
記住我
Immersion pulmonary edema (IPE) is an acute pulmonary edema that develops during scuba diving, snorkeling, breath-hold diving, or intense activities.1, 2 In a survey of 1,250 divers, 5 of the 460 responders (1.1%) reported symptoms consistent with IPE,3 and in another survey of 104,887 US triathlon participants, 20 out of 1,400 (1.4%) responders reported IPE-associated symptoms during or after swimming.4 In an open sea swimming trial, IPE occurred in 70 (1.8%) young, healthy men aged 18–19 years.5 More than 20 cases of IPE are reported yearly among US Navy combat swimmers undergoing intense training.6 Risk factors include age more than 50 years, female sex, heart disease, excess pre-exercise fluid intake, use of tight wetsuits, and cold exposure.7 Most patients with IPE show improvement within 72 h with rest and oxygen administration under atmospheric pressure. Compiling several case reports of IPE, 21 out of 37 patients had the second episode of IPE,8 and Koehle et al.9 reported that patients had a prior or subsequent episode in at least 13 of 60 cases involving scuba diving, endurance swimming, and breath-hold diving.
Although alcohol is a known risk factor for recreational near-drowning incidents,10 some divers consume alcohol to excess around the time of a dive.11 In one reported case, excessive alcohol intake almost certainly caused decompression sickness,12 which is an important complication during diving; however, there have been no reports that alcohol is a direct cause of IPE. We herein present the case of a novice scuba diver who developed apnea due to IPE during recreational diving after heavy alcohol intake but who recovered without sequelae after prompt life-saving treatment.
CASE PRESENTATIONA 71-year-old man (height, 162 cm; body weight, 57 kg; body mass index, 21.7 kg/m2) had been diagnosed with hypertension at the age of 45 years. Amlodipine (2.5 mg daily) therapy was initiated at 61 years of age; antihypertensive therapy was discontinued at 63 years of age.
Diving situation and onsetOn 1 April, 20XX, after obtaining a diving certificate, the patient participated in the Okinawa diving tour and performed two recreational diving per day on 3, 4, and 6 April. On 6 April, he consumed beverages containing approximately 253 g of alcohol. He then went for his tenth dive, and he wore a 5-mm-thick neoprene wetsuit. The ambient temperature, water temperature, transparency, and tidal current were 26°C, 23°C, 20 m, and 0 m/s, respectively.
The patient hung a dive rope and began slowly diving with the instructor after confirming a residual pressure of 20,594 kPa and weight of 5 kg at 9:15 am. He reached a depth of approximately 20 m at a dive speed of 2 m/min, and he began to ascend at a similar speed at 9:25 am. At a depth of 12 m, the patient used a hand signal at 9:40 am to inform the instructor that he was experiencing physical discomfort. The patient displayed shallow breathing; however, the instructor confirmed a residual pressure of 12,749 kPa. The patient appeared to be panicked and in pain. He signaled to the instructor that he wanted to ascend and began ascending at a rate of 4 m/min. The patient and the instructor resurfaced at 9:43 a.m. The instructor removed the patient’s regulator mask; the patient produced pink foamy sputum and was not breathing, with no confirmed pulse. While being towed to a ship 5 m away, the instructor performed mouth-to-mouth ventilation. The patient was taken onboard, cardiopulmonary resuscitation was performed immediately using a pocket mask, and agonal breathing then developed. Incidentally, the estimated no-flow time was approximately 1 min, and the estimated cardiopulmonary resuscitation time was 2–3 min according to the accident report provided by the dive shop.
Clinical courseWhen the medical helicopter crew, consisting of a physician and a nurse, encountered the patient at the port at 10:12 am, his Glasgow Coma Scale score was 3 (E1V1M1), and his systolic blood pressure (BP) and pulse rate (PR) were 230 mmHg and 80 b.p.m., respectively. When inserting an endotracheal tube, the physician noticed a smell consistent with alcohol consumption.
