
記住我

Immune checkpoint-inhibitors (CPIs) were first approved by the U.S. Food and Drug Administration in 2011 as second-line therapy for different types of carcinoma, especially melanoma and lung cancer, in adults.1, 2 Meanwhile, CPIs entered first-line therapy and are increasingly considered as adjuvant cancer therapy. CPIs block inhibitory signals of T cells thereby activating antitumor immunity.3, 4
Releasing the brakes of the immune system by blocking negative immune checkpoints may lead to various immune-related adverse events and diseases.5-7 Endocrinopathies were reported in 4%-30% of patients under CPI therapy independent of the CPI that was used.8 Among the most common immune-related adverse events are colitis, hepatitis, and hypothyroidism; more rarely adrenal failure and autoimmune diabetes.3, 6, 7
CPI-induced diabetes mellitus (CPI-DM) has most frequently been reported with anti-PD-1 or anti-PD-L1 therapy whereas DM due to anti-CTLA-4 therapy is very rare.9 Ikegami et al suggested a necessary preexisting susceptibility for type 1 diabetes (T1DM) to develop CPI-DM in PD-1 deficient patients.3 The incidence of CPI-DM among CPI users varies between 0.2%-1%.1, 3, 5, 8 CPI-DM develops often within 3 months of CPI therapy initiation10 but was also reported to vary between 2 weeks and over a year,8 and even months after discontinuation of CPI therapy5 or after a single administration.11
Interestingly, CPI-DM can develop as new onset diabetes or in patients with a history of type 2 diabetes (T2DM).12 Reviewing recent literature on the subject, authors seem to agree on CPI-DM belonging to T1DM due to immune-mediation, which is also the current classification of the German Diabetes Association.13 However, one can also argue that CPI-DM belongs - similar to glucocorticoid-induced diabetes - to the group of medication-induced diabetes (MI-DM).14
Therefore, we aimed to compare classic T1DM, MI-DM, and T2DM with CPI-DM using a large multicenter registry, which - to the best of our knowledge - has not been done in a large dataset so far.
2 METHODSIn this study, we included patients documented in the Diabetes Patient Follow-Up registry (DPV) that fulfilled the following criteria: (a) treatment data available between 2011 and 2020; (b) age at diagnosis ≥18 years; (c) CPI-DM, classic autoimmune T1DM with documented insulin treatment, T2DM, or MI-DM; and (d) no change in diabetes type due to initial misclassification.
The DPV comprises 603 554 patients with different diabetes types from 504 centers in Germany, Austria, Switzerland, and Luxembourg (January 2021).15 Of these, patients from 162 centers from Germany and Austria fulfilled the inclusion criteria and were included in the study. The registry was conducted in accordance with Good Epidemiology Practice and applicable regulatory requirements. The protocol of DPV was approved by the ethics committee of Ulm University (approval no. 202/09), and data collection was approved by local review boards at the participating centers.
Demographic data include age, sex, and diabetes duration. Outcomes are body mass index (BMI) in kg/m2, HbA1c, type of diabetes therapy (insulin pump, insulin only, oral antidiabetics [OADs] only, insulin + OADs, lifestyle modification only), daily insulin dose per kg bodyweight, diabetic ketoacidosis (DKA), and concomitant diseases including autoimmune thyroid disease (clinical diagnosis), autoimmune adrenal insufficiency (clinical diagnosis and/or adrenal antibodies plus hydrocortisone substitution), and autoimmune hepatitis (clinical diagnosis). HbA1c was standardized to the Diabetes Control and Complication Trial reference range of 4.05%-6.05% using the multiple of the mean method.16 DKA was defined via pH < 7.3 and/or serum bicarbonate <15 mmol/mol. Missing pH and bicarbonate was assumed to be within the reference range.17 Data were aggregated from repeated measurements during the patients' first documented treatment year. HbA1c and DKA were separately aggregated for manifestation (DKA: 10 days, HbA1c: 30 days around diagnosis) and for the follow-up period (first documented treatment year without the manifestation interval).
