
記住我

Mediastinal lymphatic venous malformation (LVM) is a rare condition that was first described in 1983 by Angtuaco et al.1 It contains both lymphatic and venous components and is considered to be vascular dysplasia. Microscopic examination revealed dilated spaces surrounded by endothelium, which were positively stained for either podoplanin (lymphatic component) or CD34 (venous components).2 The pathogenesis has remained unknown, although there have been a few reports that supported abnormality of vasculogenesis.3 Clinical presentation of mediastinal LVM varies depending on the proportion of lymphatic and venous components, size, location and expansion of the mass. This case report describes a rare case of mediastinal LVM with predominant lymphatic components in a child, which was difficult to diagnose. Chest computed tomography (CT) showed only minimal contrast enhancement in solid part and no venous connection was seen. The patient was successfully treated with surgical resection without complication.
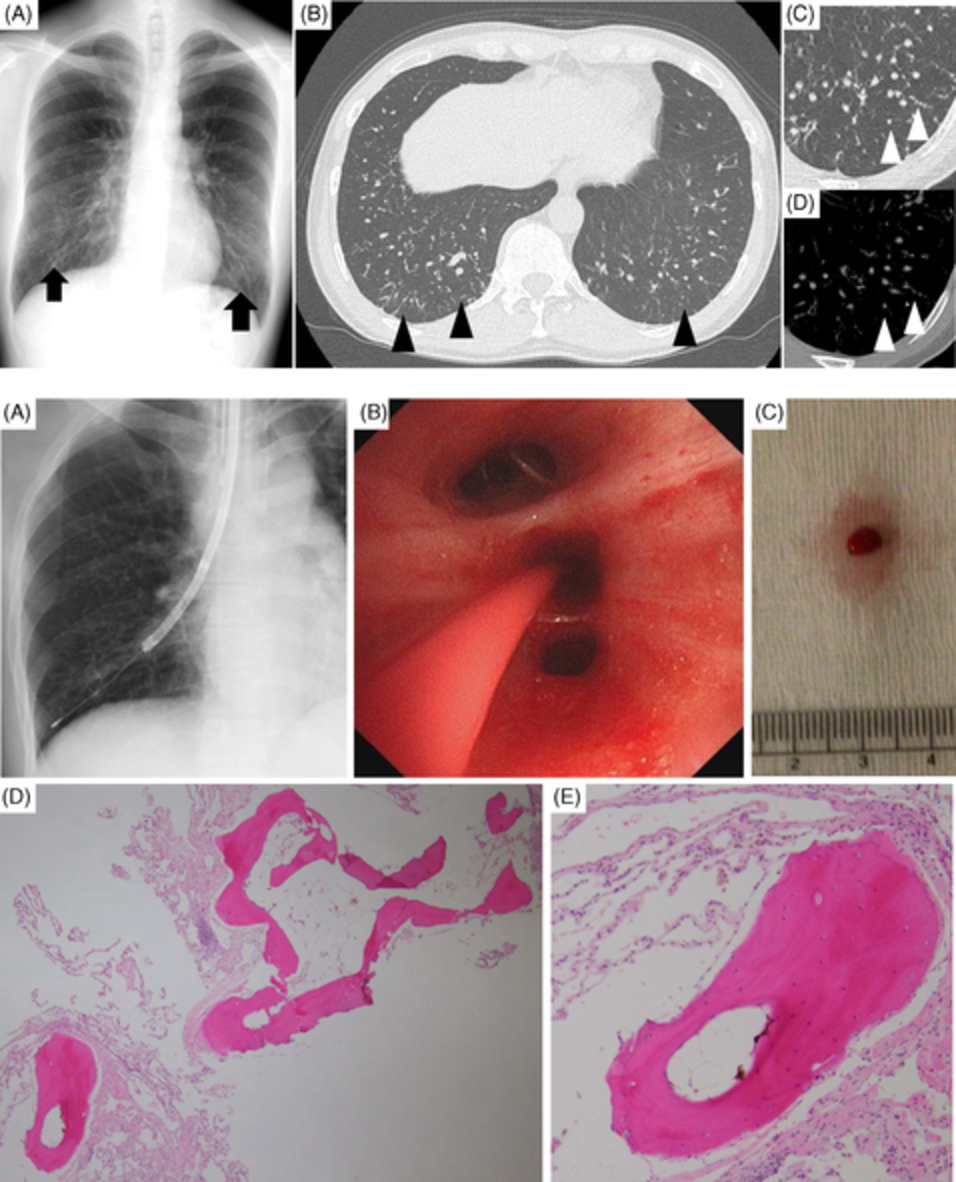
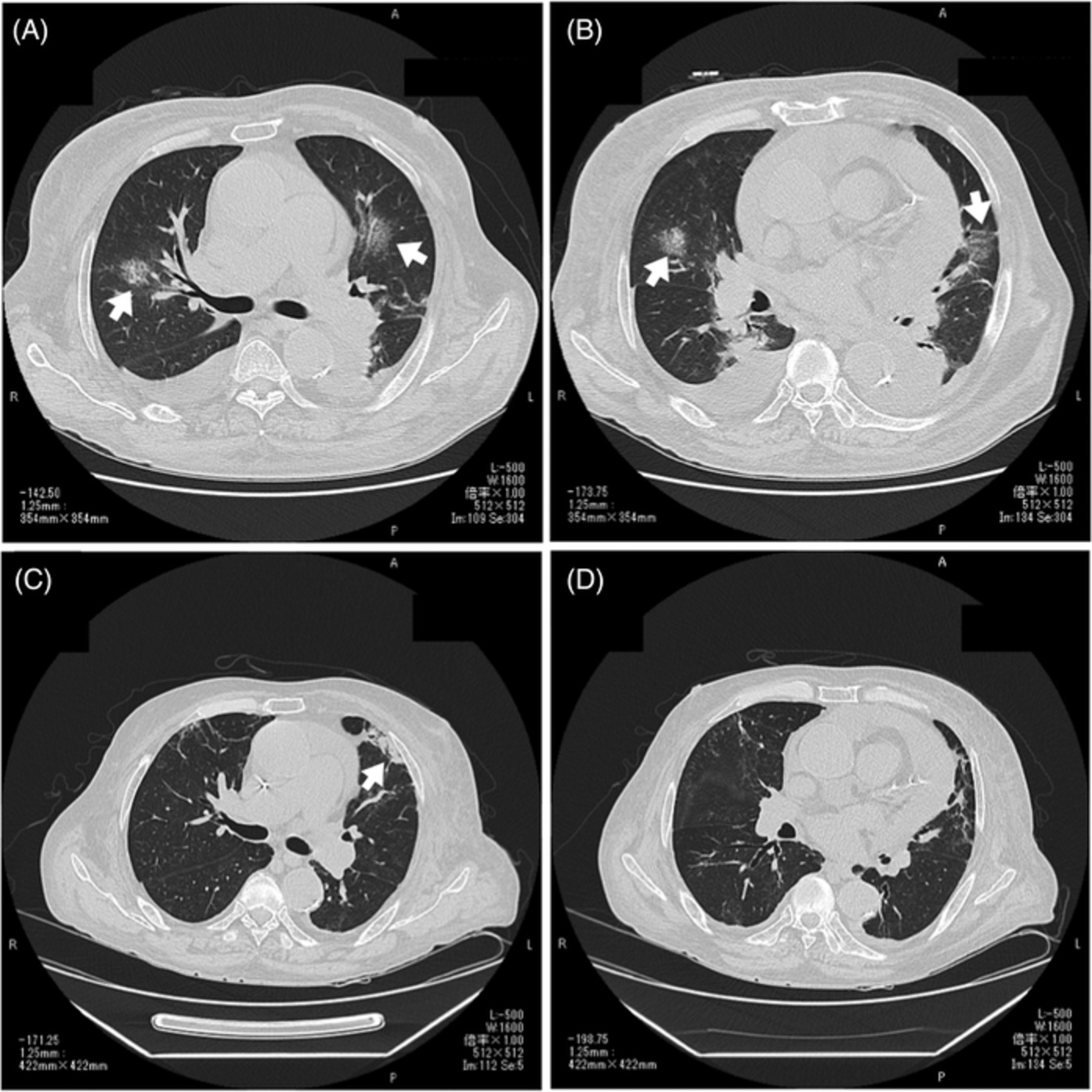
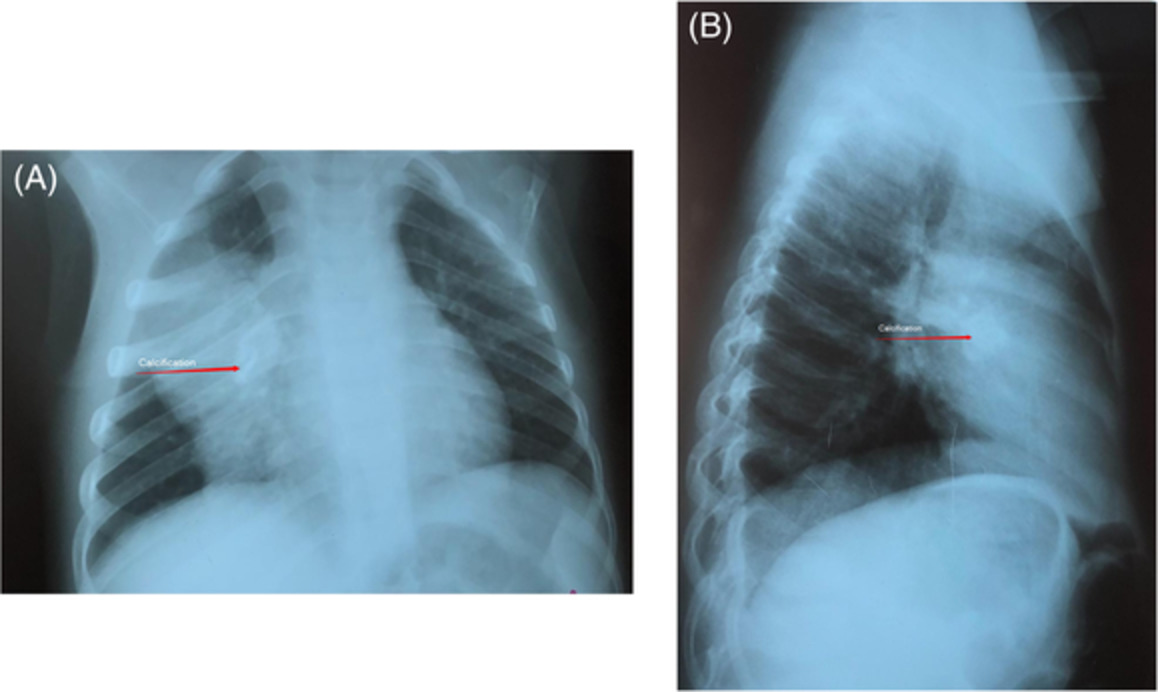
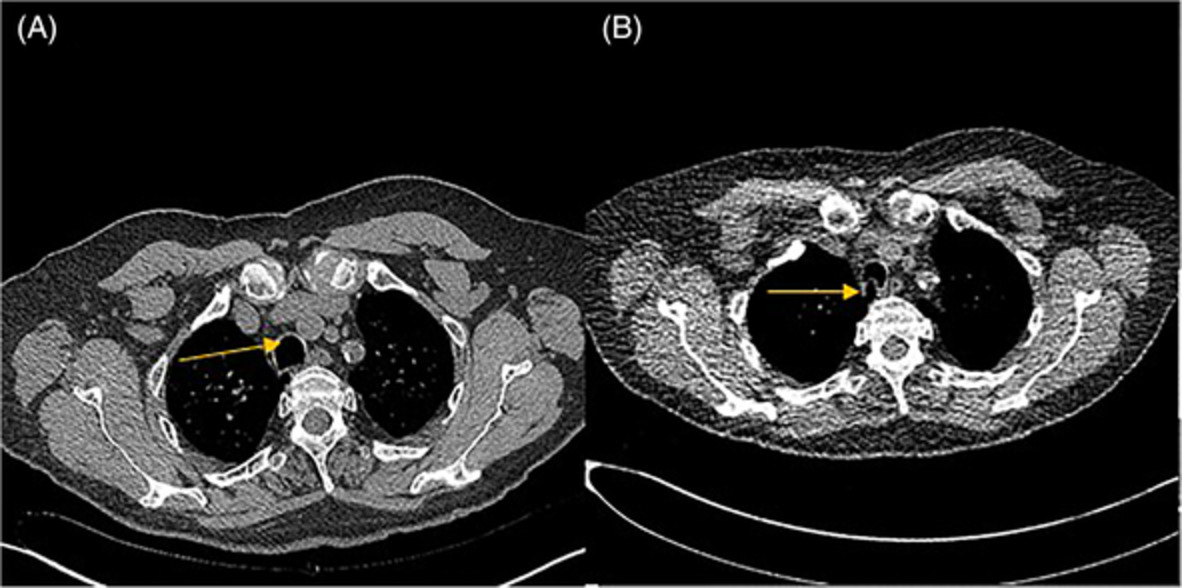
CASE REPORTA 11-year-old boy presented with chest pain after he jumped into a swimming pool. Physical examination showed decreased breath sounds at the left upper lung. Chest x-ray (CXR) posteroanterior view incidentally found a large well-defined border, soft tissue density lesion at the left upper lung field silhouette with descending aorta. The mass shows obtuse angle, no air bronchogram, positive hilar overlay sign and cervicothoracic sign, suggestive of superior mediastinal mass. (Figure 1A). Chest CT revealed a large heterogenous mass