
記住我

Pulmonary mucormycosis (PM) is a rare but often fatal fungal disease that is difficult to diagnose and treat. It often affects immunocompromised patients, with diabetes mellitus (DM), glucocorticoid use, haematological malignancies, haematopoietic stem cell transplantation and solid organ transplantation being the most common risk factors.1 The prevalence of PM is rising, with a recent outbreak associated with COVID-19, probably due to immune system dysregulation or widespread use of immunosuppressors.2 Rhizopus species in the order Mucorales cause most human infections. These fungal organisms are ubiquitous in nature. PM is caused by inhalation of spores, resulting in pneumonia and later necrosis and infarction of the lung tissue.3 The rate of recurrence of PM is high and has been reported in different literature.4-6 Here, we report a case of PM in a renal transplant recipient with poorly controlled DM, first diagnosed in 2012 and treated with antifungal for 1 year with radiological resolution. He was not prescribed secondary antifungal prophylaxis and the PM recurred in 2020 at the same site. To prevent recurrence, risk factors for PM, especially DM, should be controlled. Antifungal should be continued until complete response is demonstrated on imaging, and predisposing factors are permanently reversed.7
CASE REPORTA 51-year-old man presented in September 2020 with a 1-month history of cough, fever and frank haemoptysis.
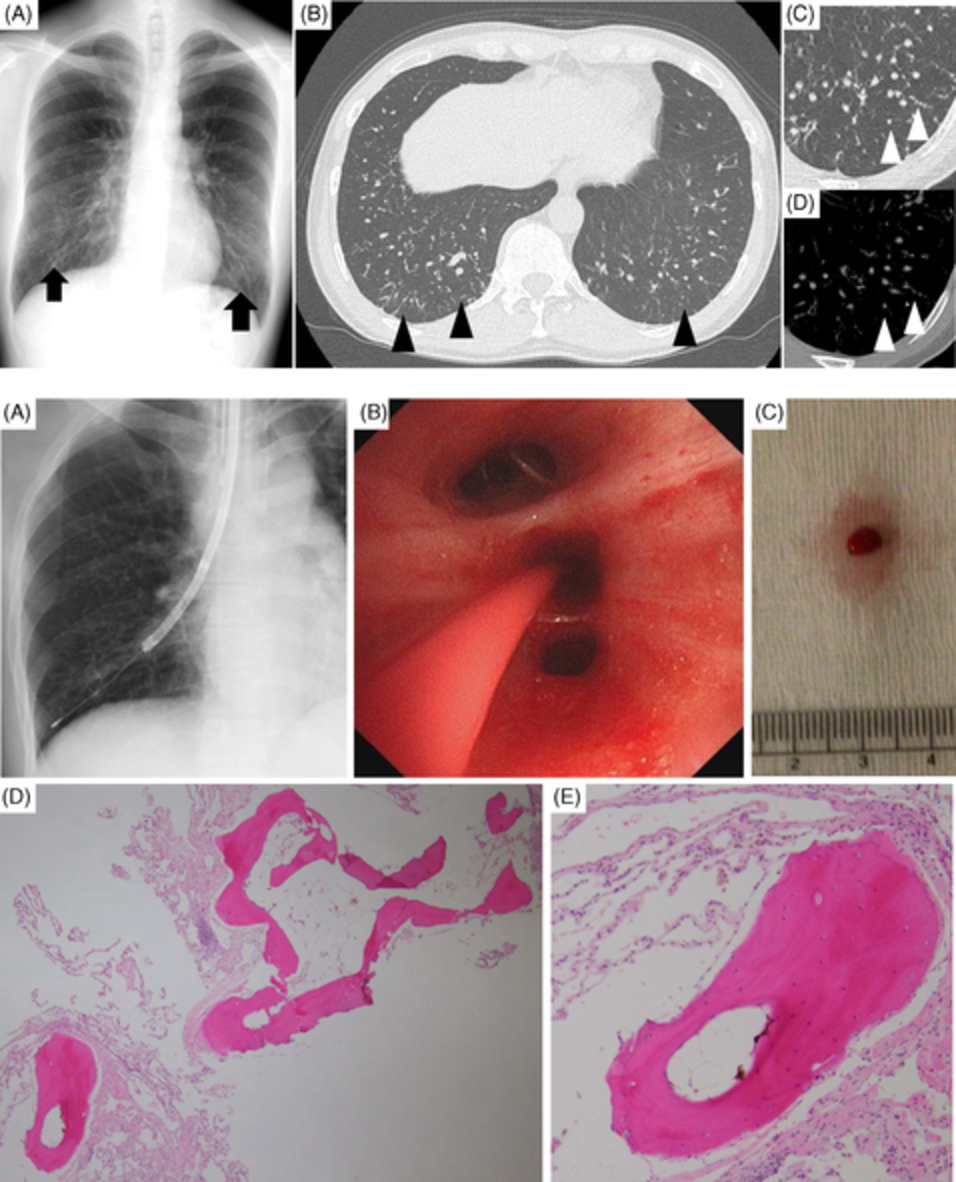
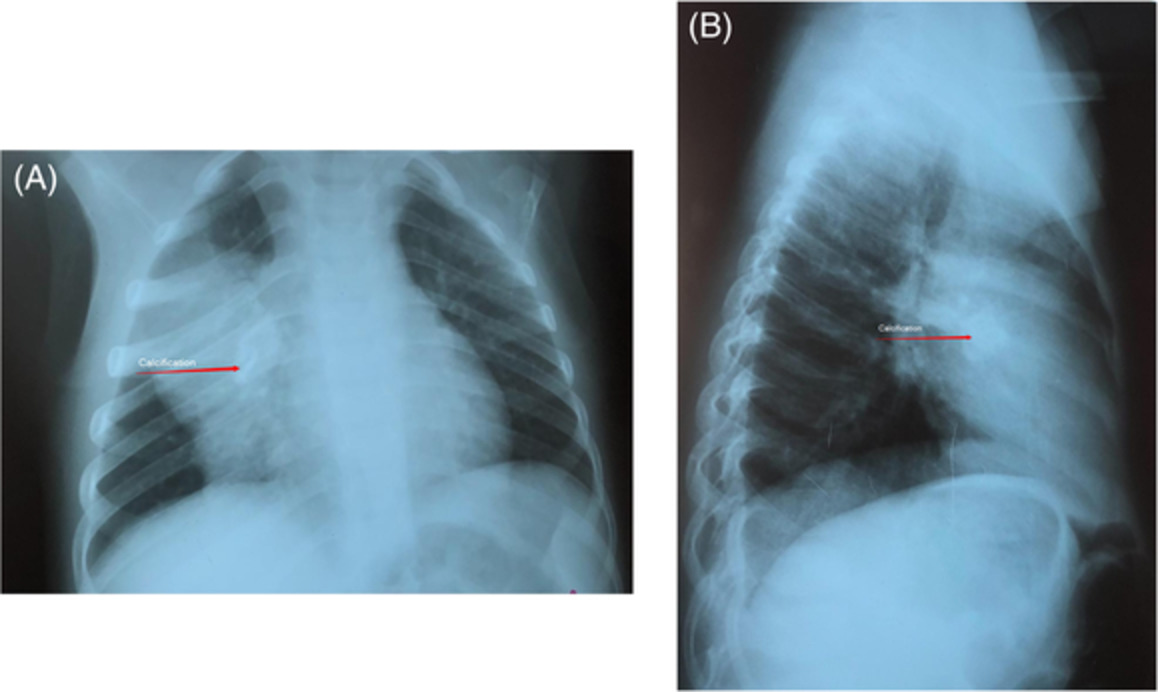
He had a past medical history of PM in March 2012. In 2012, computed tomography (CT) showed a 6-cm mass in the lingula (Figure 1A). Flexible bronchoscopy with transbronchial lung biopsy and bronchoalveolar aspirate was performed over the lingula (Figure 1B). Histopathological examination of the biopsy found fungal hyphae consistent with mucormycosis (Figure 1C) and the bronchial aspirate cultured Rhizopus species. He was treated with 6 weeks of intravenous (IV) amphotericin B liposome (5 mg/kg/day) followed by 48 weeks of oral posaconazole (300 mg twice daily) until complete radiological resolution of mycetoma on progress chest x-ray in January 2013 (Figure 1D). Surgical intervention was considered but no further follow-up action was taken.