Continuous outcomes were presented as medians with interquartile range, dichotomous outcomes as percentage. Outcomes that were available only in <5 patients were not reported because of data protection. We performed separate propensity score matching procedures for CPI-DM and T1DM/T2DM/MI-DM respectively using the variables age, sex, and diabetes duration owing to significant differences between the groups and the rarity of CPI-DM. With a greedy k:1 matching, we found 29 T1DM, 24 000 T2DM, and 120 MI-DM patients with standard caliper width less than 0.2. We maximized k for each group-wise matching procedure to receive comparison groups that were as large as possible. We calculated standardized differences for the unmatched and matched cohort. Standardized differences of <10% after propensity score matching were treated as negligible.15 Then, the groups were compared via Wilcoxon's rank-sum test for continuous outcomes and  -test for dichotomous outcomes with CPI-DM patients representing the reference group. Two-sided P values (significance set < 0.05) were adjusted for multiple testing using the Bonferroni stepdown method. Statistical analysis was carried out using SAS 9.4 for Windows (SAS Institute, Cary, NC, USA).
-test for dichotomous outcomes with CPI-DM patients representing the reference group. Two-sided P values (significance set < 0.05) were adjusted for multiple testing using the Bonferroni stepdown method. Statistical analysis was carried out using SAS 9.4 for Windows (SAS Institute, Cary, NC, USA).
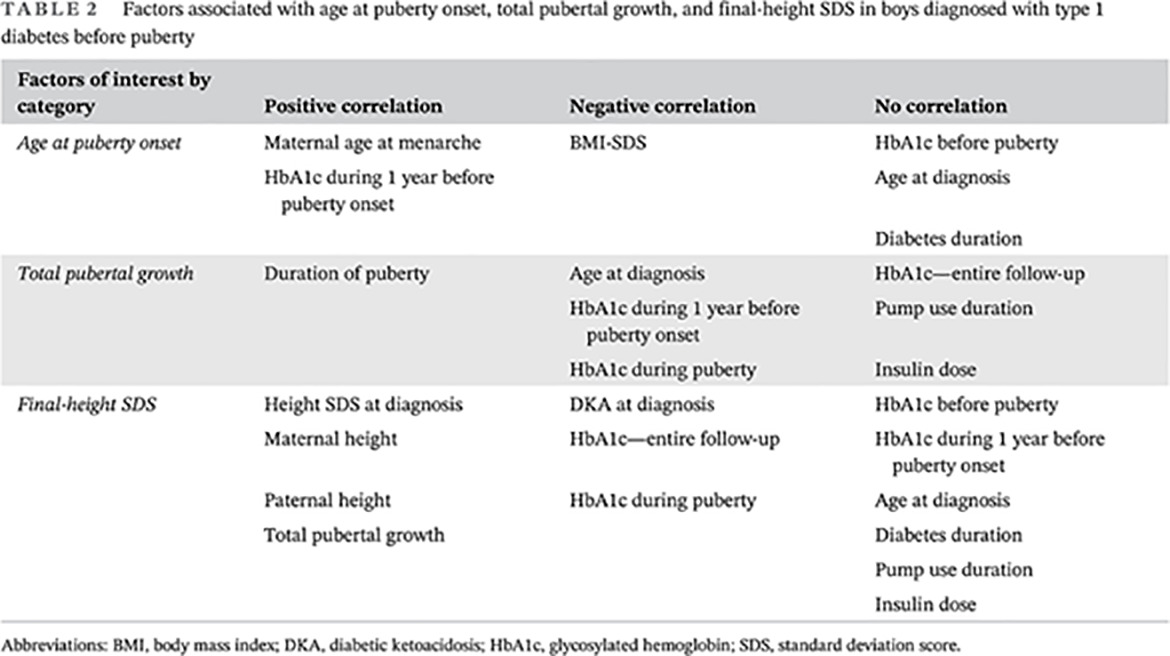
We included 88 177 patients with T1DM (n = 5456), T2DM (82018), MI-DM (n = 688), and CPI-DM (n = 15). Patients with T1DM were significantly younger at manifestation compared with CPI-DM (P < 0.001) (Table 1). In the unmatched cohort, DKA at manifestation was present in 0.6% (T1DM: 2.7%, T2DM: 0.4%, MI-DM: 0.9%, CPI-DM: 26.7%). Parameters before and after matching including standardized differences are described in Tables 1 and 2, respectively. All standardized differences regarding age, sex, and diabetes duration were <10% and therefore negligible.
