
記住我

Good's syndrome (GS), also known as immunodeficiency syndrome associated with thymoma, is a rare primary immunodeficiency disease.1 It was discovered and first reported by Robert Good in 1954. Although there are reports of childhood-onset cases, GS is characterized by adult-onset immunodeficiency associated with thymoma, and its clinical manifestations are recurrent infections, autoimmunity diseases and so on.2 Diffuse panbronchiolitis (DPB) is chronic inflammatory disease of the airways, which predominantly affects East Asians, mainly involving respiratory bronchioles.3 Japanese scholars have reported extensively about GS combined with DPB or DPB-like pulmonary manifestation. However, such reports are rare in China.4, 5 As clinicians generally lack understanding of GS and DPB,6 in order to improve the comprehensive understanding of GS, we report here a case of GS with DPB as the prominent manifestation and carry out the literature review accordingly.
CASE REPORTA 67-year-old female farmer was admitted in late March 2016 due to recurrent cough and expectoration for 3 years, aggravated with shortness of breath for 10 days. The patient had paroxysmal cough 3 years prior to her admission, the tone was not high and there was no obvious time regularity, showing no correlation with body position and food intake. The patient coughed with moderate amounts of white phlegm, and the cough worsened after weather change and catching cold. She was hospitalized in other hospitals many times