When the ambulance staff physician evaluated the patient at 10:39 am, the Glasgow Coma Scale score was E1VTM1. Vital signs were as follows: axillary temperature, 35.7°C; BP, 225/143 mmHg; PR, 80 b.p.m.; respiratory rate, 30 breaths/min; percutaneous arterial oxygen saturation (SpO2), 95% under 100% oxygen at 10 L/min; and end-tidal carbon dioxide concentration, 36 mmHg measured using a pocket carbon dioxide monitor (WEC-7301 Capno petite; Nihon Kohden). His pupils were 3.5 mm in diameter, and his pupillary light reflex was dull. His wetsuit was cut, and heat restorative measures were initiated.
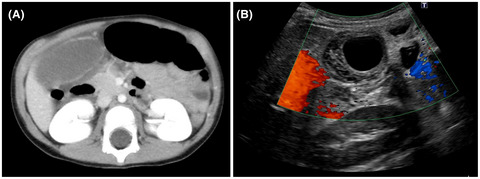
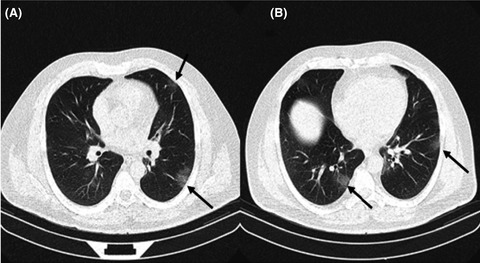
When the patient was brought to the Emergency Department at 10:49 am, his BP and PR were 115/92 mmHg and 70 b.p.m., respectively. No abnormalities were found on electrocardiogram, and echocardiography showed no obvious asynergy or decreased ejection fraction. Chest radiography revealed a butterfly-shaped shadow (Fig. 1A), and chest computed tomography showed thickening of the bronchovascular bundle, bilateral infiltrative lower lobe shadows, and minor bilateral pleural effusions (Fig. 1B, C). During bronchoscopy for the evaluation of possible airway foreign body, a large amount of sandy-brown sputum was aspirated. Based on the P/F ratio of less than 200 (Table 1), the extensive bilateral infiltration on imaging, and normal cardiac function by echocardiography, acute respiratory distress syndrome (ARDS) due to drowning was diagnosed in the Emergency Department. Intermittent positive pressure ventilation was started according to open lung strategy. On day 2 of hospitalization, left ventricular ejection fraction was 71.3%. The white blood cell count was 10,100 cells/μL, and the C-reactive protein concentration was 9.3 mg/dl (Table 1); therefore, we determined that aspiration pneumonia was present, and piperacillin/tazobactam was initiated. The patient was weaned from mechanical ventilation, and the butterfly-shaped radiographic shadow disappeared on day 3 of hospitalization (Fig. 1D). Infiltrative shadows remained in a part of both lower lung fields; however, the patient was discharged without sequelae on day 7 of hospitalization.

Imaging of a 71-year-old man with severe immersion pulmonary edema while scuba diving after heavy alcohol intake. A, Chest radiography on admission, with the patient in the half-sitting position. The image shows large butterfly-shaped shadows in both lungs. The lung pattern is seen to be expanding to the right side. The right costophrenic angle is slightly blunted; however, the cardiothoracic ratio does not appear increased. B, C, Computed tomography images of the lung on admission. Multiple focal ground-glass shadows are apparent bilaterally in the middle lobe; thickening of the bronchovascular bundle and the interlobular septum are observed. D, Chest radiography at day 3 of hospitalization, with the patient in the sitting position. The butterfly-shaped shadow has disappeared; however, the thickening of the right major fissure remains. An infiltrative shadow is observed in the lower right lung field, and the line of the descending aorta overlapping the left fourth arch is obscured.
