Background
Topical forms of nonsteroidal anti-inflammatory drug (NSAIDs) have been developed to lessen systemic adverse effects associated with oral NSAIDs, such as gastrointestinal injury and renal toxicity and currently are commonly to relieve pain from localized musculoskeletal ailments such as epicondylitis, ankle sprains, and knee osteoarthritis.1 In general, they are believed to be well tolerated and appropriate for use as an over-the-counter (OTC) drug without a medical prescription or supervision of health-care professionals.2
We report a case of recurrent peptic ulcer bleeding caused by chronic excessive use of topical diclofenac epolamine patches in an elderly female patient. Despite routine questions regarding past medications, patients might not always accurately remember their medications, especially OTC medications.3 The present case demonstrates that inappropriate use of topical NSAIDs could have serious implications, resulting in substantial morbidity and mortality, as well as increasing health-care costs.4 This report is a reminder that patients often do not disclose the use of OTC drugs, including NSAID patches, which can be possible causes of unexplained refractory peptic ulcers.5
Case presentation
A 68-year-old woman visited our clinic due to tarry stool and was admitted for urgent treatment. The patient reported multiple episodes of recurrent bleeding from a gastric ulcer for 2 months and was treated with endoscopic hemostatic clipping. Her prescribed medicines were amlodipine (5 mg/day), sennoside (12 mg/day), and omeprazole (10 mg/day).
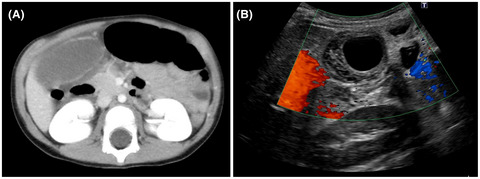
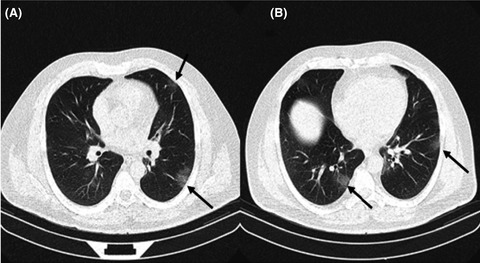
The patient was alert with stable vital signs: blood pressure, 124/78 mmHg; heart rate, 78 b.p.m.; and body temperature, 36.2°C. Laboratory test values included white blood cell count of 1.21 × 103/μl and platelet count of 870 × 103/μl. Hemoglobin levels were reduced to 5.8 mg/dl. Her other blood chemistry results (creatinine and blood urea nitrogen) were within normal range. Her serum gastrin level was 34 pg/ml (normal range, 0–180 pg/ml). Computed tomography revealed no pneumoperitoneum or ascites in the abdominal cavity. Upper gastrointestinal endoscopy on the day of admission demonstrated a large ulcer on the anterior corpus of the stomach with diffuse pseudomembranes. Biopsied ulcer specimens showed ulcerated gastric mucosa with fibrinonecrotic debris and acute inflammation, exudates, and reactive epithelial changes. Tests for Helicobacter pylori infection were negative. Before admission, the patient had been going about her life as usual, with no abnormal stressors. The patient disclosed she had using a large number of diclofenac patches (20 mg × eight sheets together in a day) for more than 3 months to ameliorate pain in her back and shoulder. The use of an excessive number of diclofenac patches was a potential cause of her gastric ulcer. The patient was treated conservatively by discontinuation of diclofenac patches and treatment with a proton pump inhibitor and omeprazole. Repeated gastroendoscopy performed 7 days later showed that her ulcers previously bleeding were healing, but had a largely improved endoscopic appearance.
Discussion
Topically applied NSAIDs provide the benefits of enhanced delivery of local drugs to affected tissues and have a superior safety profile, with lower incidence of systemic adverse effects, compared with oral NSAIDs. Approximately 10%–15% of patients experience adverse effects secondary to topical NSAID application, but these are mostly cutaneous conditions like pruritus and rash at the application site.2 For topical NSAIDs, skin reactions are the most frequent, accounting for 95% of all events.6 Adverse gastrointestinal drug reactions are very rare with topical NSAIDs, compared to 15% incidence for oral NSAIDs.2 To the best our knowledge, only five cases of gastrointestinal bleeding due to NSAID patches have been previously reported in Japan (Table 1). Although critical complications are rare, topical NSAIDs should be used carefully in patients with other risk factors for upper gastrointestinal bleeding, including smoking, advanced age, concomitant use of oral corticosteroids or anticoagulants, history of peptic ulcer, and the presence of H. pylori infection. Sudden impairment of renal function could occur after modest exposure to topical NSAIDs; patients with this history should be cautioned to avoid these medications regardless of the administration route or dose.7
Table 1.
Cases of gastrointestinal bleeding due to topical nonsteroidal anti-inflammatory drug use (review of Japanese reports)
First author
Year
Age (years)
Gender
Medicine
Dose/day
Site of ulcer
Oda
2021
68
Female
Ketoprofen
160 mg
Stomach
Shirohata
2020
70s
Female
Diclofenac
210 mg
Ileum
Kimoto
2020
63
Female
Ketoprofen
160–200 mg
Stomach
Aoyama
2019
70
Male
Flurbiprofen
240 mg
Ileum
Nagano
2017
N/A
N/A
Esflurbiprofen
N/A
Stomach
Hirose
2017
74
Male
Ketoprofen
160 mg
Ileum
Abbreviation: N/A, not available.
As percutaneous absorption of NSAIDs could be influenced by the properties of the skin, dose, and method of administration, local tissue concentrations after topical application of NSAIDs are highly variable. However, overall concentrations in tissues including the tendons, muscles, and subcutis after topical NSAID application are regularly several times higher than those observed after oral intake.8 Pharmacokinetic elimination data showed that NSAIDs remain in the tissue locally much longer than after oral administration, which can be explained by the presence of a tissue reservoir.9 Topical NSAIDs are absorbed gradually and in small amounts into the systemic circulation; maximal plasma NSAID concentration and bioavailability following topical application are normally less than 5% and 15%, respectively, compared with identical oral dose.2
Our experience illustrates that undisclosed use of topical NSAIDs could be the cause of an unexplained peptic ulcer. We must include questions regarding nonprescription medicines, supplements and herbals remedies. However, undisclosed use of NSAIDs is well recognized. Patients remember only approximately half of their medications, and recall of OTC NSAIDs could be lower than recall of prescription drugs.5 Surprisingly, it is estimated that approximately 30% of patients with peptic ulcers who denied NSAID use on interview had been found to have taken NSAIDs based on suppressed levels of serum thromboxane B2.10
A limitation of this study is a lack of measurement of plasma diclofenac or thromboxane concentrations. Although we do not have evidence that the topical NSAID caused gastric ulcer bleeding in this patient, immediate improvement of the symptoms without recurrence of peptic ulcers after discontinuation of these patches could support our diagnosis.
In conclusion, inappropriate use of topical NSAID patches can be a cause of peptic ulcer bleeding. Immediate discontinuation of NSAID patches combined with proton pump inhibitors resulted in an early recovery. Patients should be questioned, particularly about the use of OTC medications that might include topical NSAID patches.
Disclosure
Approval of the research protocol: N/A.
Informed consent: Informed consent was obtained from the patient to publish this case report.
Registry and registration no. of the study/trial: N/A.

留言 (0)