and was diagnosed with chronic obstructive pulmonary disease (COPD) through pulmonary function test. After receiving relevant treatment, her condition improved slightly, but she did not take medication consistently. Ten days before admission, the above symptoms recurred after catching cold, and the patient coughed a large amount of yellow purulent sputum, sometimes with blood. She was short of breath at rest, unable to lie on the back and accompanied by fatigue, anorexia and night sweat; she had no fever and no limb oedema. Three days of intravenous infusion in the local clinic was not effective (details unknown). Since the onset of the disease, the patient had lost about 10 kg of weight. In 2012, she underwent resection of thymoma in another hospital (details unknown). She denied smoking history, and no obvious abnormalities were found in her personal, menstrual, obstetrical or family history. Physical examination showed a body temperature of 36.2 °C, pulse rate of 90 bpm, respiratory rate of 26 bpm, blood pressure 140/80 mmHg and peripheral capillary oxygen saturation (SpO2) of 94% (oxygen flow 3 L/min). She had a clear mind; shortness of breath; slight cyanosis of lip; no palpable lymph nodes in the neck, supraclavicular and axillary regions; emphysema sign; wheezing mainly in the expiratory phase and heard in both lungs; and obvious moist rales heard in both lower lungs. Her heart rate was 90 bpm and had irregular rhythm, but no murmur, no swelling of both lower limbs or no clubbed fingers (toes).