Table 1. Laboratory data during admission of a 71-year-old man with severe immersion pulmonary edema while scuba diving after heavy alcohol intake Day 0 Day 2 Day 5 Arterial blood gas IPPV, FiO2 0.99 IPPV, FiO2 0.25 Nasal O2 0.5 L/min pH 7.2 7.4 7.4 pCO2 torr 53.0 40.0 42.0 pO2 torr 88.0 82.0 62.0 HCO3 mmol/L 22.2 27.2 28.5 B.E. −5.8 2.8 3.9 Lactate mmol/L 2.8 1.6 0.7 Blood counts White blood cell /μl 6,000 10,100 4,100 Red blood cell ×104/μl 453 365 359 Hemoglobin g/dl 15.4 12.0 12 Platelets ×104/μl 20.7 17.1 15.2 Blood chemistry Sodium mmol/L 127 137 137 Potassium mmol/L 5.0 4.3 3.8 Albumin g/dl 3.6 1.3 3 AST U/L 38 25 19 ALT U/L 21 14 18 LDH U/L 367 288 191 BUN mg/dl 21.1 35.3 13.3 Creatinine mg/dl 1.1 1.5 0.85 Glucose g/dl 262 170 133 CRP mg/dl 0.0 9.3 3.8 Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; B.E., base excess; BUN, blood urea nitrogen; CRP, C-reactive protein; IPPV, invasive positive pressure ventilation; LDH, lactate dehydrogenase.After a detailed interview carried out at a later date, it was determined that the initial symptom was chest discomfort; however, no seawater was aspirated until the patient lost consciousness.
DISCUSSIONBased on the sudden onset of chest symptoms, imaging findings, and prompt weaning from mechanical ventilation, we finally determined that the patient’s diagnosis was IPE. The main causes of IPE were suspected to be the patient’s hypertension and excessive alcohol consumption the night before. The inflammatory reaction that increased on day 2 of hospitalization improved with antibacterial therapy; therefore, it might have been due to aspiration pneumonia as a complication. Although a detailed history was re-recorded through interviews with the patient and the diving instructor, we could not determine the time of seawater aspiration.
Excessive alcohol consumption significantly increases the risk of ARDS. A meta-analysis of 13 studies showed that any measure of high alcohol consumption was associated with a significantly increased risk of ARDS (odds ratio, 1.89; 95% confidence interval, 1.45–2.48), and a sensitivity analysis of 10 studies indicated that this association was attributable primarily to a history of alcohol abuse (odds ratio, 1.90; 95% confidence interval, 1.40–2.60).13 Alcohol abuse enhances pulmonary edema in ARDS, due to increased extravascular lung water and increased pulmonary vascular permeability14, 15 (Fig. 2). Alcohol impairs the alveolar barrier by increasing paracellular leaks and disrupting fluid homeostasis, predisposing the lung to flooding, leading to subsequent “second-hit” injuries such as infection and inflammation.16 From the above, our patient developed IPE as the result of diving with underlying excessive alcohol-induced pulmonary edema. He might have felt the onset of IPE as chest discomfort because he was exposed to a high-pressure environment in this condition (Fig. 2).

Pathophysiological mechanism of immersion pulmonary edema onset in this case.
In animal experiments, ethanol induces increased systemic vascular resistance and heart rate in a dose-dependent manner,17 resulting in increased afterload and increased capillary pressure (Fig. 2). In our patient, vascular resistance might have been increased due to untreated hypertension; therefore, it is possible that afterload was increased (Fig. 2). Alcohol alters the functioning of the autonomic nervous system, and serum alcohol concentrations greater than 100 mg/dl weaken cardiac contractility in healthy young adults18; therefore, the patient’s cardiac output may have been reduced by consumption of a large amount alcohol the night preceding the diving activity (Fig. 2). Moreover, a diving reflex, by itself, increases stroke volume and peripheral vascular resistance, with a resultant increase in blood pressure.19 Although cardiac output was decreased to some degree, ARDS was clinically diagnosed based on the history of exposure to a high-pressure environment and heavy alcohol consumption. Based on the above, the decrease in cardiac output and the increase in vascular resistance due to ethanol, superimposed on the underlying untreated hypertension, led to a hypertensive environment that triggered IPE.
In this case, acute lung edema was considered secondary to heavy drinking. Therefore, IPE should be considered a possibility in rescue victims who have had excessive alcohol intake in advance.