TABLE 1. Demographics of the unmatched cohort in first documented treatment year Total T1DM T2DM MI-DM CPI-DM Standardized difference CPI-DM-T1DM Standardized difference CPI-DM–T2DM Standardized difference CPI-DM-MI-DM Number of cases 88 177 5456 82 018 688 15 Male sex (%) 57.0 58.1 56.9 53.9 53.3 −0.095 −0.072 −0.012 Age (y) 62.7 (51.8-74.0) 37.1 (27.0-51.5) 63.8 (53.4-74.6) 66.3 (54.5-74.7) 63.6 (57.8-72.9) 2.020 0.332 0.287 Diabetes duration (y) 0.4 (0.0-2.3) 0.2 (0.0-1.2) 0.4 (0.0-2.4) 0.0 (0.0-0.3) 0.1 (0.0-0.6) −0.492 −0.718 −0.096 Note. Data presented as median with interquartile range or as percentage. Abbreviations: CPI-DM, checkpoint-induced diabetes mellitus; MI-DM, medication-induced diabetes mellitus; T1DM, type 1 diabetes mellitus; T12DM, type 2 diabetes mellitus. TABLE 2. Demographics of the matched cohort in first documented treatment year Total T1DM T2DM MI-DM CPI-DM Standardized difference CPI-DM- T1DM Standardized difference CPI-DM–T2DM Standardized difference CPI-DM- MI-DM Number of cases 24 164 29 24 000 120 15 Male sex (%) 53.3 51.7 53.3 53.3 53.3 0.032 0.000 0.000 Age (y) 68.4 (57.3-78.4) 65.5 (57.5-73.6) 68.4 (57.3-78.4) 68.1 (55.8-74.1) 63.6 (57.8-72.9) 0.042 0.057 0.006 Diabetes duration (y) 0.1 (0.0-0.5) 0.1 (0.0-0.6) 0.1 (0.0-0.5) 0.0 (0.0-0.2) 0.1 (0.0-0.6) −0.024 0.014 0.020 Note. Data presented as median with interquartile range or as percentage. Abbreviations: CPI-DM, checkpoint-induced diabetes mellitus; MI-DM, medication-induced diabetes mellitus; T1DM, type 1 diabetes mellitus; T12DM, type 2 diabetes mellitus.The matched cohort consisted of 24 164 patients (99.3% T2DM, Table 2). Of the 120 MI-DM patients, 37 were classified as having cortisol-induced diabetes, 83 had diabetes induced by other medication (including, for example, pentamidine, niacin, and unspecified medication). Data at diagnosis of DM were available in 15 T1DM, 14 506 T2DM, 81 MI-DM, and 11 CPI-DM patients. During follow-up, data were available from 16 T1DM, 15 362 T2DM, 56 MI-DM, and 10 CPI-DM patients.
BMI was significantly higher in T2DM patients compared with CPI-DM (Table 3). At manifestation, HbA1c in T1DM and in CPI-DM was comparable but significantly higher compared with MI-DM (P = 0.04). During follow-up, HbA1c did not differ between CPI-DM and the other groups. DKA at manifestation was most frequently in CPI-DM (54.6%) compared with the other groups (T1DM: 0.0%, T2DM: 0.4%, MI-DM: 0.0%, all P < 0.01).
TABLE 3. Outcomes of the matched cohort in first documented treatment year Total T1DM T2DM MI-DM CPI-DM Body mass index (kg/m2) 29.8 (26.2–34.3) 24.7 (21.3-30.3) 29.8* (26.2-34.3) 25.8 (23.7-29.7) 26.8 (23.9–28.1) HbA1c at manifestation (%) 7.5 (6.3-10.1) 10.6 (10.1-12.1) 7.5 (6.3-10.1) 7.2* (5.8-8.9) 10.1 (8.0-12.5) HbA1c during follow-up (%] 6.6 (6.0-7.7) 6.1 (6.0-8.0) 6.6 (6.0-7.7) 6.6 (6.0-7.6) 7.5 (6.9-8.6) Daily insulin dose (IU/kg/d] 0.31 (0.18-0.51) 0.35 (0.21-0.52) 0.31 (0.18-0.51) 0.24 (0.13-0.46) 0.39 (0.35-0.50) DKA at manifestation (%] 0.4 0.0* 0.4** 0.0** 26.7 DKA during follow-up (%] 0.2 0.0 0.2 3.6 0.0 Autoimmune thyroid disease (%] 1.0 0.0* 1.0** 0.8** 26.7 Autoimmune hyperthyroidism (%] 0.2 0.0 0.2 0.0 0.0 Autoimmune thyroiditis (%] 0.8 0.0 0.8 0.8 13.3 Autoimmune adrenal insufficiency (%] 0.0 0.0 0.0** 0.0* 6.7 Autoimmune hepatitis (%) 0.0 0.0 0.0** 0.0* 6.7 Note. Data presented as median with interquartile range or as percentage. CPI-DM was reference group. * P value <0.05. ** P value <0.001. Abbreviations: CPI-DM, checkpoint-induced diabetes mellitus; DKA, diabetic ketoacidosis; MI-DM, medication-induced diabetes mellitus; T1DM, type 1 diabetes mellitus; T12DM, type 2 diabetes mellitus.Insulin requirement did not differ significantly between CPI-DM and T1DM. Insulin therapy in CPI-DM was required in 14 patients, where three additionally required OADs. T2DM patients mostly used lifestyle modification (38.8%), followed by OAD only (34.8%). Only 26.5% of individuals with T2DM required insulin (15.3% additional OAD). More than 52% of MI-DM patients were treated with insulin (10.8% additional OAD). The others were treated with lifestyle modification (31.7%) and OADs only (15.8%).