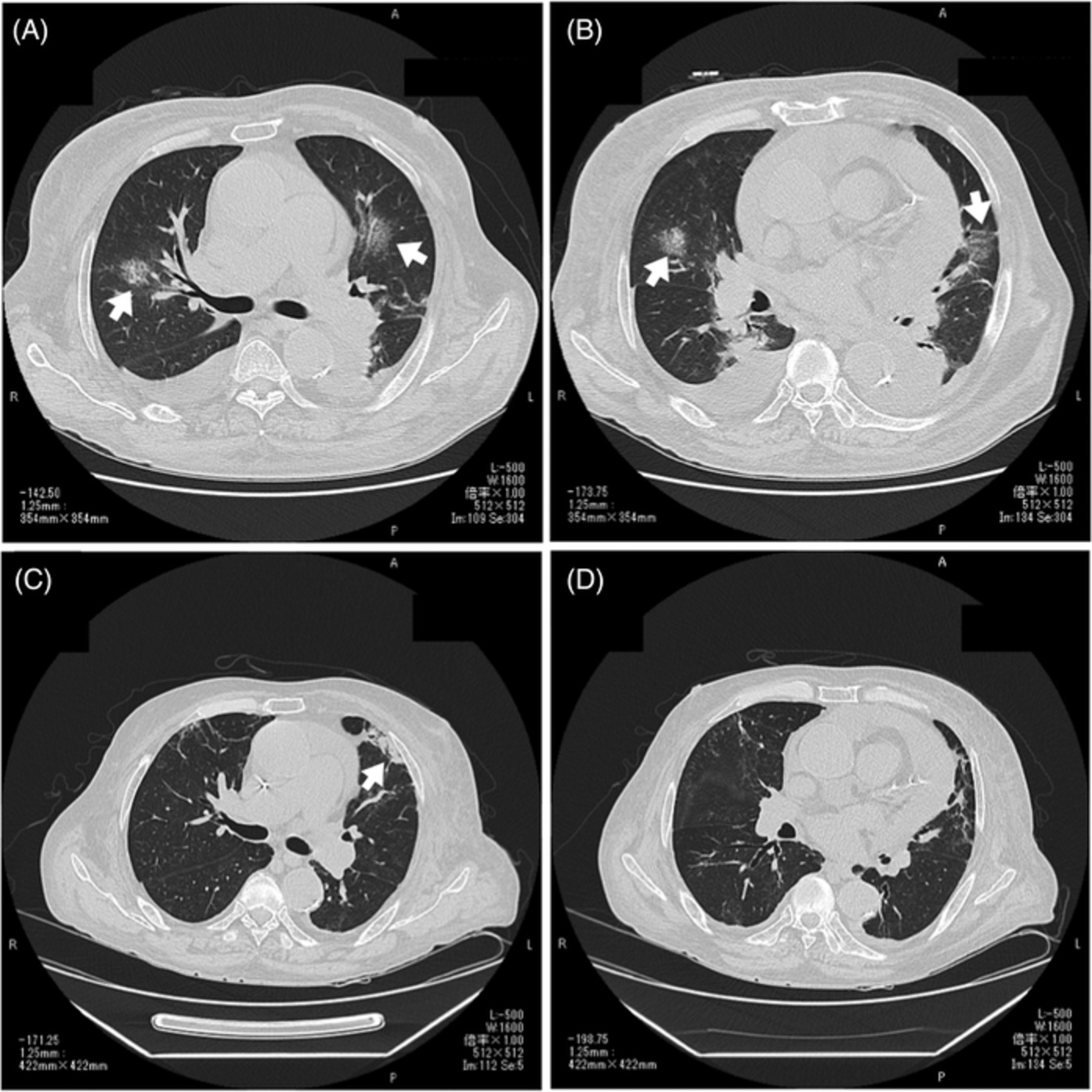
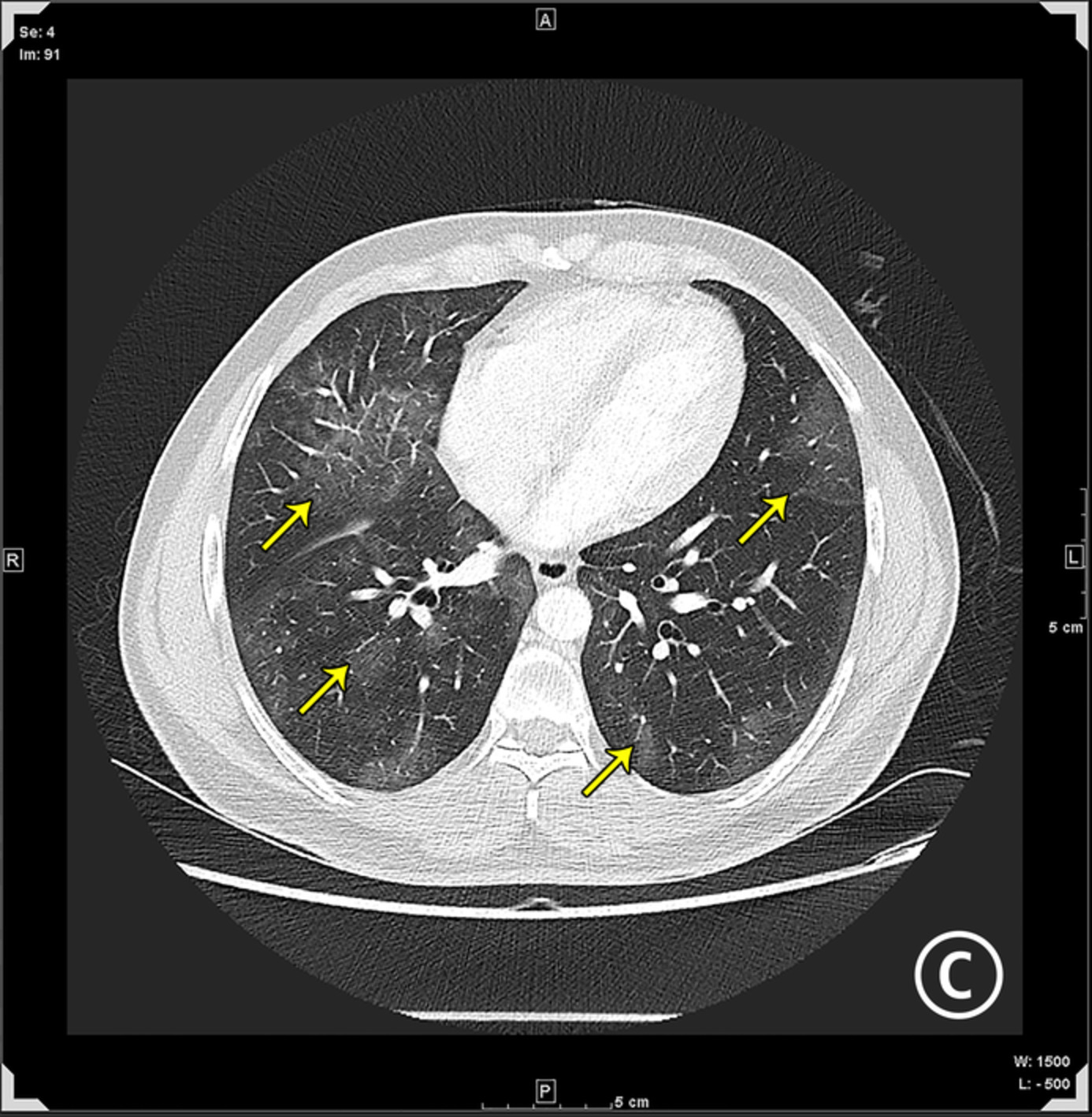
Her laboratory findings on admission (Table 1) revealed an increase in the white blood cell count (WBC), high-sensitivity C-reactive protein (hs-CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST) and total haemolytic complement activity (CH50). Immunoglobulin G (IgG), B lymphocytes and CD4+ T lymphocytes were significantly decreased. Bedside electrocardiogram revealed sinus rhythm and frequent atrial premature beats. Chest computed tomography (CT) scan showed diffuse centrilobular nodules in both lungs, with fuzzy boundaries and tree-in-bud sign (Figure 1). CT of the paranasal sinus showed inflammation of the right maxillary sinus (Figure 2). Sputum smear showed Gram-negative bacilli+ + + and Gram-positive streptococcus+, but no fungal spores were found. The sputum cultures revealed the growth of Pseudomonas aeruginosa without fungi; acid-fast bacilli were not found in four sputum smears. Vasculitis antibodies were negative. Tumour markers, serum carcinoembryonic antigen (CEA), alpha fetoprotein (AFP), cytokeratin fraction 21-1(CYFRA 21-1) and neuron-specific enolase (NSE), were normal. Pulmonary function test showed moderate to severe obstructive pulmonary ventilation dysfunction (forced expiratory volume in 1 s percent predicted [FEV1 %pred] was 55.61%, the ratio of the FEV1 to the forced vital capacity [FEV1/FVC] was 56.34%) and negative bronchial dilation test results.
