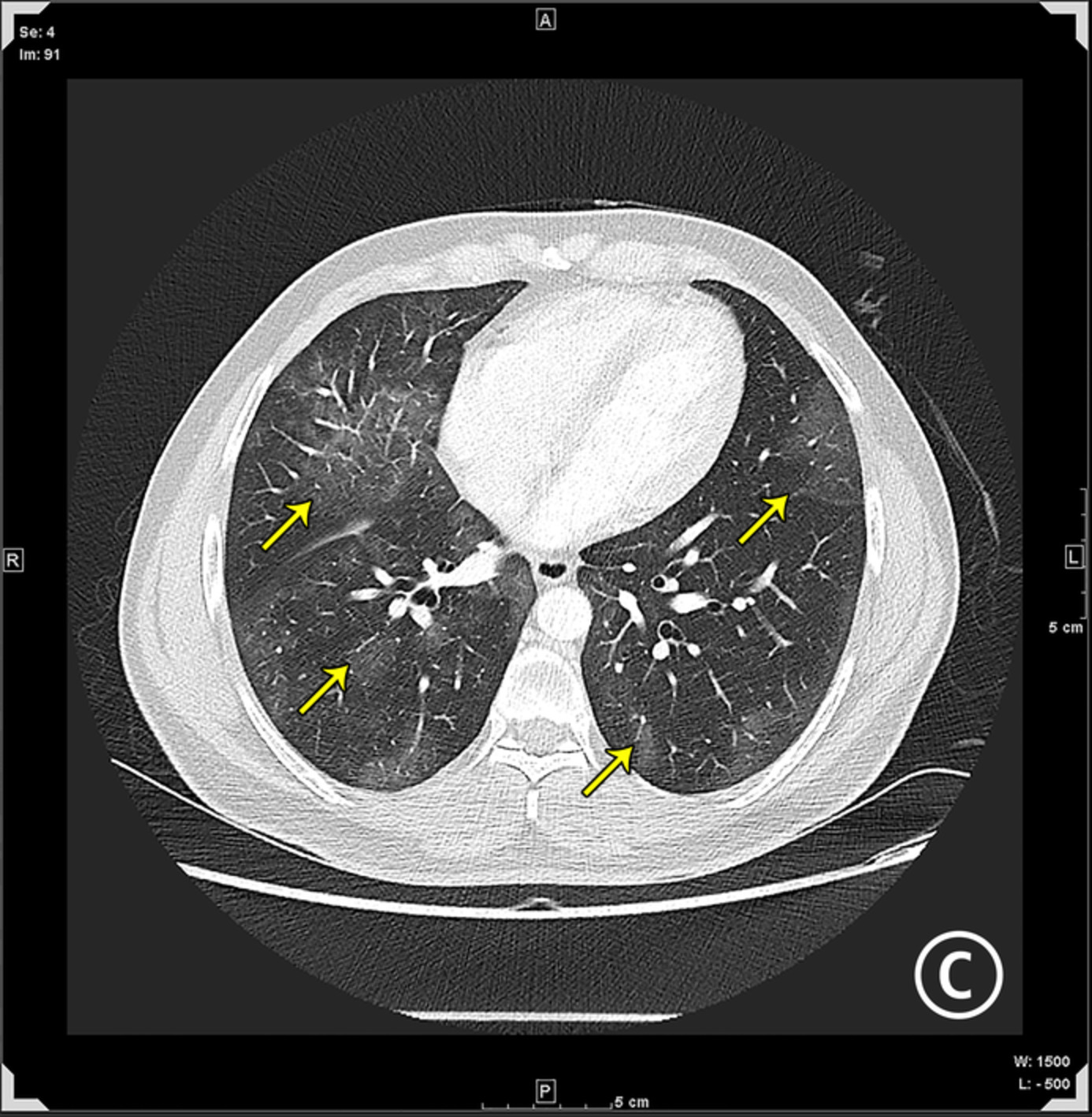
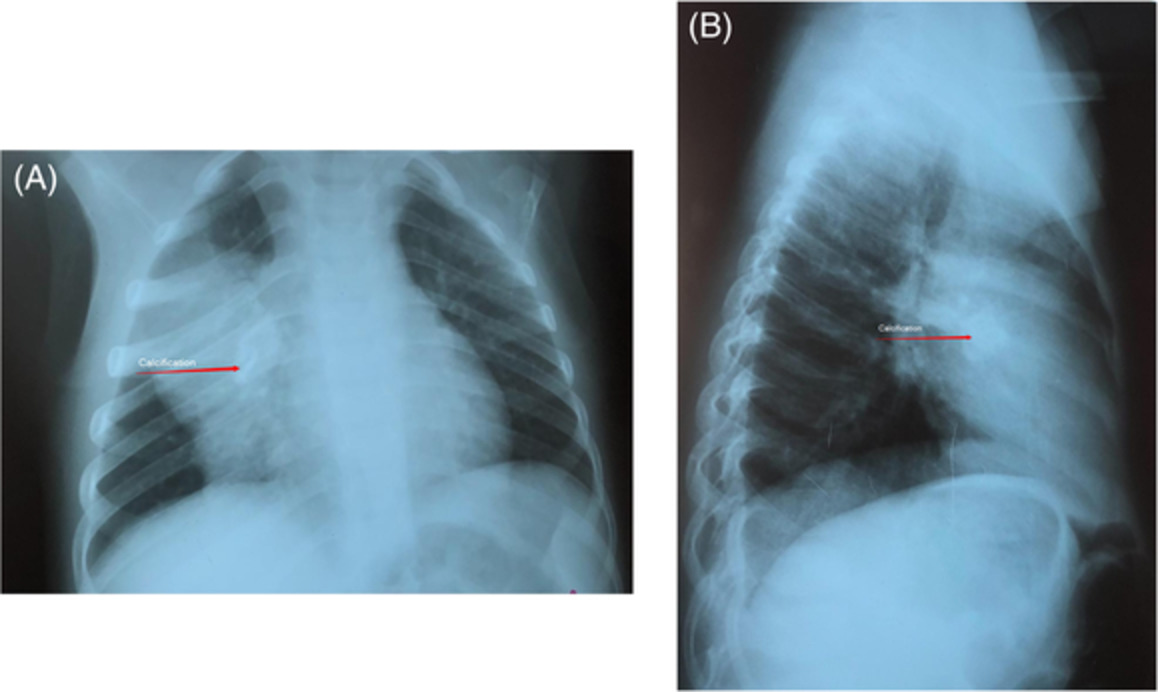
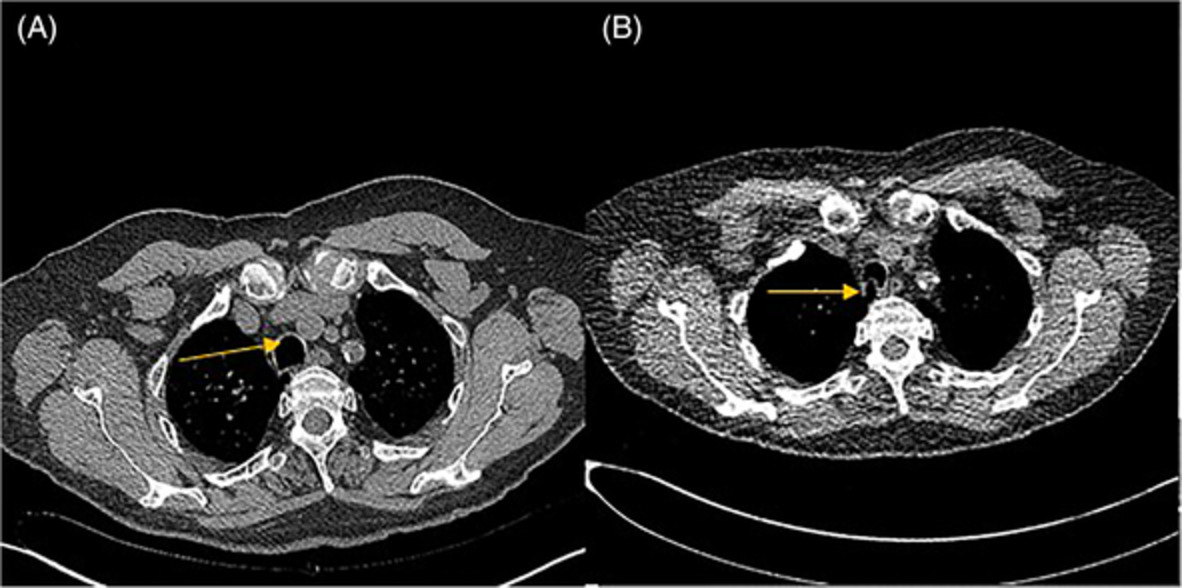
CASE REPORTA 60-year-old diabetic gentleman was referred to our centre for a non-resolving pneumonia. He had previously received two courses of broad-spectrum antibiotics (amoxicillin-clavulanate + azithromycin and piperacillin + tazobactam) in the past 3 weeks. His high-resolution computed tomography (CT) of the thorax showed bilateral lower lobe consolidation with associated pleural collection (Figure 1A). The patient was admitted to our centre and a contrast CT of the chest showed bilateral pleural effusion with minimal parenchymal infiltrates in both lower lobes with an associated paraoesophageal collection with thick-walled oesophagus. On further questioning, the patient revealed dysphagia to solids for 2 months. Positron emission tomography-CT showed diffuse fluorodeoxyglucose uptake in oesophageal wall and at GE junction (Figure 1B). A differential of oesophageal carcinoma with tracheoesophageal fistula was made. The patient then underwent upper gastrointestinal endoscopy which showed few mucosal sinuses of various sizes ranging from 3 to 7 mm with plaques but no other mucosal lesion indicative of malignancy or tracheo-oesophageal fistulas (Figure 2A). Gastrografin study was conducted which demonstrated multiple false luminal diverticula and irregular oesophageal lumen that helped clinch the diagnosis (Figure 3).

