
記住我

Pulmonary pleomorphic carcinoma (PPC) is a rare type of non-small cell lung cancer (NSCLC) with a more aggressive clinical course and a worse outcome than other types of NSCLC.1, 2 PPC is the most common (>50%) type of pulmonary sarcomatoid carcinoma, which consists of spindle cell carcinoma, giant cell carcinoma, pulmonary blastoma and carcinosarcoma.3 PPC is common in elderly male smokers.4 Despite diagnosis and resection of early-stage disease, the risk of PPC relapse and aggressive clinical course is high.5 However, there is no consensus regarding the chemotherapy regimen for advanced pulmonary carcinoma.
Pembrolizumab, a monoclonal antibody targeting programmed cell death-1 (PD-1), has been approved as the first-line treatment for advanced NSCLC with strongly expressed PD-1 in at least 50% of tumour cells, without epidermal growth factor receptor gene (EGFR) mutations or anaplastic lymphoma kinase gene (ALK) rearrangement.6 However, little is known concerning the efficacy of anti-PD-1 therapy for PPCs.
Here, we describe a patient with PPC characterized by robust PD-L1 expression who showed a good response to pembrolizumab and sequential radiotherapy.
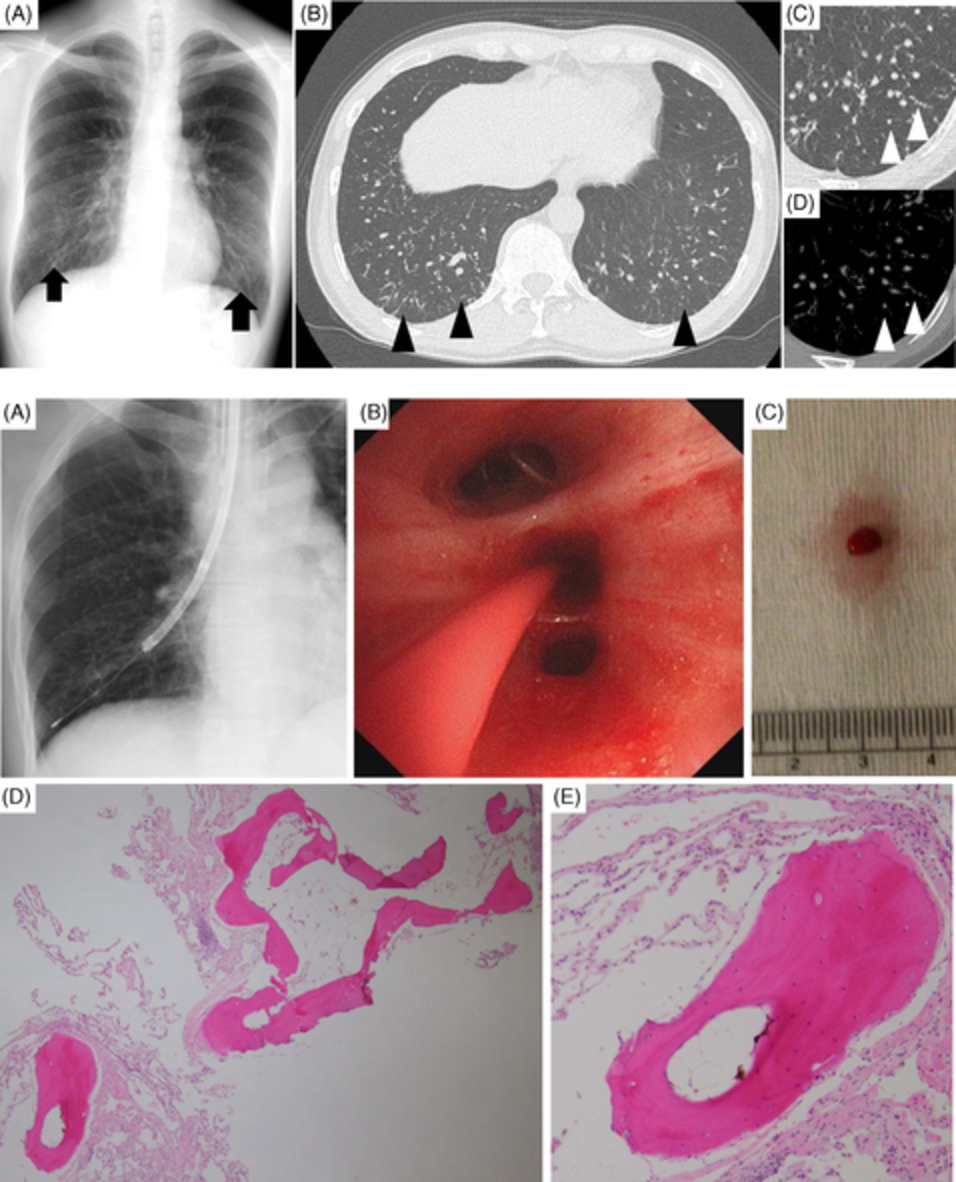
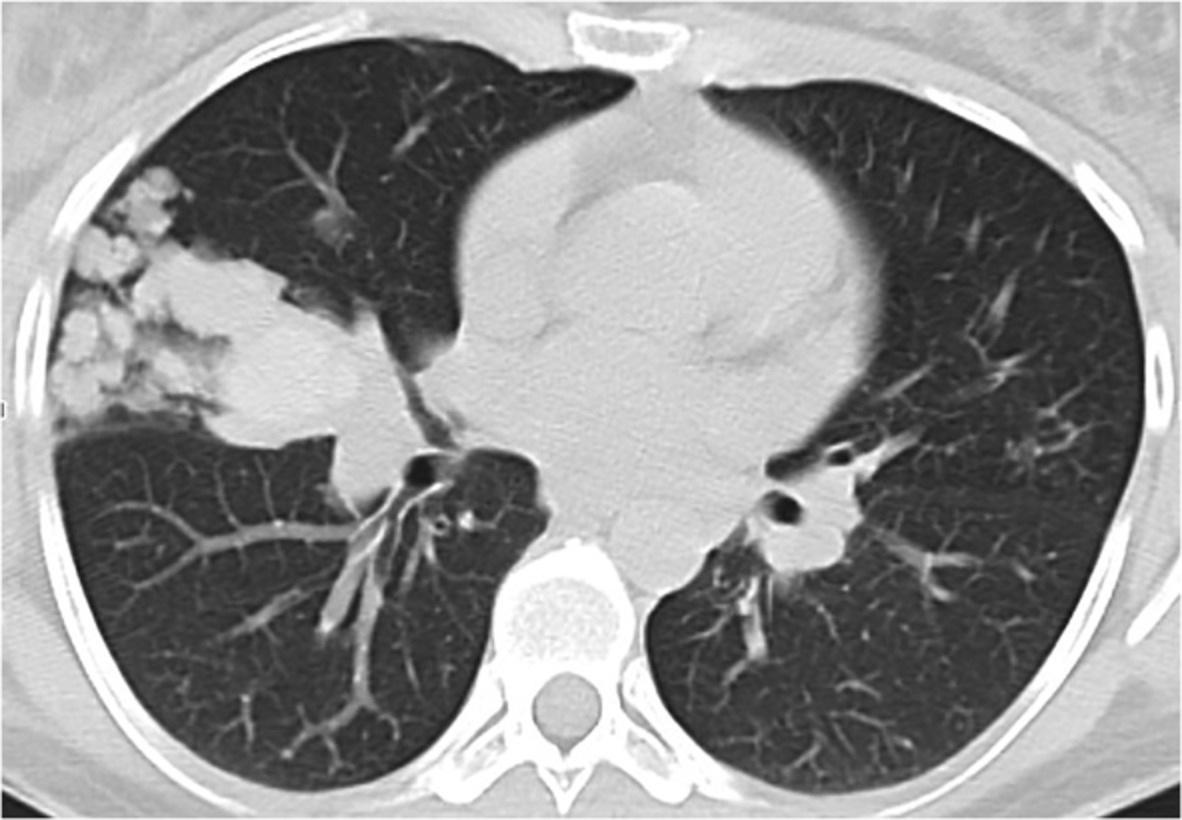
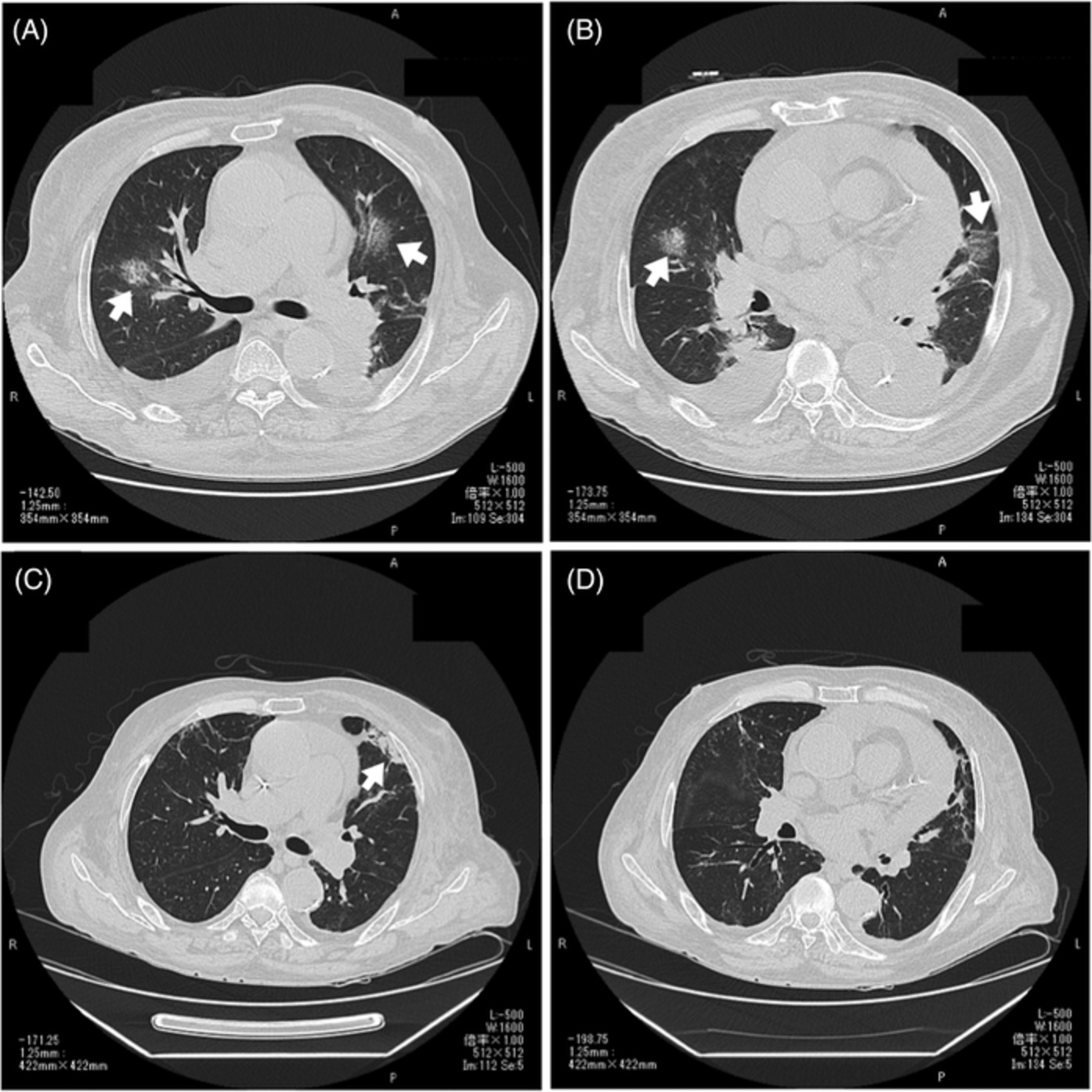
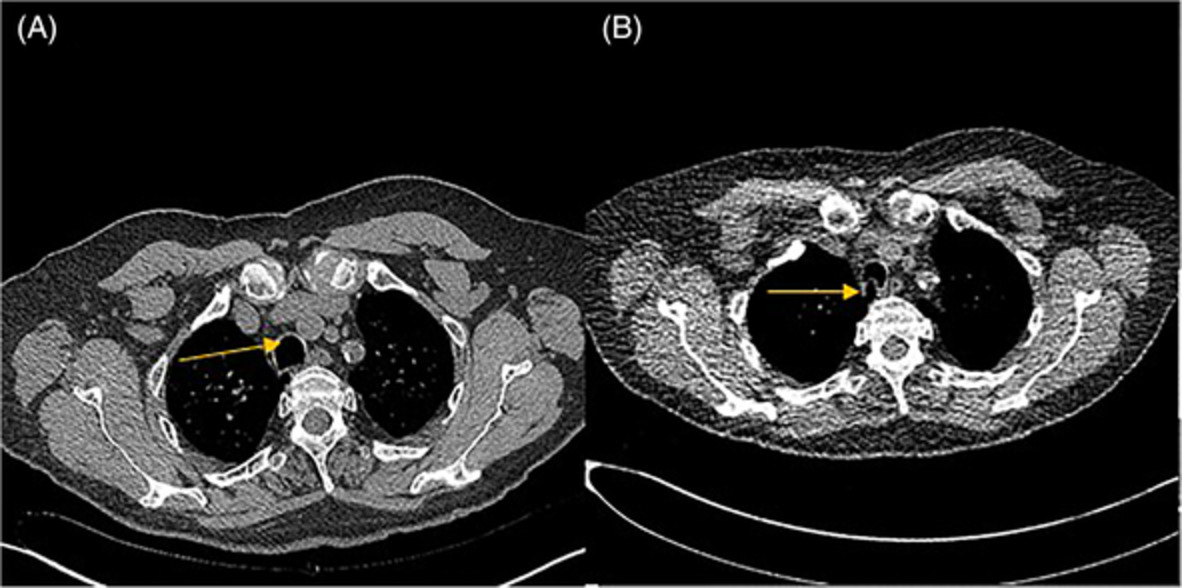
CASE REPORTAn 80-year-old man who smoked (one pack per day for 60 years) visited the emergency room because of haemoptysis in late January 2020. He had a history of diabetes, hypertension, atrial fibrillation and stable angina; he had taken oral hypoglycaemic agent and insulin, anti-hypertensive medicine, amiodarone and anticoagulant (apixaban). He had undergone cholecystectomy in early January 2020. His performance status was European Cooperative Oncology Group (ECOG) 3. Chest computed tomography (CT) scan taken when he was admitted for surgery showed a small nodule (Figure 1A). A chest CT scan taken when he visited the emergency room showed a lung nodule (approximately 3 cm) in the left upper lobe (LUL) (Figure 1B). We regarded it as a haematoma because of its rapid growth rate and poor contrast enhancement. As he was a current heavy smoker and had a haemoptysis, he was hospitalized and anticoagulant was stopped. Bronchoscopy showed no evidence of endobronchial lesion and symptom was improved after stopping anticoagulant. We recommended that the patient undergo a biopsy of lung nodule; however, he was reluctant to invasive procedures and we decided to perform follow-up chest CT scan. However, we found that the mass in the left lingular segment increased from 3 to 6 cm within 1 month (Figure 1C). Because of the rapid growth, the patient underwent [18F]fluorodeoxyglucose (FDG) positron emission tomography (PET)-CT. The scan showed a high level of [18F]FDG uptake in the LUL mass (Figure 2A).