TABLE 1. Laboratory tests on admission List Standard Value Blood gas analysis (oxygen inhalation 3 L/min) pH 7.35–7.45 7.406 PaCO2 (mmHg) 35–45 52.9 PaO2 (mmHg) 80–100 70.3 SaO2 (%) 95–98 94.5 Blood routine WBC (109/L) 3.97–9.15 14.42 N (%) 50–70 83 L (%) 18–40 8.7 hs-CRP (mg/L) 0–6 61.0 ALT (U/L) 9–50 107.0 AST (U/L) 9–50 78.0 Detection of immunoglobulins IgG (g/L) 8–17 4.7 CH50 (U/ml) 25–75 104.00 Lymphocyte subsets CD3+ T lymphocytes (/μl) 723–2737 557 CD4+ T lymphocytes (/μl) 404–1612 262 CD8+ T lymphocytes (/μl) 220–1129 351 NK (/μl) 84–724 93 B lymphocytes (/μl) 80–136 51 Infection PPD skin test 4 × 5 mm T-SPOT.TB Negative Galactomannan test Negative (1,3)-β-d-Glucan test Negative MP-Ab Negative CP-Ab Negative HIV-Ab Negative Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; CH50, total haemolytic complement activity; CP-Ab, Chlamydia pneumonia antibody; HIV-Ab, HIV antibody; hs-CRP, high-sensitivity C-reactive protein; IgG, immunoglobulin G; L, lymphocyte; MP-Ab, Mycoplasma pneumonia antibody; N, neutrophil; NK, natural killer cell; PaCO2, partial pressure of