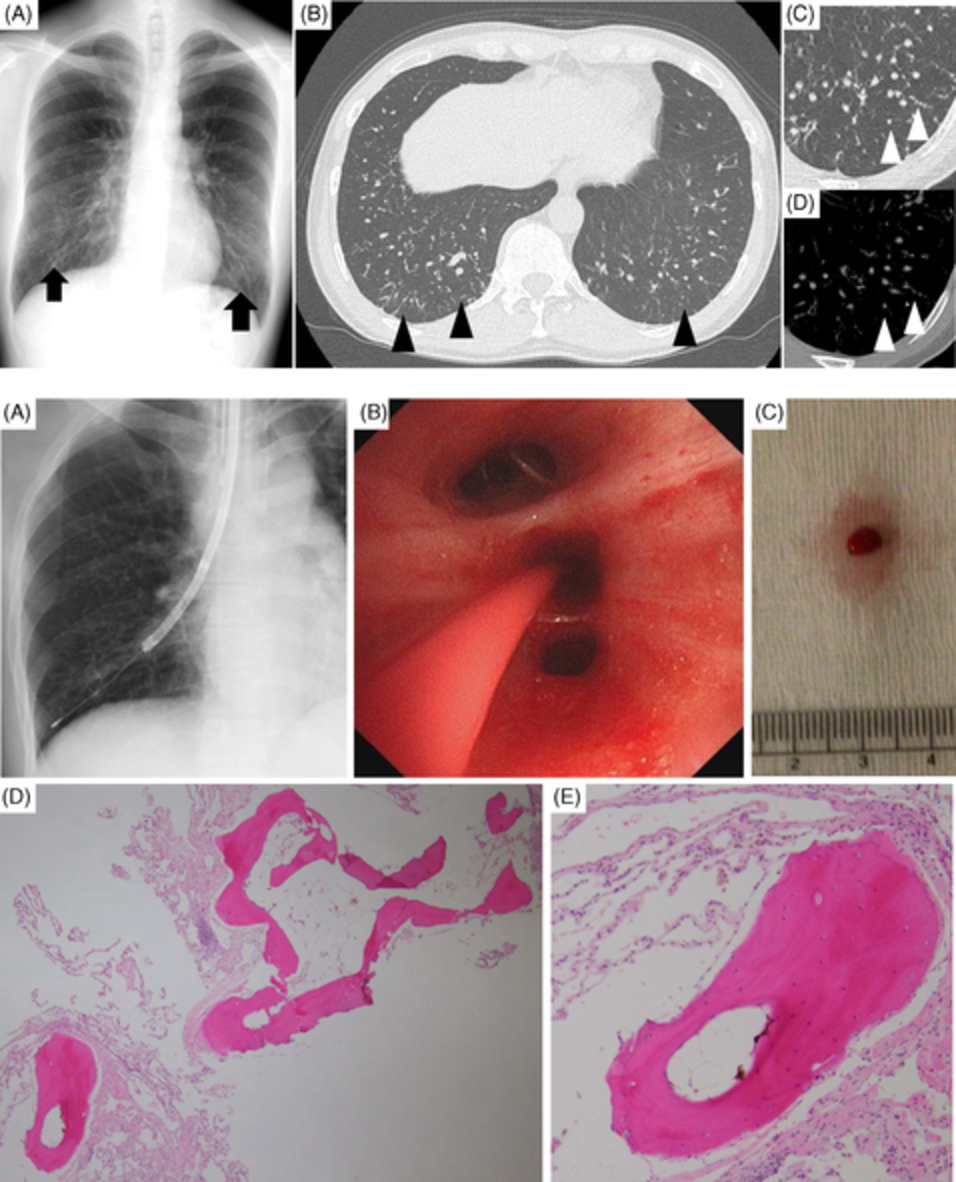
(A) Computed tomography (CT) of the thorax: bilateral lower lobe consolidation with associated pleural collection. (B) Positron emission tomography-CT: diffuse fluorodeoxyglucose uptake in oesophageal wall and at gastroesophageal (GE) junction

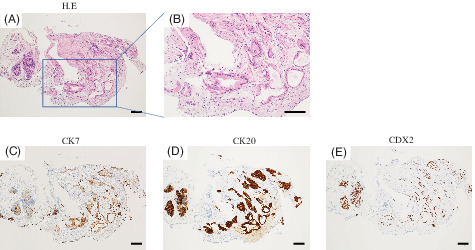
(A) Upper gastrointestinal endoscopy: few mucosal sinuses with plaques. Endoscopic ultrasound bronchoscope-guided fine needle aspiration (EUS-B-FNA): homogenous diffuse collection in para-oesophageal space

Gastrografin study: multiple false luminal diverticula and irregular oesophageal lumen
A bronchoscopy with endobronchial ultrasound (EBUS) was performed. EBUS study was non-contributing; therefore, EUS-B-fine-needle aspiration (FNA) was done that showed a homogenous diffuse collection in para-oesophageal space (Figure 2B). Fine-needle aspirate yielded small quantity of dirty white material that was sent for cytological and microbiological analyses. The EUS-B-FNA culture subsequently grew drug-resistant Candida glabrata. The patient was started on voriconazole therapy as per sensitivity pattern. His fever and appetite improved in few days. Endoscopic dilatation and stenting were done. The stent was removed after 4 weeks. The patient was allowed oral feeds which he tolerated well. Subsequent endoscopy showed a clear oesophageal lumen and the patient had no dysphagia along with complete radiological resolution.
DISCUSSIONThis patient presented as a case of non-resolving pneumonia with fever and was found to have para-oesophageal mass. These characteristics should prompt differentials of neoplasm including lymphoma or metastatic disease, tracheal or oesophageal tumours, bacterial abscesses, foregut duplication cysts and lymphadenopathy from infections such as tuberculosis or histoplasmosis.3
Our patient was initially treated with antibiotics upon suspicion of pneumonia, without clinical effect, and a bacterial infection was never documented.
The aim in this condition should be to obtain tissue biopsy to rule out neoplasm and to send it for fungal and mycobacterial smears and cultures and also concomitantly obtain appropriate serological and urinary microbiological assays to rule out the possible fungal or mycobacterial aetiology.