AcknowledgmentsWe thank Mr. Yasuo Uchihara, the representative of the Pink Marlin Club dive shop, for providing valuable information.
Funding informationNo funding information provided.
DisclosureApproval of the research protocol: N/A.
Informed consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
References
1Wilmshurst PT, Nuri M, Crowther A, Webb-Peploe MM. Cold-induced pulmonary oedema in scuba divers and swimmers and subsequent development of hypertension. Lancet 1989; 333: 62– 5. 2Davis FM. Immersion pulmonary edema-facts and fancies. Undersea Hyperb. Med. 2016; 43: 744– 5. 3Pons M, Blickenstorfer D, Oechslin E, et al. Pulmonary edema in healthy persons during scuba diving and swimming. Eur. Respir. J. 1995; 8: 762– 7. 4Miller CC III, Calder-Becker K, Modave F. Swimming-induced pulmonary edema in triathletes. Am. J. Emerg. Med. 2010; 28: 941– 6. 5Adir Y, Shupak A, Gil A, et al. Swimming-induced pulmonary edema: clinical presentation and serial lung function. Chest 2004; 126: 394– 9. 6Mahon RT, Kerr S, Amundson D, Parrish JS. Immersion pulmonary edema in special forces combat swimmers. Chest 2002; 122: 383– 4. 7Kumar M, Thompson PD. A literature review of immersion pulmonary edema. Phys. Sportsmed. 2019; 47: 148– 51. 8Cochard G, Arvieux J, Lacour JM, Madouas G, Mongredien H, Arvieux CC. Pulmonary edema in scuba divers: recurrence and fatal outcome. Undersea Hyperb. Med. 2005; 32: 39– 44. 9Koehle MS, Lepawsky M, Mckenzie D. Pulmonary oedema of immersion. Sports Med. 2005; 35: 183– 90. 10Sheldrake S, Pollock NW. Alcohol and diving. In: D Steller, L Lobel (eds). Diving for Science 2012—Proceedings of the American Academy of Underwater Sciences 31st Scientific Symposium; 20– 29. 11Dowse MSL, Cridge C, Shaw S, Smerdon G. Alcohol and UK recreational divers: consumption and attitudes. Diving Hyperb. Med. 2012; 42: 201– 7. 12Davis M. Alcohol and scuba diving. Diving Hyperb. Med. 2012; 42: 193. 13Simou E, Leonardi-Bee J, Britton J. The effect of alcohol consumption on the risk of ARDS: A systematic review and meta-analysis. Chest 2018; 154: 58– 68. 14Berkowitz DM, Danai PA, Eaton S, Moss M, Martin GS. Alcohol abuse enhances pulmonary edema in acute respiratory distress syndrome. Alcohol Clin. Exp. Res. 2009; 33: 1690– 6. 15Corgie L, Huiban N, Pontier JM, Brocq FX, Boulard JF, Monteil M. Diving accident evacuations by helicopter and immersion pulmonary edema. Aerosp. Med. Hum. Perform 2020; 91: 806– 11. 16Jeffers L, Nguyen T, Staitieh BS, Koval M. Increased hydrostatic fluid pressure sensitizes the alcoholic lung to pulmonary edema. Am. J. Respir. Crit. Care. Med. 2020; 201: A4103. 17Brackett DJ, Gauvin DV, Lerner MR, Holloway FA, Wilson MF. Dose- and time-dependent cardiovascular responses induced by ethanol. J. Pharmacol. Exp. Ther. 1994; 268: 78– 84. 18Lang RM, Borow KM, Neumann A, Feldman T. Adverse cardiac effects of acute alcohol ingestion in young adults. Ann. Int. Med. 1985; 102: 742– 7. 19Wittmers LE Jr, Pozos RS, Fall G, Beck L. Cardiovascular responses to face immersion (the diving reflex) in human beings after alcohol consumption. Ann. Emerg. Med. 1987; 16: 1031– 6.
留言 (0)