carbon dioxide in artery; PaO2, partial pressure of oxygen in artery; PPD, purified protein derivative; SaO2, arterial oxygen saturation; T-SPOT.TB, T-cell spot of tuberculosis assay; WBC, white blood cell.
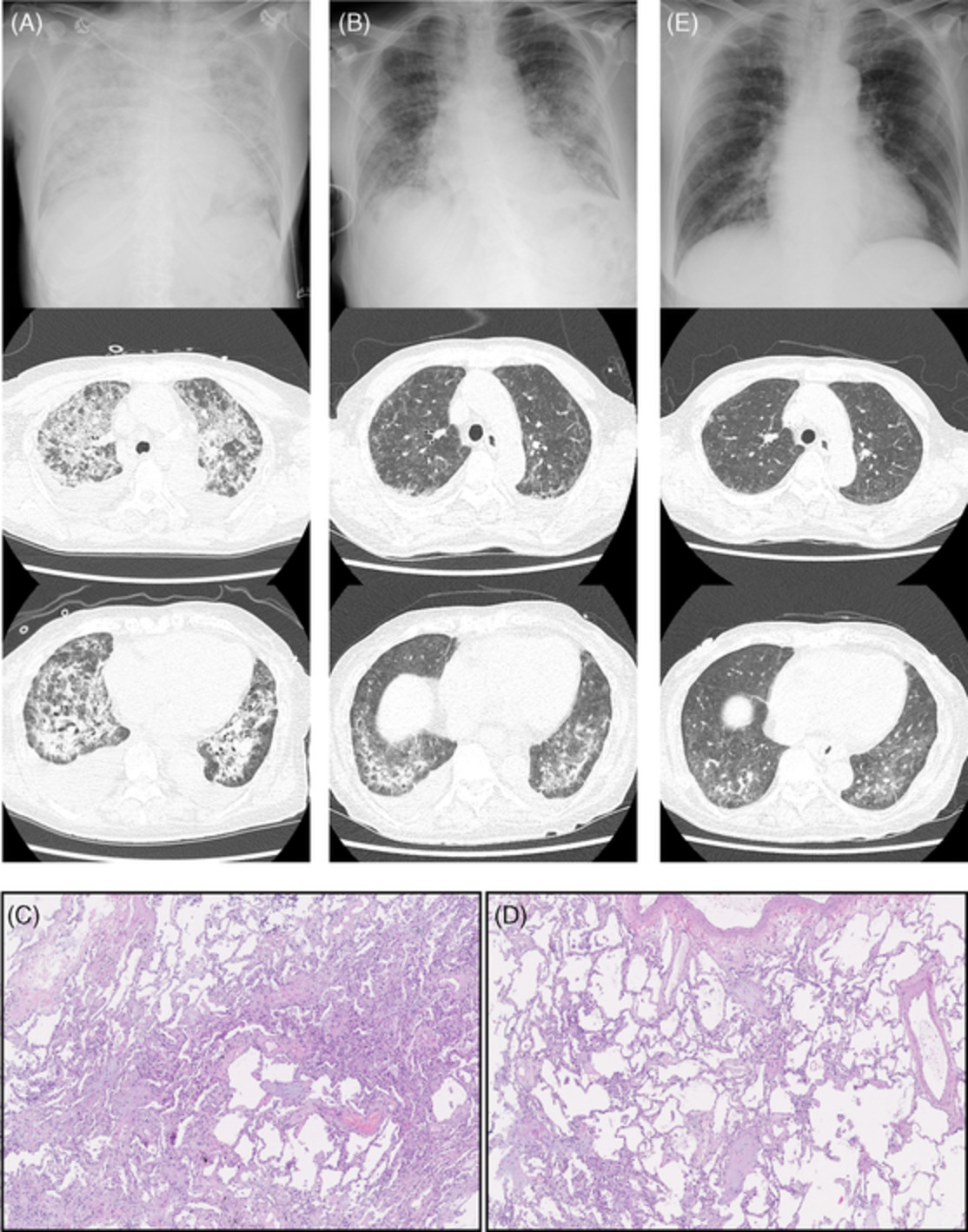
Chest computed tomography (CT) images: (A–C) Centrilobular nodules diffusely distributed in both lungs on chest CT scan in late March 2016, with fuzzy boundaries and tree-in-bud sign. (D–F) Images of chest CT (re-examination) in early April 2016, showing that the centrilobular nodules in both lungs had significantly reduced. (G–I) Images of chest CT in mid-January 2018, showing that the centrilobular nodules in both lungs had disappeared

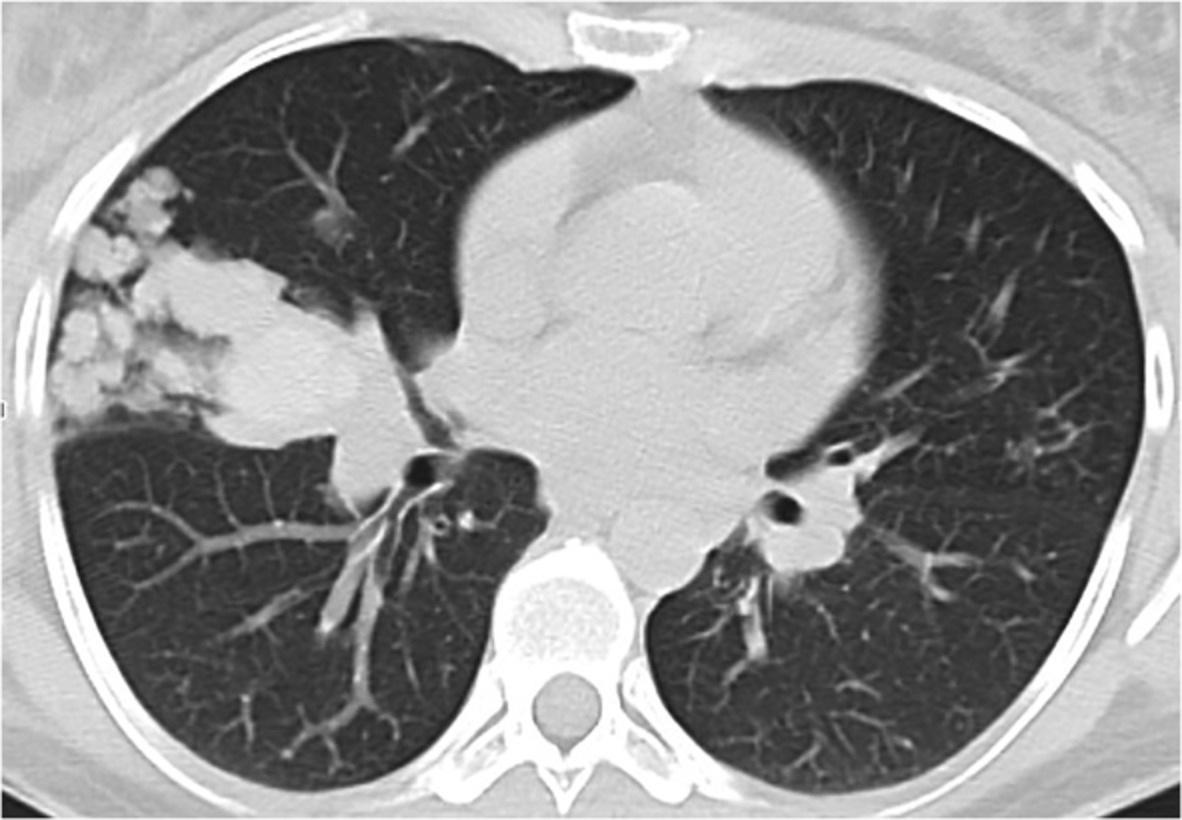
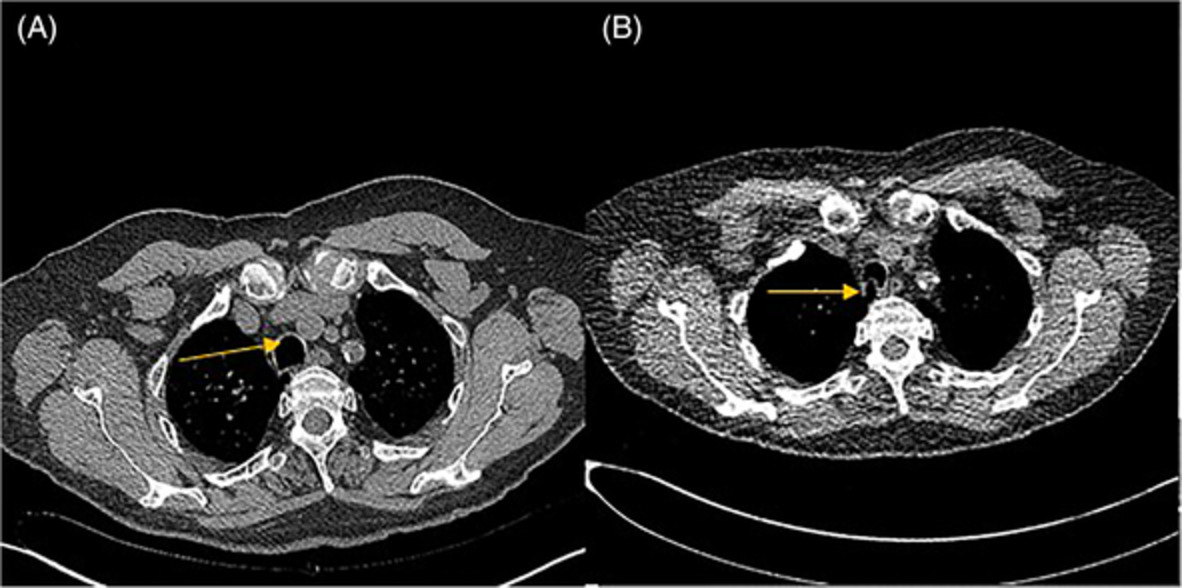
Computed tomography image of paranasal sinus: inflammation of right maxillary sinus
Referring to Li et al.,7 the patient's symptoms improved after 2 weeks of intravenous administration of azithromycin (0.5 g/day) while using piperacillin-tazobactam for P. aeruginosa infections. A blood gas analysis (oxygen inhalation 2 L/min) in early April 2016 showed pH 7.391, PaCO2 (partial pressure of carbon dioxide in artery) 39.2 mmHg, PaO2 (partial pressure of oxygen in artery) 72.2 mmHg and SaO2 (arterial oxygen saturation) 94.5%. Routine blood tests showed WBC 3.36 × 109/L, neutrophils 47.1%, lymphocytes 8%, hs-CRP 2.6 mg/L, ALT 35.0 U/L, AST 22.0 U/L and normal renal function. Chest CT scan (re-examination) in early April 2016 showed that the centrilobular nodules in both lungs were significantly reduced (Figure 1). The patient stopped taking piperacillin-tazobactam but continued taking azithromycin (0.5 g, qod) for a total course of 1 year, and the chest CT scan (re-examination) in the local hospital showed that there were no obvious nodules in both lungs (no image). The administration of azithromycin was therefore stopped. In mid-January 2018, the patient came to our hospital for follow-up examination. The chest CT scan showed that the centrilobular nodules in both lungs had disappeared (Figure 1). The final diagnosis included: (1)GS, (2) DPB (Stage 2) and (3) thymoma after surgery.