Chest computed tomography (CT) scan taken a month before presenting haemoptysis reveals a tumour of 13 mm in diameter in the left lung (A). Chest CT scan taken after visiting emergency department with haemoptysis shows about a 30-mm-sized lung nodule (B). It is observed that the diameter of the left lung nodule nearly doubled, showing a rapid growth rate (C). The tumour size was 80 mm at the time of first cycle of pembrolizumab treatment (D)

[18F]fluorodeoxyglucose-positron emission tomography (FDG-PET) scan shows a huge hypermetabolic mass in the left mid-thorax near hilar region [maximum standardized uptake value (SUV max): 26.5, 69 mm in diameter] with invasion of mediastinal pleura (A). FDG-PET scan taken after radiotherapy shows a markedly decreased size and metabolism (SUV max: 1.67, 24 mm in diameter) of previous hypermetabolic mass lesion in the left upper lobe (LUL), thyroid transcription factor-1 (TTF-1) of the lung (B). FDG-PET scan taken 13 months after the end of treatment shows a decreased size and metabolism of a hypermetabolic fibrotic lesion at the LUL (C)
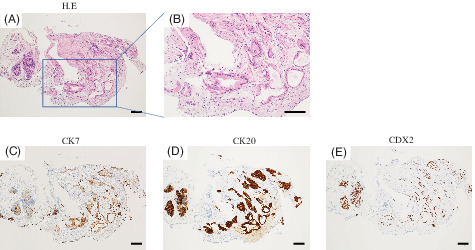