containing some fat density, enhancing solid portion, large non-enhancing cystic portion and minimal calcification at the left-sided anterior mediastinum abutting the left-sided thymus gland extended to the posterior mediastinum, measured about 6.7 × 9.6 × 7.8 cm (Figure 1B). His chest pain was resolved after taking analgesic drug.

Chest imaging findings. (A) Chest x-ray found a large well-defined border, soft tissue density lesion at the left upper lung field silhouette with descending aorta. The mass shows obtuse angle, no air bronchogram, positive hilar overlay and cervicothoracic sign, suggestive of superior mediastinal mass. (B) Chest CT in axial and coronal reformatted revealed a large, predominantly cystic lesion in the left side of the superior mediastinum involving anterior and posterior compartments. There are gross fat components and spot calcification within the mass
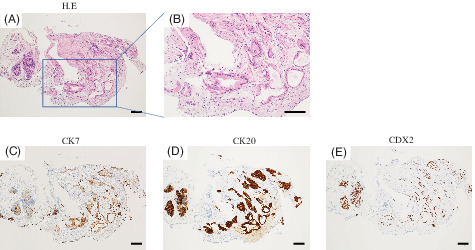
Because of the large size of the mass, the patient underwent video-assisted left thoracotomy with tumour removal. Operative findings were multi-cystic lesion with intralesional haemorrhage. The largest cyst was 10 × 10 cm. The lesion was between the phrenic and vagus nerve. Gross and microscopic findings are shown in Figure 2. Serial section showed that the solid part was finely lobulated fatty tissue interspersed with intercommunicating slit-like spaces and channels, varying from 0.2 to 1 cm in greatest dimension. The interconnecting spaces contained dark brown watery fluid. The cystic part was collapsed, uniloculated cystic tissue, measuring 4.3 × 3.5 × 3.5 cm. A definitive diagnosis was mediastinal LVM. The patient had an uneventful clinical course and was discharged without complication.