DISCUSSIONGS is characterized by thymoma combined with adult-onset immunodeficiency, combined (B and T lymphocytes) immunodeficiency including hypogammaglobulinaemia (decreased IgG, IgA, IgM), low or absent peripheral blood B lymphocytes, decreased CD4+ T lymphocytes, inverted CD4+/CD8+ T-cell ratio and so on.8 Most GS patients are aged 40–70 years, and although there is no significant gender difference,9 more Chinese patients are female.2 The patient in this case had a history of thymoma, decreased IgG and significantly decreased B lymphocytes and CD4+ T lymphocytes, which were consistent with the diagnosis of GS. The patient was a woman aged 67 at diagnosis, which was also consistent with the literature report.
The main clinical manifestations of GS include thymoma, infection, gastrointestinal manifestations (diarrhoea) and autoimmune manifestations (myasthenia gravis, pure red cell aplasia and oral lichen planus).2 The diagnosis of thymoma may occur before, after or during other clinical manifestations.2 The most common clinical manifestation is recurrent respiratory infection, especially lower respiratory tract infection.2, 8 Bronchial wall thickening and tree-in-bud sign may appear on the lung CT scans of GS patients in the early stage, suggesting bronchiolar lesions.10 Japanese scholars have reported extensively about GS combined with DPB or DPB-like pulmonary manifestation.4, 5 The mechanism of DPB presentation in GS patients is not completely clear. Studies have suggested that the over-reaction of lymphocytes associated with human leucocyte antigen-B54 (HLA-B54) in respiratory bronchioles and the recurrent and/or persistent bacterial infection caused by thymomas-induced reduction in the immunocompetence of B lymphocytes are related.5
DPB is a rare chronic inflammatory disease affecting the respiratory bronchioles. It was first described and reported by Japanese scholars in 1969. Most cases occurred in East Asia.3 It is considered that DPB involves many factors such as heredity, immunity, environment and infection. Some HLA types are related to the disease, such as HLA-B54 in Japanese patients and HLA-A11 in Korean patients.11 Typical manifestations of DPB include chronic cough, expectoration and exertional dyspnoea, history of chronic sinusitis, high titre of serum cold agglutination test, centrilobular nodule shadow with tree-in-bud sign widely distributed in both lungs on chest CT scan and so on.11, 12 Akira et al.13 classified the patients into four stages according to the radiographic findings of DPB: Stage 1, diffuse centrilobular nodules; Stage 2, tree-in-bud sign; Stage 3, bronchiectasis in peripheral areas; and Stage 4, bronchiectasis in the central area. The pathological features of DPB are full-thickness respiratory bronchiolitis with infiltration of lymphocytes, plasma cells and so on. In some patients, clusters of foamy macrophages can be seen in the bronchioles and lung tissues, and the peripheral bronchiectasis may occur in the late stage of the disease.14 The clinical diagnosis of DPB usually requires no pathological examination of lung tissues, and the current diagnosis mainly refers to DPB diagnostic criteria formulated by the Ministry of Health and Welfare of Japan in 1998.3 The patient described here had recurrent cough, expectoration and right maxillary sinusitis; chest CT scan showed diffuse centrilobular nodules with tree-in-bud sign in both lungs; pulmonary function test showed moderate to severe obstructive pulmonary ventilation dysfunction (FEV1 %pred was 55.61%, and FEV1/FVC was 56.34%); blood gas analysis (oxygen inhalation 3 L/min) showed PaO2 70.3 mmHg; there were obvious moist rales in both lower lungs; all of which were consistent with DPB (Stage 2).