Endobronchial ultrasound-guided biopsy of the lung nodule was performed for diagnosis, and the histological examination revealed pleomorphic carcinoma (Figure 3A,B). Immunohistochemistry showed that the primary tissue did not express P40. Staining for TTF-1 was negative; pan- cytokeratins (CK) staining results were positive. The tumour did not exhibit EGFR mutations or ALK rearrangement. Immunohistochemistry also detected PD-L1 (22C3, SP263) expression in 100% of tumour cells (Figure 3C,D).

Histological examination of a tumour biopsy specimen by haematoxylin–eosin staining reveals undifferentiated polymorphic malignant cells (A, ×200). The tumour cells show highly atypical, with distinct nucleoli, heterogeneous or bizarre megakaryocytes and polynuclei (B, ×500). Immunohistochemical analysis showed that the tumour cells strongly expressed PD-L1 (C, ×200, tumour proportion score 100% for 22C3; D, ×200, tumour proportion score 100% for SP263)
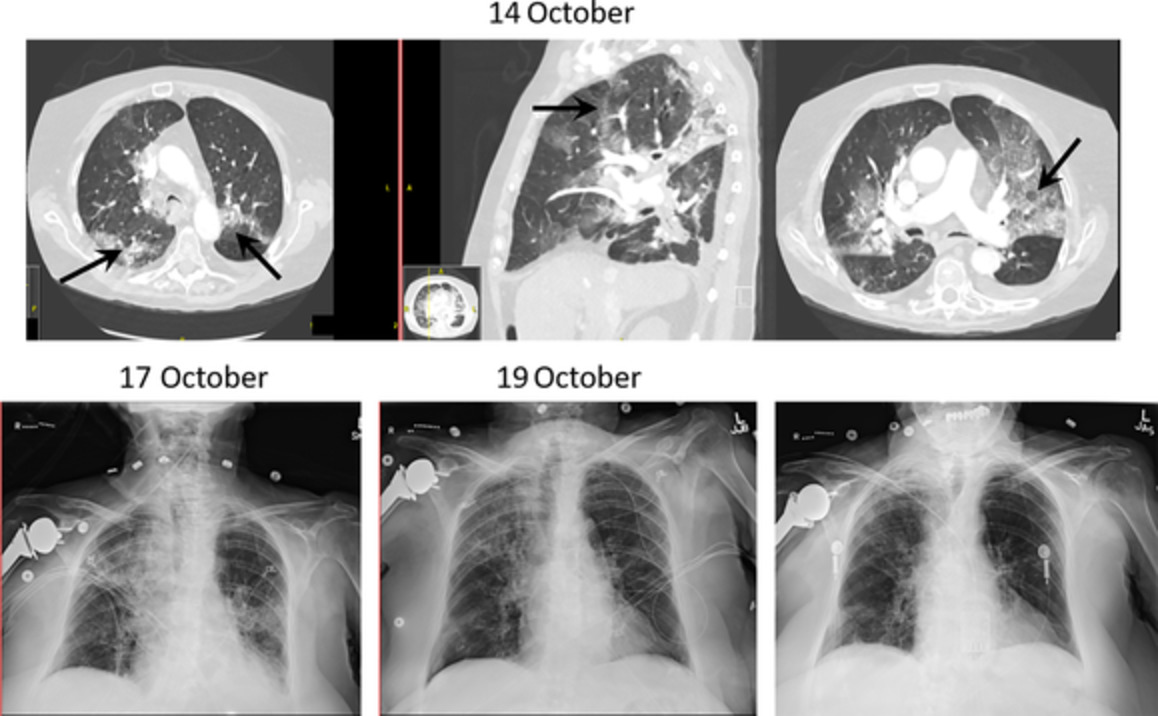
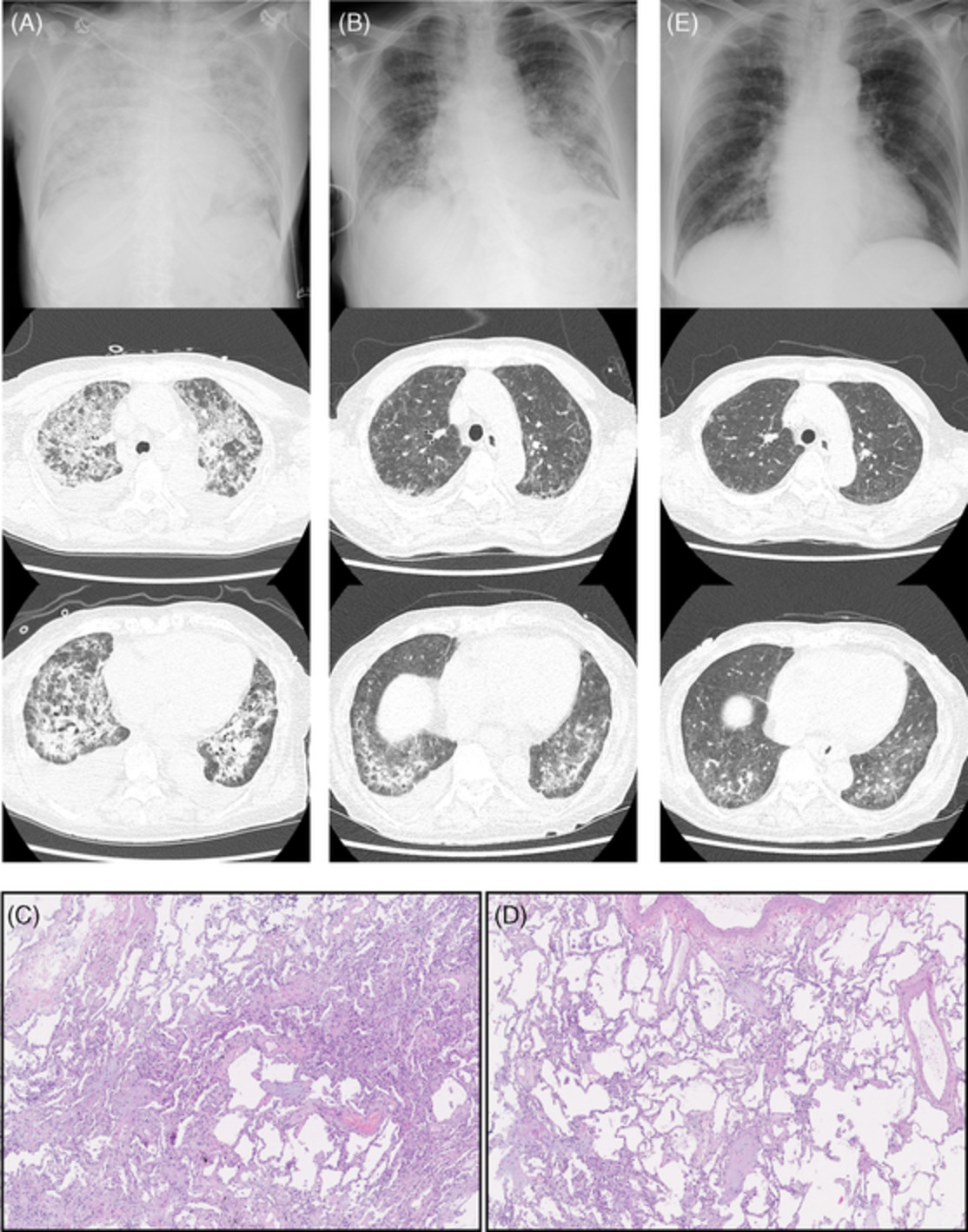
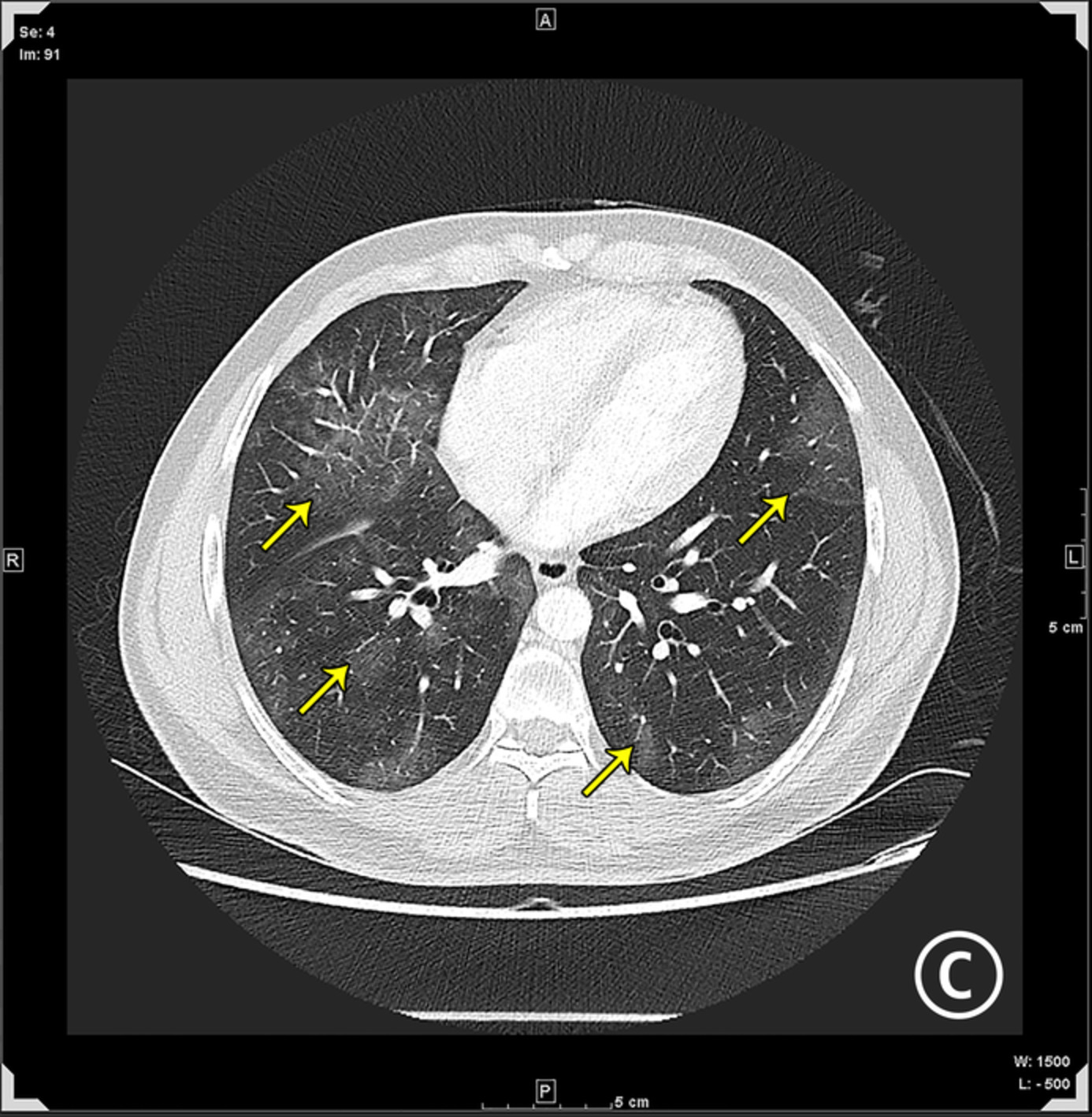
Chest CT scan taken after tissue diagnosis showed the tumour was increased to 8.1 cm with encasement of left atrial appendage within 3 weeks (Figure 1D). The clinical stage was classified as stage IIIA (cT4N0M0). Considering the patient's age, comorbidities and performance status, pembrolizumab was administered at a dose of 200 mg every 3 weeks rather than surgery or cytotoxic chemotherapy. After four cycles of pembrolizumab treatment, CT revealed marked shrinkage of the left lung nodule (Figure 4A) and PET-CT showed a marked decrease in [18F]FDG uptake in primary mass (Figure 2B). Subsequently, the tumour was treated with intensity-modulated radiation therapy (IMRT) of 6000 cGy. Two months after IMRT completion, the tumour had decreased to 1.8 cm in diameter and it remains stable disease after 6 months (Figure 4C). PET-CT scan taken 13 months after radiation therapy showed decreased size and metabolism of a hypermetabolic fibrotic lesion at the LUL (Figure 2C). Although the patient with locally advanced stage was elderly and had multiple comorbidities such as atrial fibrillation, diabetes, stable angina and stroke, he completed the treatment without adverse side effects. After four cycles of pembrolizumab therapy and IMRT, the disease has been well controlled without additional treatment for 15 months, until now.