Images taken in 2012–2013. (A) Computed tomography of the thorax showed a lingular cavitary lesion. (B) Bronchoscopy image identified abnormal discharge over the lingula. (C) Haematoxylin and eosin stained histopathology slide showed fungal material against an inflammatory background. (D) Chest x-ray with radiological resolution of pulmonary mucormycosis after treatment
His other past medical histories included chronic hepatitis B with liver cirrhosis, peripheral vascular disease, type 2 DM with nephropathy and cadaveric renal transplant in 2011. He was on several medications, including oral prednisolone 6 mg daily and tacrolimus prolonged release 1.5 mg daily. He was a lifelong non-smoker, worked as a security guard and had no known sick contact.
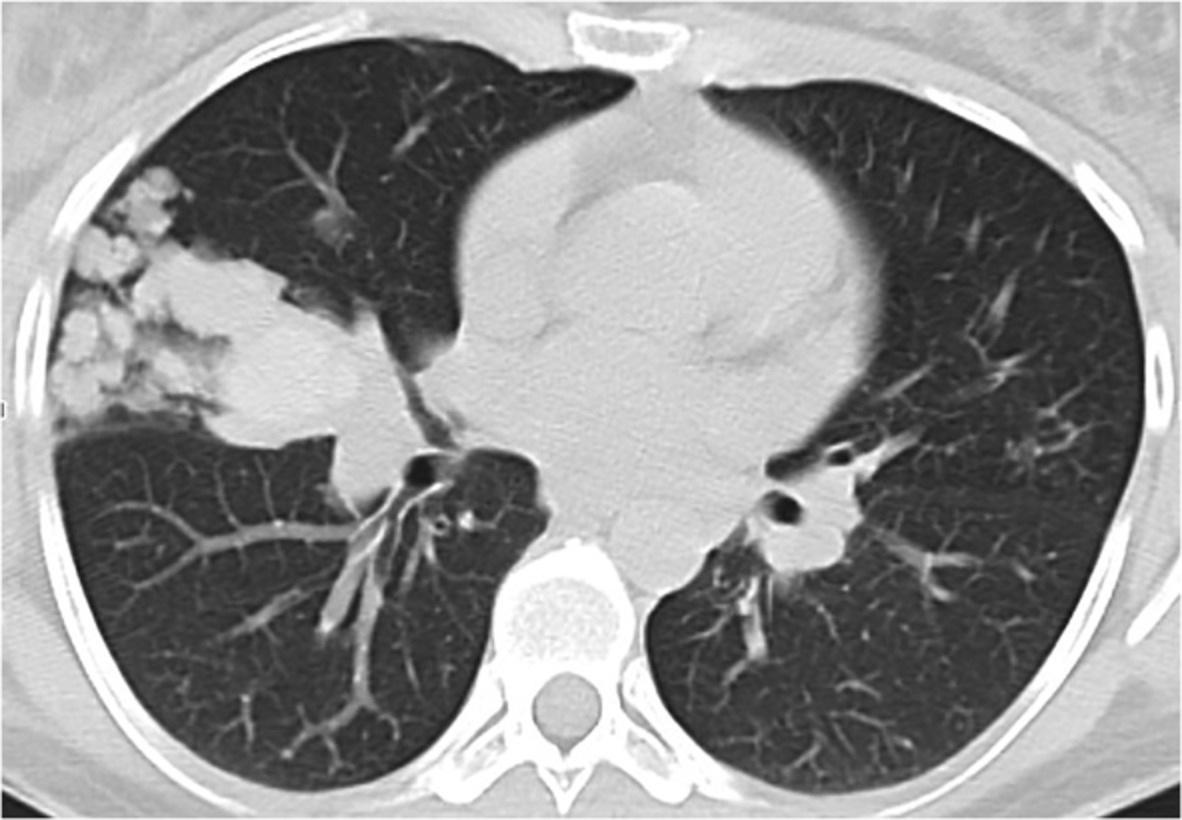
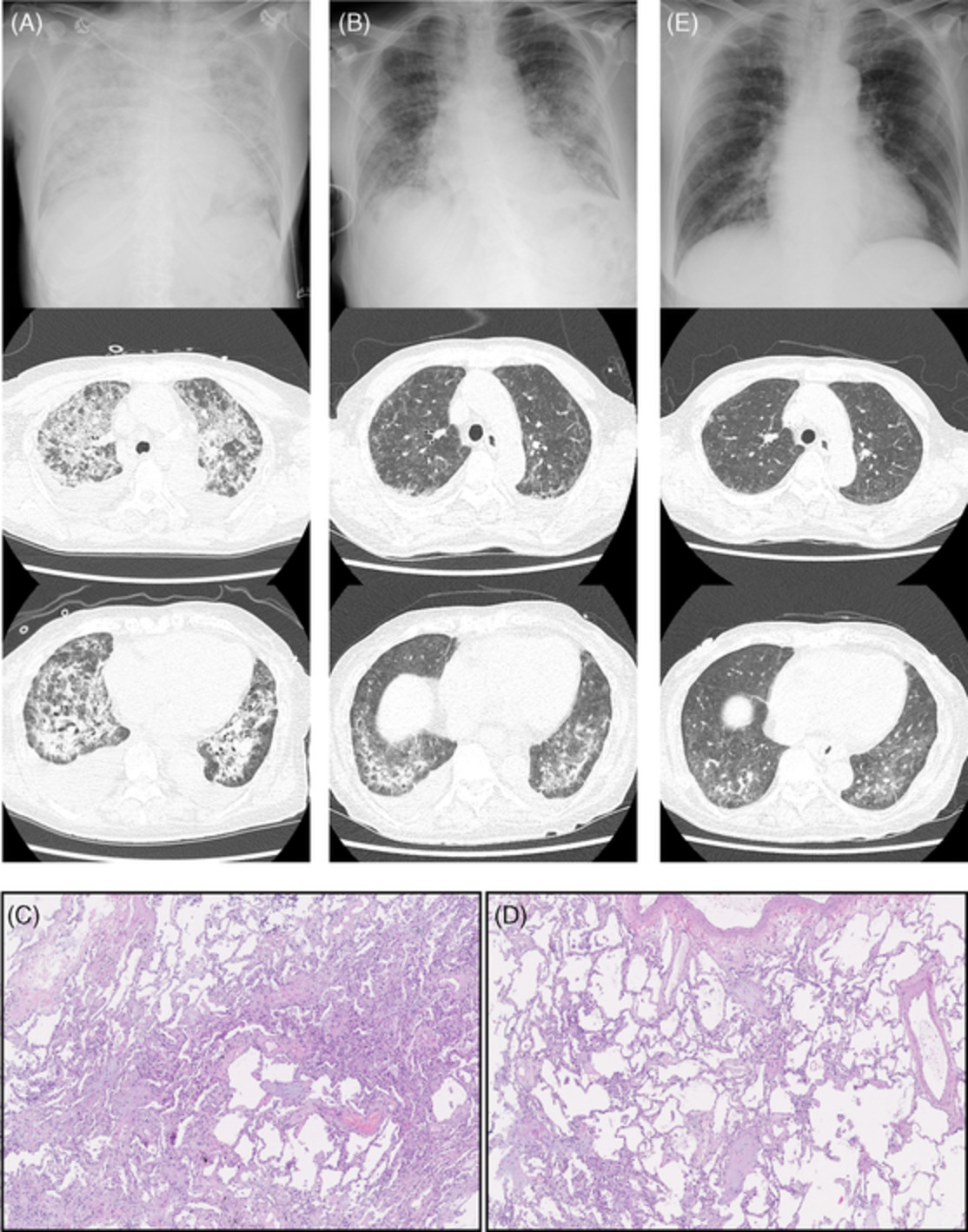
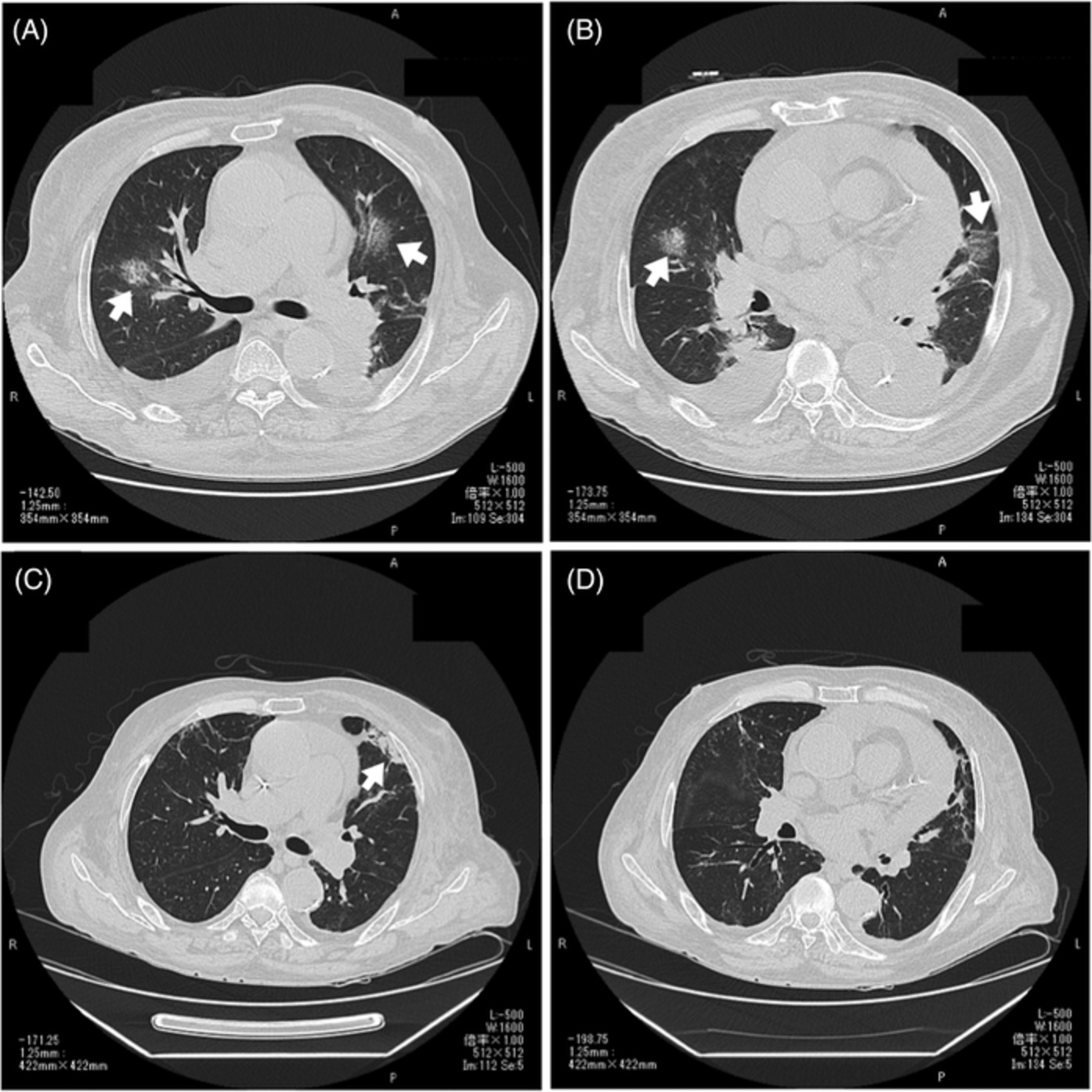
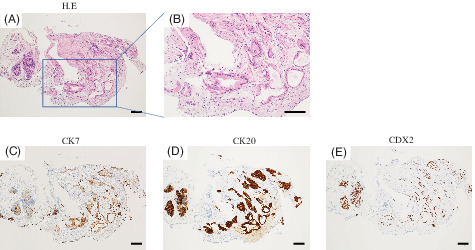