Chinese literature shows that most patients were misdiagnosed as chronic bronchitis, COPD or other lung diseases before diagnosis.4, 12, 15 The presence of sinusitis and the isolation of P. aeruginosa in the sputum are often associated with DPB, and the understanding of such association may improve the diagnosis.4, 16 The patient in this case had recurrent cough and expectoration for 3 years. Before the diagnosis of DPB, she was misdiagnosed as having COPD, which may be related to clinicians' insufficient understanding of DPB.4, 12, 15 Chinese DPB patients have a low positive rate of the serum cold agglutination test,7, 17, 18 and the patient in this case was negative in such test, further confirming that the difference in laboratory test results between Chinese patients and Japanese patients of DPB may be related to ethnic differences. This would suggest that the diagnostic significance of serum cold agglutination test for Chinese DPB patients is not as important as for Japanese patients.7, 14
A retrospective analysis of 81 patients with histologically confirmed DPB showed that P. aeruginosa was cultured in the sputum of 22% of patients.3 Four years after diagnosis, the detection rate of P. aeruginosa in the sputum increased to 60% on average.3 The analysis of DPB cases in China showed that the detection rate of P. aeruginosa in patients' sputum fluctuated between 46.2% and 60%.17 The sputum cultures of the patient in this case revealed the growth of P. aeruginosa, which was consistent with China's domestic reports. Once DPB is diagnosed, macrolides should be used as early as possible. The first-line regimen is oral administration of erythromycin (400–600 mg/day). If the first-line regimen is ineffective or has high side effects, the 14-membered ring clarithromycin (200–400 mg/day, orally), roxithromycin (150–300 mg/day, orally) or the 15-membered ring azithromycin3 can be used; azithromycin is recommended because of its rapid onset, obvious curative effect, fewer adverse reactions and good patient compliance.7, 19 Termination of treatment can be considered when the centrilobular nodules in lungs disappear on chest CT scan, and the treatment time ranges from 6 months to 2 years.20, 21 After 2 weeks of treatment with azithromycin, the patient's symptoms were improved, and the centrilobular nodules in both lungs were significantly absorbed, suggesting the efficacy of the treatment. After a total course of treatment with azithromycin for 1 year, chest CT scan (re-examination) showed that the centrilobular nodules in both lungs had disappeared, and azithromycin was stopped. Long-term treatment (at least 6 months) with low-dose macrolide antibiotics has increased the 10-year survival rate of DPB patients to over 90%.21
GS can be treated with resection of thymoma and intravenous immunoglobulin (IVIG).2 However, the resection of thymoma can relieve only some symptoms caused by space-occupying thymoma (chest pain, etc.) but cannot improve the abnormal immune function. Symptoms were aggravated after resection of thymoma in some GS patients.8, 22 IVIG can improve humoral immunodeficiency and is helpful in reducing respiratory infection (serum IgG level is recommended to be maintained at no lower than 5 g/L), but it cannot improve cellular immunodeficiency.6 Targeted antimicrobial prophylaxis and vaccination strategies can reduce the infectious complications of GS patients.23 GS has a poor prognosis with a mortality rate of about 45%–57%, and infection is the most common cause of death.2 The patient in this case had undergone resection of thymoma before diagnosis, but her IgG was 4.7 g/L (close to 5.0 g/L), and she did not receive IVIG for economic reasons.
Therefore, GS should be considered when recurrent pulmonary infections occur in adults with a history of thymoma.6 In addition, GS should also be considered in the case of centrilobular nodules with tree-in-bud changes on chest CT scan in patients with resection of thymoma.10 For patients with thymoma and recurrent pulmonary infection, high-resolution chest CT, determination of peripheral blood lymphocyte subsets, immunoglobulin determination and other immune function tests should be timely completed. In adults with DPB-like clinical manifestations, thymic lesions should be excluded and related immune function tests should be performed to exclude GS to avoid missed diagnosis and misdiagnosis.
AUTHOR CONTRIBUTIONTian Luo and Lile Wang contributed equally to this article. All authors have contributed substantially to the data acquisition and drafting of the manuscript, and have read and approved the final version.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
留言 (0)