Chest computed tomography (CT) scan taken after the third cycle of the pembrolizumab therapy revealed shrinkage of the primary lesion (A). Chest CT scan (2 months after the radiotherapy) reveals a pronounce decrease in the diameter of lung nodule in the left upper lung with pericardial effusion (B). Chest CT scan shows a stable disease at about 1 year after diagnosis (C)
DISCUSSIONHere, we report a case of PPC with robust expression of PD-L1 (SP263, 22C3), which was treated with four cycles of pembrolizumab followed by IMRT. In this case, we performed successful treatment with pembrolizumab and sequential IMRT without complications in an older patient who had clinically inoperable status because of multiple comorbidities and locally advanced disease. PPC is a condition with a poor prognosis, that is, the 5-year survival rate was approximately 11%–21%,7 and without clear standard treatment; therefore, we explored the role of combined pembrolizumab and radiotherapy in PPC through our case report and a literature review.
The incidence of PPC has been reported to range from 0.1% to 0.4% of all lung cancers; only a few case reports have been published. Because of its rarity, clinical trials have been limited and no standard treatment has been established. Usually, surgery is the first choice during the early stage of the disease and the role of chemotherapy remains unclear.8-11 Advanced PPC has shown poor response to palliative chemotherapy regimens.8, 12 EGFR mutations are recognized in approximately 20% of PPCs and some patients with EGFR mutations have shown responses to erlotinib or gefitinib.13, 14
It has been recently reported that the expression of PD-L1 is relatively high in PPCs.15 In addition, several reports indicated that anti-PD-1/PD-L1 treatment was effective for PPCs with robust expression of PD-L1.16-19 The cases so far reported that anti-PD/PD-L1 treatment prolonged the progression-free duration by maintaining immune checkpoint inhibitors in patients who respond well to the treatment; 16 cycles of pembrolizumab therapy and more than 10 cycles of nivolumab therapy continuously.17, 20 However, the combination treatment of four cycles of pembrolizumab and IMRT was effective in this case. There have been several case reports concerning the positive effects of combining immune checkpoint inhibitors and radiotherapy after surgical treatment of PPCs.21, 22 Based on these studies, we attempted pembrolizumab followed by radiation therapy as the first-line treatment in a patient with locally advanced clinical stage with inoperable medical condition, which resulted in a favourable response. There may be economic limitations in the use of anti-PD-1/PD-L1 therapy in various medical and social environment. After reducing the tumour burden with several cycles of immune checkpoint inhibitors, in patients with PPC with expression of PD-L1, addition of radiation therapy can be an option for local tumour control instead of continuing immune checkpoint inhibitors.
This case shows that the combination of immune checkpoint inhibitor and radiation therapy is an option for effective treatment of highly aggressive PPCs. In addition, this case reinforces the importance of measuring PD-L1 expression on tumour cells to provide optimal anti-PD-1 therapy in patients with PPC. Although PPCs are rare, there is a need to determine the efficacy of combination treatment comprising anti-PD-1 therapy and radiotherapy for PPC through clinical trials. We report this case to demonstrate the effectiveness of combined immunotherapy and radiotherapy in the treatment of locally advanced stage of PPCs.
CONFLICT OF INTERESTNone declared.