Gross and microscopic findings showed mixed cystic and solid tissue. The cystic part was variable-sized, intercommunicating spaces and channels embedded within finely lobulated fatty tissue (solid tissue). The cystic spaces and channels were lined by flat endothelial cells and variably associated with smooth muscle bundles (*) in their walls. Parts of thin-walled cysts without associated smooth muscle occasionally contained lymphoid collection in the walls and filled with proteinaceous fluid (arrow)
DISCUSSIONLVMs, previously called lymphangiohaemangiomas, combine dysplastic lymphatic and venous malformations that are slow-flow vascular malformations. The International Society for the Study of Vascular Anomalies (ISSVA) classified vascular anomalies into two major categories, vascular tumours and vascular malformations. The vascular malformations can be subclassified, based on their predominant vessel involvement, into four subcategories including simple, combined, of major name vessels and associated with other anomalies. LVMs are one of the malformations in combined type, which are defined as two or more vascular malformations found in one lesion.4 They are usually found in the cervical, axillary, head and neck region but rarely found in the mediastinum.5 Among mediastinal LVM, most cases developed predominantly in the anterior mediastinum.6 Patients may be asymptomatic or diagnosed with cough, chest pain, dyspnoea, haemoptysis or venous varicosities. Expanded lesions may compress the surrounding structures.7
Radiological findings of LVM vary in the proportions of lymphatic and venous components. Multidetector CT angiography and magnetic resonance imaging (MRI) are useful for the diagnosis of mediastinal LVM because they can effectively detect slow-flow components and small vessels such as venous connections to the superior vena cava.8 CT scan is excellent for delineating the lesions, their relationships to adjacent structures and may reveal signs of infiltration. Enhancement of venous components is useful for diagnosis if the bolus is followed by sequential scans.8 The MRI imaging of the lymphatic component shows low T1 and markedly high T2 signal intensity without contrast enhancement. The MRI imaging of venous component shows intermediate T1 and high T2 signal intensity with contrast enhancement and may demonstrate phleboliths.9, 10 Imaging studies are helpful in guiding both preoperative differential diagnosis and subsequent plan of treatment.
The definite diagnosis of LVM was made by pathology, but tissue biopsy can confer a risk of bleeding due to the abundant vascular flow. Although LVM have been considered to result from aberrations at some stage of vasculogenesis,3 the histogenesis of vascular malformations remains controversial. Immunohistochemical staining was positive for podoplanin in lymphatic portion and positive for CD34 in vascular portion. The treatment options were surgery and sclerotherapy. Surgery is most successful in isolated, symptomatic LVM or following sclerotherapy. However, it is usually difficult to completely remove the mass; then, recurrence is more common in diffuse form or incomplete excision.5, 11 Fortunately, our patient underwent surgical excision and post-operative CXR was completely resolved, but the patient has to be followed up.
In conclusion, we presented a unique case of a 11-year-old boy with mediastinal LVM presented with chest pain and a mediastinal mass accidentally found on CXR. Definite diagnosis was made by gross and microscopic examination. Our report is a reminder that mediastinal LVM might be considered in the differential diagnosis of mediastinal mass, especially in asymptomatic patients, which are not typical for other tumour-like mediastinal mass. Mediastinal LVM, even rare, should be of concern because biopsy of this lesion may lead to life-threatening bleeding complication.
ACKNOWLEDGMENTSThe authors would like to express gratitude to the patient and the staff of Radiology Department, Faculty of Medicine, Siriraj Hospital Mahidol University, for reviewing chest imaging and to Siriraj Medical Research Center (SiMR) for financial support for publication.
AUTHOR CONTRIBUTIONPrakarn Tovichien and Phatthareeda Kaeotawee drafted the manuscript. All authors contributed to patient care. Prakarn Tovichien revised the manuscript. All authors read and approved the final manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
留言 (0)