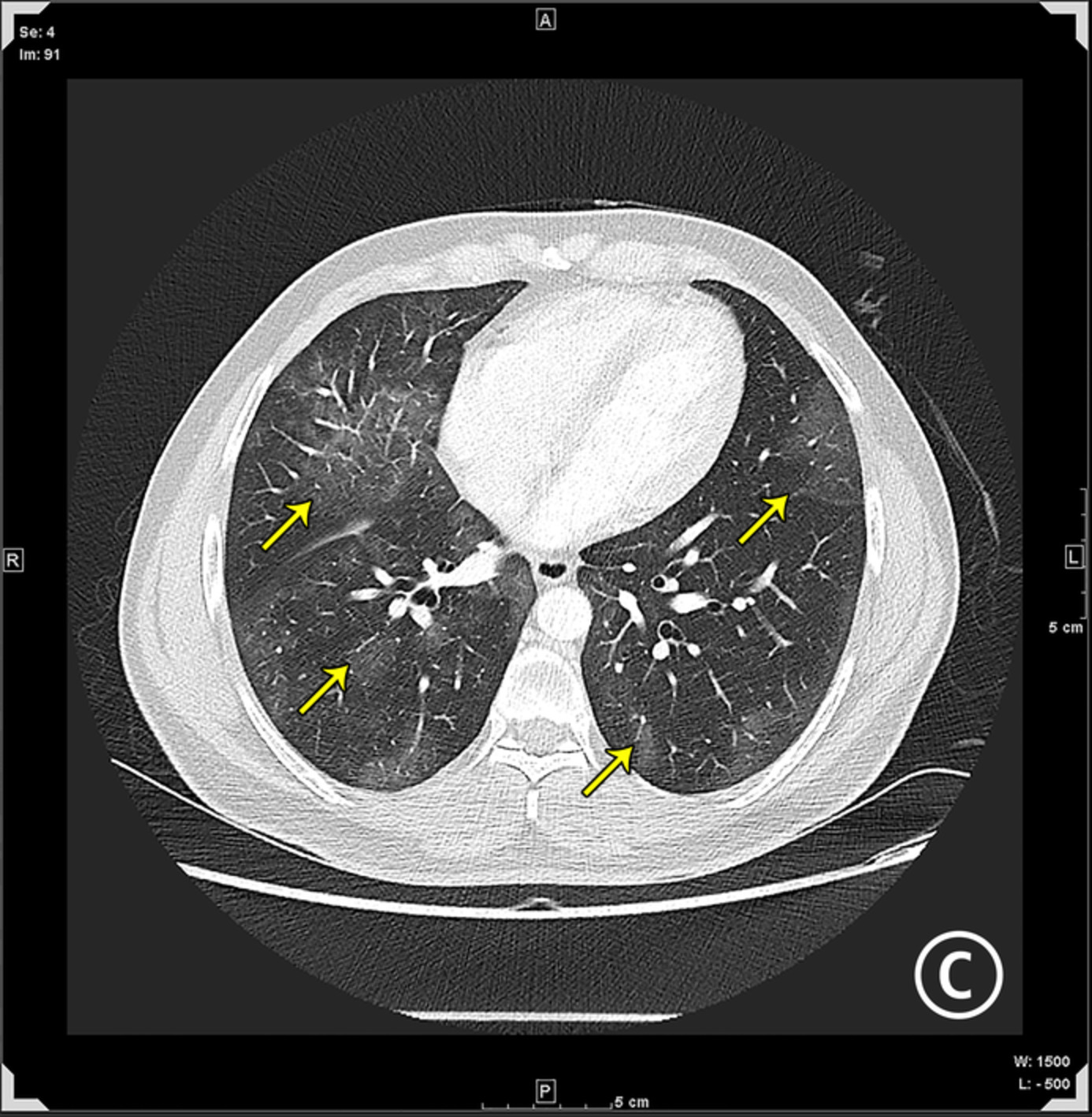
On the admission day in September 2020, chest examination of the patient revealed coarse crackles in the left middle zone. His sputum cultures, including Mycobacterium and fungal cultures, were negative. Procalcitonin was <0.05 ng/ml, white cell count 20.9 × 109/L, C-reactive protein 5.8 mg/L and HbA1c was 11.2%. Chest x-ray showed a left-sided homogenous opacity with surrounding consolidation. CT of the thorax with contrast showed a 1.7-cm cavitary lesion in the lingula, with lingular ground-glass opacity and left upper and left lower lobe infiltrate (Figure 2A). Flexible bronchoscopy identified a lesion in the superior lingular segment with spontaneous bleeding (Figure 2B). Multiple endobronchial biopsies of the mass were taken, and histopathological examination revealed fungus that are morphologically consistent with mucormycosis (Figure 2C). However, the fungal culture was negative for the specimen.