The mechanism in this case was oesophageal fistulas, which led to mediastinitis and recurrent aspiration causing a non-resolving pneumonia. An out-of-the-box approach using EUS-FNA helped to tissue diagnosis and definitive management.
The exact mechanism and pathogenesis for EIP are not yet understood. It is postulated that inflammation/oesophagitis and motility disorders lead to diverticular formation. Oesophageal stricture as a cause is still not clear and it may be the effect of EIP. Similarly, association of fungal esophagitis with EIP is inconsistent in all reported cases. Fungal oesophagitis is possibly one of the causes of EIP and antifungals along with serial dilatations of oesophagus have been successfully used to treat similar cases in the literature.4
EIP commonly presents with symptoms of dysphagia and/or regurgitation while some patients may also present with chest heaviness or odynophagia. It has also been seen to exist with other conditions such as diabetes mellitus, HIV disease, Chron's disease, alcohol abuse, corrosive injury, fungal esophagitis and carcinoma of oesophagus.2 Oesophageal imaging is the prime modality to establish a diagnosis. A single thin barium contrast is better in evaluation than the double contrast study. An oesophagoscopy or endoscopic evaluation also helps establishing the diagnosis.2
Ultrasound imaging of mediastinum has become part of the armamentarium for pulmonologists. EBUS-guided transbronchial needle aspirate plays an important role in the evaluation of lesions adjacent to major airways. Dual use of EBUS, through the respiratory tract and oesophagus, is feasible and can be performed in the same sitting. This was proved in 2010 through two landmark papers.5 The EBUS scope has been increasingly used in the gastrointestinal tract (EUS-B). Use of EUS-B-FNA for the establishment of aetiology of EIP is yet not published in the literature.
Fine-needle aspirate from thickened para-oesophageal collection demonstrated C. glabrata on fungal culture. This supported the fungal oesophagitis as one of the causes for EIP. We propose the use of EUS-B-FNA for evaluation of oesophageal and para-oesophageal pathologies.
AUTHOR CONTRIBUTIONAll authors contributed their part in either the management of patient and/or preparation of the manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
留言 (0)