Autoimmune diseases such as thyroid disease (26.7%), adrenal insufficiency (6.7%), and autoimmune hepatitis (6.7%) were most common in CPI-DM, compared with all other groups (Table 3).
4 DISCUSSIONIn this study, we described and compared patients with CPI-induced DM with adult T1DM, T2DM, and medication-induced diabetes. We identified 15 cases of new-onset diabetes after initiation of CPI therapy. In the unmatched cohort, CPI-DM patients were older in their first documented treatment year compared with T1DM and similar in age as the T2DM/MI-DM patients. After matching for age, sex, and diabetes duration, HbA1c at manifestation was comparable between CPI-DM and T1DM, and significantly higher compared with MI-DM. Diabetes therapy was also comparable between CPI-DM and T1DM with a high percentage of patients with insulin treatment. Additional autoimmune diseases were significantly more frequent in CPI-DM compared to all other type of diabetes under investigation.
In the unmatched cohort, the older age at diagnosis of CPI-DM and the subgroup of patients with medication-induced diabetes compared with T1DM has been reported before18 and is not surprising, because cancer occurs more frequently with increasing age19 and the risk for corticoid-induced diabetes typically increases with a longer period of medical treatment.20
In our cohort, we had approximately equal numbers of men and women with CPI-DM. We would have expected a higher proportion of women, because women have a higher life expectancy compared to men. Female cancer patients have overall better outcomes and lower risk of death compared with male peers.21 On the other hand, CPI therapy is often administered in cancers that occur more frequently in men, such as lung cancer or melanoma.1, 22 Previous reports of CPI-DM patients even suggest a slightly higher male proportion of 55%-60% in cohorts of 71 and 91 cases respectively.1, 8 Given the small number of patients in our study, we can neither imply nor rule out a tendency toward preferential manifestation in men vs women. It is also possible that there is no sex difference concerning CPI-DM.
Beta cell antibodies could not be analyzed because there was only a small percentage of documented antibody diagnostics. In classic T1DM, antibody positivity is present in 80%-95% of cases,8 whereas in CPI-DM antibody positivity is lower at around 53% (mostly glutamic acid decarboxylase antibodies).8, 10
CPI-DM has been reported to be more DKA prone (50%-76%) compared with T1DM,8, 10, 18, 23, 24 which can also be seen in our cohort. This can be explained by the T-cell mediated extremely rapid destruction of beta cells in CPI-DM patients. If unrecognized, the resulting insulin deficiency leads to life-threatening DKA. However, DKA can be prevented by structured monitoring with regular glucose measurements and education programs on the symptoms of hyperglycemia and DKA. Together, these measures contribute to an early diagnosis before the onset of severe hyperglycemia or DKA. The unusual absence of any DKA at onset in T1DM could be attributed to the higher age of the matched patients25 and small number of T1D patients with available data at manifestation.
HbA1c at diagnosis was comparable between CPI-DM and T1DM5 and significantly higher compared to patients with medication-induced diabetes. Glucocorticoids have been reported to possibly mainly elevate postprandial blood-glucose, which may be the reason for the comparably low HbA1c in MI-DM compared with other diabetes types.26 On the other hand, in T1DM, T2DM, MI-DM, and CPI-DM HbA1c decreased during the follow-up as expected.