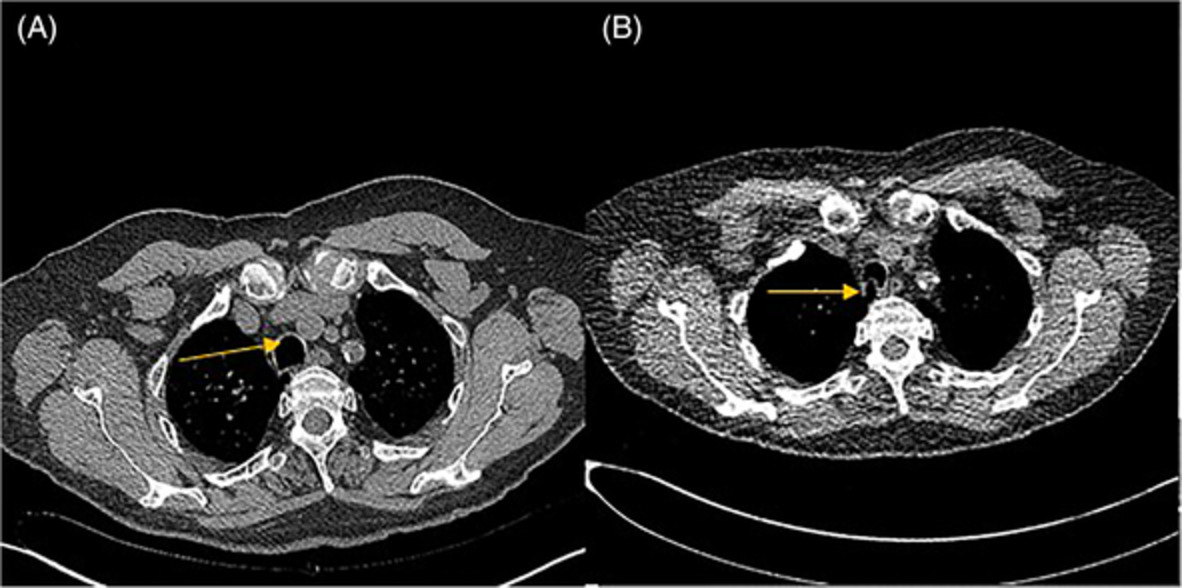
Images taken in 2020–2021. (A) Computed tomography of the thorax showed a cavitary lesion at the lingula. (B) Bronchoscopy image identified a lesion in the superior lingular segment. (C) Haematoxylin and eosin stained histopathology slides showed broad, non-septate fungal hyphae that branched irregularly at wide angles. (D) The latest chest x-ray in 2021 showed residual disease of pulmonary mucormycosis
The patient was diagnosed with recurrence of PM and received isavuconazole 200 mg daily, which was switched to IV amphotericin B liposome (5 mg/kg/day) due to worry about treatment resistance to the former antifungal. Cardiothoracic surgeons' opinions were sought but surgery was not performed eventually due to extremely high operational risk in view of the patient's multiple comorbidities. During his 3-month hospital stay, he was complicated by Chryseobacterium septicaemia, methicillin-sensitive Staphylococcus aureus septicaemia and amphotericin B liposome-induced acute kidney injury. Three months into treatment with IV amphotericin B liposome, repeat CT of the thorax showed interval enlargement of lingular mycetoma and the patient still complained of recurrent haemoptysis. Treatment failure was accepted by the patient, and he was discharged on non-curative treatment with oral isavuconazole 200 mg daily and nebulized amphotericin B 10 mg twice weekly. The latest chest x-ray taken 6 months after the diagnosis of PM recurrence showed a residual lingular cavitary lesion (Figure 2D).
DISCUSSIONMucormycosis is the second most common mould infection in immunocompromised patients.7 A multi-centred observational study in India found the most common predisposing factors for mucormycosis are diabetes (73.5%), malignancy (9%) and transplant (7.7%).8 For diagnosis, histopathological examination and fungal culture are strongly recommended. Histopathologically, the lesion is characterized by the presence of fungal hyphae, which under microscope, appears to be broad (5–15 μm in diameter), have rare or no septations and branch irregularly at wide angles.9 Fungal culture allows species identification but is falsely negative in up to half of the mucormycosis cases, as homogenization of the tissue may cause viability loss of the mucorales.10
Treatment of PM consists of a combination of surgery and antifungal. Procedures including lobectomy, pneumonectomy or wedge resection, whenever possible, are strongly recommended as they decrease mortality.7 IV amphotericin B liposome is the mostly used antifungal to treat PM, while isavuconazole or posaconazole may be used as salvage or step-down therapy. To prevent recurrence of mucormycosis, surgical resection and secondary prophylaxis with the last effective antifungal are strongly recommended in patients whose predisposing factors, such as solid organ transplant recipients, are irreversible.10
Recurrence of mucormycosis has been described in various case reports and the time interval between the first occurrence and recurrence ranges from 1 week to 2.5 years.4-6 Here, we have described a case of PM recurrence 8 years after its first occurrence, which is a much longer time interval in comparison with the available literature. Re-infection is a possibility, but recurrence is more likely as the PM occurred at the same anatomical site.