AUTHOR CONTRIBUTIONTae-Hun Kim and Sun Hyo Park contributed equally to this work. Tae-Hun Kim, Sun Hyo Park, Ilseon Hwang, Jin Hee Kim and Hyun Jung Kim contributed to the drafting of the manuscript, data analysis and draft revision. Jin Hee Lee and Hae Won Kim contributed to draft revision and image analysis, and all authors approved the final draft for publication.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
REFERENCES
1Chang YL, Lee YC, Shih JY, Wu CT. Pulmonary pleomorphic (spindle) cell carcinoma: peculiar clinicopathologic manifestations different from ordinary non-small cell carcinoma. Lung Cancer. 2001; 34(1): 91– 7. 2Mochizuki T, Ishii G, Nagai K, Yoshida J, Nishimura M, Mizuno T, et al. Pleomorphic carcinoma of the lung: clinicopathologic characteristics of 70 cases. Am J Surg Pathol. 2008; 32(11): 1727– 35. 3Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol. 2015; 10(9): 1243– 60. 4Baldovini C, Rossi G, Ciarrocchi A. Approaches to tumor classification in pulmonary sarcomatoid carcinoma. Lung Cancer (Auckl). 2019; 10: 131– 49. 5Yuki T, Sakuma T, Ohbayashi C, Yoshimura M, Tsubota N, Okita Y, et al. Pleomorphic carcinoma of the lung: a surgical outcome. J Thorac Cardiovasc Surg. 2007; 134(2): 399– 404. 6Pai-Scherf L, Blumenthal GM, Li H, Subramaniam S, Mishra-Kalyani PS, He K, et al. FDA approval summary: pembrolizumab for treatment of metastatic non-small cell lung cancer: first-line therapy and beyond. Oncologist. 2017; 22(11): 1392– 9. 7Lin Y, Yang H, Cai Q, Wang D, Rao H, Lin S, et al. Characteristics and prognostic analysis of 69 patients with pulmonary sarcomatoid carcinoma. Am J Clin Oncol. 2016; 39(3): 215– 22. 8Bae HM, Min HS, Lee SH, Kim DW, Chung DH, Lee JS, et al. Palliative chemotherapy for pulmonary pleomorphic carcinoma. Lung Cancer. 2007; 58(1): 112– 5. 9Hong JY, Choi MK, Uhm JE, Park MJ, Lee J, Park YH, et al. The role of palliative chemotherapy for advanced pulmonary pleomorphic carcinoma. Med Oncol. 2009; 26(3): 287– 91. 10Kato D, Chihara Y, Shirase T, Takahashi T, Takahashi KI, Sakai N. Successful treatment of two consecutive cases of pulmonary pleomorphic carcinoma with platinum chemotherapy. Oncol Lett. 2015; 10(5): 3040– 2. 11Takeda K, Matsushita H, Kubozono M, Tanabe T, Ishikawa Y, Yamamoto T, et al. Definitive chemoradiotherapy for advanced pulmonary sarcomatoid carcinoma. Intern Med. 2016; 55(22): 3325– 30. 12Oda T, Sekine A, Kato T, Baba T, Okudela K, Ogura T. Promising effect of chemotherapy with bevacizumab for patients with pulmonary pleomorphic carcinoma: two case reports and a literature review. Respir Investig. 2015; 53(6): 296– 9. 13Kaira K, Horie Y, Ayabe E, Murakami H, Takahashi T, Tsuya A, et al. Pulmonary pleomorphic carcinoma: a clinicopathological study including EGFR mutation analysis. J Thorac Oncol. 2010; 5(4): 460– 5. 14Tamura Y, Fujiwara Y, Yamamoto N, Nokihara H, Horinouchi H, Kanda S, et al. Retrospective analysis of the efficacy of chemotherapy and molecular targeted therapy for advanced pulmonary pleomorphic carcinoma. BMC Res Notes. 2015; 8: 800. 15Kim S, Kim MY, Koh J, Go H, Lee DS, Jeon YK, et al. Programmed death-1 ligand 1 and 2 are highly expressed in pleomorphic carcinomas of the lung: comparison of sarcomatous and carcinomatous areas. Eur J Cancer. 2015; 51(17): 2698– 707. 16Ikematsu Y, Yoneshima Y, Ijichi K, Tanaka K, Harada T, Oda Y, et al. Marked response to pembrolizumab in a patient with pulmonary pleomorphic carcinoma highly positive for PD-L1. Lung Cancer. 2017; 112: 230– 1. 17Kanazu M, Uenami T, Yano Y, Nakatsubo S, Hosono Y, Ishijima M, et al. Case series of pleomorphic carcinomas of the lung treated with nivolumab. Thorac Cancer. 2017; 8(6): 724– 8. 18Matsumoto Y, Miura T, Horiuchi H, Usui K. The successful treatment of pulmonary pleomorphic carcinoma with pembrolizumab: a case report. Case Rep Oncol. 2017; 10(2): 752– 7. 19Lee J, Choi Y, Jung HA, Lee SH, Ahn JS, Ahn MJ, et al. Outstanding clinical efficacy of PD-1/PD-L1 inhibitors for pulmonary pleomorphic carcinoma. Eur J Cancer. 2020; 132: 150– 8. 20Chang HC, Hsu CL, Chang YL, Yu CJ. Pulmonary pleomorphic carcinoma with pembrolizumab monotherapy. Respirol Case Rep. 2020; 8(6):e0597. 21Yorozuya T, Taya T, Yasuda K, Nagano Y, Shioya M, Chiba H, et al. Long-term response with durvalumab after chemoradiotherapy for pulmonary pleomorphic carcinoma: a case report. Thorac Cancer. 2020; 11(4): 1090– 3. 22Yaguchi D, Ichikawa M, Ito M, Okamoto S, Kimura H, Watanabe K. Dramatic response to nivolumab after local radiotherapy in pulmonary pleomorphic carcinoma with rapid progressive post-surgical recurrence. Thorac Cancer. 2019; 10(5): 1263– 6.
留言 (0)