Almost all of our CPI-DM patients initiated insulin therapy within the first year of diabetes onset. Multiple studies suggest that all patients with CPI-induced DM required insulin after manifestation with difficulties concerning metabolic control despite good compliance and even after CPI discontinuation.1, 5, 10, 12 It is expected that eventually all CPI-DM patients will require therapy with insulin, either in monotherapy or with additional OADs for support. In our cohort, only around 50% of MI-DM patients needed insulin as monotherapy or in combination with OADs, and 32% controlled their diabetes with lifestyle modification only. Because our patient data were aggregated in the first documented year, it is not surprising that many patients first tried lifestyle modifications to lower their HbA1c, which is in agreement with recommendations of some caregivers.26 Finally, almost 40% of T2DM patients started their diabetes therapy with lifestyle modification, which is common before initiation of OADs and/or insulin. In concordance with recent American Diabetes Association guidelines for the treatment of T2DM,27 which endorse initial treatment with metformin before insulin is necessary, one third received OADs only and 15% OADs in combination with insulin.
Concomitant autoimmune diseases were found almost exclusively in the group of CPI-DM patients. Out of 15 patients, four were diagnosed with autoimmune thyroid disease, which was significantly more frequent compared with all other groups. This is at least partly due to CPIs influencing the immune system leaving the patients more prone to adverse autoimmune effects. Autoimmune thyroid disease was not present in the T1DM group. The prevalence of thyroid disease in T1DM has been reported previously in age-stratified analyses as 11.2%.28 Some T1DM patients may still develop thyroid disease with increasing diabetes duration. A study from Sweden suggested a 0.2% prevalence of Addison's disease in adult T1DM patients. However, in our matched cohort we did not find any T1DM patients with Addison's disease, but one patient with CPI-DM and Addison's disease. The limited number of T1DM patients in our cohort could explain the absence of the very rare Addison's disease in this group.
Strengths of our study include the study design with large number of patients with DM overall, which allowed matching of the identified 15 patients with new-onset CPI-DM to a large number of patients with other diabetes types who were similar in age, diabetes duration, and had the same sex distribution. Previous publications mostly presented case series, whereas our cohort consisted of 15 patients with CPI-DM who were compared to other diabetes forms. DPV has shown to be capable of contributing to the analysis of rare diabetes types in a meaningful way.29 Another strength is the multicenter nature of the DPV and the prospective data collection allowing for generalizability of our findings. One limitation is the lack of data at onset of CPI-DM, so we may not exclude more frequent events of DKA at diagnosis. Because patients are primarily treated by oncologists and not diabetologists, immunologic data on beta cell antibodies and C-peptide measurements were unfortunately too scarce to report, which prevented us from getting mechanistic insights of the disease onset.
The data from this controlled study show that CPI-DM is characterized by a high prevalence of DKA, autoimmune comorbidity, and metabolic decompensation at onset. Structured diagnostic monitoring is warranted to prevent DKA and other acute endocrine complications in CPI-treated patients.