The reason for our patient's disease recurrence is likely multifactorial. First, surgery was not performed after the first PM diagnosis. Medical treatment alone often fails to treat mucormycosis. Second, the treatment duration of antifungal for the initial PM was suboptimal. The patient is a renal transplant recipient who receives lifelong immunosuppressants, which predisposes him to mucormycosis. According to international guidelines,7, 10 he should have received lifelong antifungal as secondary prophylaxis of mucormycosis. Third, his HbA1c was 11.2% meaning his DM was poorly controlled, which is also a risk factor for mucormycosis.
In conclusion, PM should be treated with a combination of antifungal and surgical resection. To prevent recurrence, risk factors for PM, especially DM, should be tightly controlled. Antifungal should be continued until complete response is demonstrated on imaging, and predisposing factors are permanently reversed.
ACKNOWLEDGMENTSThe authors would like to express their appreciation to Dr Chee Heng Cheryl Lung for providing and interpreting the histopathology slides. The authors also thank the patient who agreed to have his case published to raise awareness among medical staff for recurrence of PM.
CONFLICT OF INTERESTNone declared.
AUTHOR CONTRIBUTIONCheuk Cheung Derek Leung drafted the case report. Yu Hong Chan, Man Ying Ho and Ming Chiu Chan revised the case report critically for important intellectual content. Chun Hoi Chen and Chin Tong Kwok contributed to literature review. Yiu Cheong Yeung was involved in the final approval of the version to be published.
ETHICS STATEMENTAppropriate written informed consent was obtained for the publication of this case report and accompanying images.
REFERENCES
1Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis. 2005; 41: 634. 2Shakir M, Maan MHA, Waheed S. Mucormycosis in a patient with COVID-19 with uncontrolled diabetes. BMJ Case Rep. 2021 Jul 29; 14(7):e245343. 3Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. An unusual presentation of opportunistic mucormycosis. Br Med J (Clin Res Ed). 1981; 282: 108– 9. 4Panneerselvam K, Kumar MS, Karthikeyan, Mohan AM. Recurrent mucormycosis – better understanding of treatment and management. J Family Med Prim Care. 2020 Dec 31; 9(12): 6279– 81. 5Zhang L, Tian X, Wang P, Zhang H, Feng R. Recurrent pulmonary mucormycosis after lobectomy in a non-smoking patient without predisposing risk factors. Braz J Infect Dis. 2012 Nov–Dec; 16(6): 590– 3. 6Martin MS, Smith AA, Lobo M, Paramesh AS. Successful treatment of recurrent pulmonary mucormycosis in a renal transplant patient: a case report and literature review. Case Rep Transplant. 2017; 2017:1925070. 7Cornely OA, Arikan-Akdagli S, Dannaoui E, Groll AH, Lagrou K, Chakrabarti A, et al. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of mucormycosis 2013. Clin Microbiol Infect. 2014 Apr; 20(Suppl 3): 5– 26. 8Patel A, Kaur H, Xess I, Michael JS, Savio J, Rudramurthy S, et al. A multicentre observational study on the epidemiology, risk factors, management and outcomes of mucormycosis in India. Clin Microbiol Infect. 2020 Jul; 26(7): 944.e9– 944.e15. 9Frater JL, Hall GS, Procop GW. Histologic features of zygomycosis: emphasis on perineural invasion and fungal morphology. Arch Pathol Lab Med. 2001 Mar; 125(3): 375– 8. 10Cornely OA, Alastruey-Izquierdo A, Arenz D, Chen SCA, Dannaoui E, Hochhegger B, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019 Dec; 19(12): e405– 21.
留言 (0)