ACKNOWLEDGEMENTSSpecial thanks to A. Hungele and R. Ranz for development of the DPV documentation software, K. Fink and E. Bollow for the DPV data management (clinical data managers, Ulm University), and Stefanie Lanzinger, PhD, for checking the statistical program and revising the manuscript. We further thank all centers contributing to this analysis: Aachen-Innere RWTH, Aidlingen Praxisgemeinschaft, Altötting-Burghausen Innere Medizin, Asbach Kamillus-Klinik Innere, Augsburg IV. Med. Uni-Klinik, Bad Aibling Internist. Praxis, Bad Aibling Internist. Praxis-2, Bad Driburg/Bad Hermannsborn Innere, Bad Hersfeld Innere, Bad Reichenhall Kreisklinik Innere Med., Bad Säckingen Hochrheinklinik Innere, Bayreuth Innere Medizin, Bensheim Heilig Geist Innere, Bergen Gemeinschaftspraxis, Berlin DRK-Kliniken Mitte Innere, Berlin Endokrinologikum, Berlin Evang. Krankenhaus Königin Elisabeth, Berlin Klinik St. Hedwig Innere, Berlin Oskar Zieten Krankenhaus Innere, Berlin Parkklinik Weissensee, Berlin Schlosspark-Klinik Innere, Berlin St. Josephskrankenhaus Innere, Berlin Vivantes Hellersdorf Innere, Bonn Schwerpunktpraxis, Bottrop Knappschaftskrankenhaus Innere, Bremen-Mitte Innere, Castrop-Rauxel Evangelisches Krankenhaus, Castrop-Rauxel Rochus-Hospital, Chemnitz-Hartmannsdorf Innere Medizin-DIAKOMED-1, Coburg Innere Medizin, Coesfeld/Dülmen Innere Med., Darmstadt Innere Medizin, Deggendorf Gemeinschaftspraxis, Deggendorf Medizinische Klinik II, Dortmund Knappschaftskrankenhaus Innere, Dortmund Medizinische Kliniken Nord, Dortmund-Hombruch Marienhospital, Dortmund-St. Josefshospital Innere, Dortmund-West Innere, Duisburg Malteser Rhein-Ruhr St. Anna Innere, Duisburg Malteser St. Johannes, Duisburg-Huckingen, Duisburg-Huckingen Malteser Rhein-Ruhr ST. Johannes, Duisburg-St.Johannes Helios, Eberswalde Klinikum Barnim Werner Forßmann-Innere, Eckernförde Gem.-Prax, Eisleben Lutherstadt Helios-Klinik, Erlangen Uni Innere Medizin, Essen Diabetes-SPP, Essen Diabetes-Schwerpunktpraxis, Forchheim Diabeteszentrum SPP, Frankfurt Diabeteszentrum Rhein-Main-Erwachsenendiabetologie (Bürgerhospital), Frankfurt Uni-Klinik Innere, Frankfurt Uni-Klinik Innere2, Frankfurt-Sachsenhausen Innere, Frankfurt-Sachsenhausen Innere MVZ, Freiburg Uni Innere, Friedberg Innere Klinik, Geislingen Klinik Helfenstein Innere, Gelnhausen Innere, Gießen Ev. Krankenhaus Mittelhessen, Göppingen Innere Medizin, Göttingen Uni Gastroenterologie, Güstrow Innere, Halberstadt Innere Med. AMEOS Klinik, Hamburg Endokrinologikum, Hanau diabetol. Schwerpunktpraxis, Hannover DM-SPP, Heidelberg St. Josefskrankenhaus, Heidenheim Arztpraxis Allgemeinmed, Heilbronn Innere Klinik, Herdecke Kinderklinik, Herford Innere Med I, Herne Evan. Krankenhaus Innere, Herten St. Elisabeth Innere Medizin, Hildburghausen Hennebergklinik, Hildesheim GmbH - Innere, Hohenmölsen Diabeteszentrum, Idar Oberstein Schwerpunktpraxis, Innsbruck Universitätsklinik Innere, Iserlohn Innere Medizin, Kamen Klinikum Westfalen Hellmig Krankenhaus, Kamen MKK - Medizinisches Kompetenzkollegium, Karlsburg Klinik für Diabetes & Stoffwechsel, Karlsruhe Schwerpunktpraxis, Kempen Heilig Geist - Innere, Kempen Heilig Geist-KHS-Innere, Kirchheim-Nürtingen Innere, Kleve Innere Medizin, Koblenz Kemperhof 1. Med. Klinik, Koblenz Kemperhof 1. Mediz. Klinik, Konstanz Innere Klinik, Krefeld Alexianer Innere, Krefeld Innere Klinik, Krefeld-Uerdingen St. Josef Innere, Landau Innere, Lilienthal Diabeteszentrum, Limburg Innere Medizin, Lindenfels Luisenkrankenhaus Innere, Lindenfels Luisenkrankenhaus Innere 2, Lindlar DM-Zentrum, Linz Krankenhaus Barmherzige Schwestern Kardiologie Abt. Int. II, Ludwigshafen diabetol. SPP, Lübeck Uni-Klinik Innere Medizin, Lünen Klinik am Park, Magdeburg Städtisches Klinikum Innere, Malchower See Rehaklinik, Manderscheid Rathauspraxis, Marburg - UKGM Endokrinologie & Diabetes, Marktredwitz Innere Medizin, Memmingen Internistische Praxis, Murnau am Staffelsee - diabetol. SPP, München Diabetes-Zentrum Süd, Münster Herz Jesu Innere, Münster Ludgerus-Kliniken GmbH, Neumarkt Innere, Neunkirchen Innere Medizin, Neuwied Marienhaus Klinikum St. Elisabeth Innere, Nidda Bad Salzhausen Klinik Rabenstein/Innere-1 Reha, Nidda Bad Salzhausen Klinik Rabenstein/Innere-2 Reha, Nürnberg Uniklinik Med. Klinik 4, Oberhausen Innere, Oberndorf Gastroenterologische Praxis Schwerpunkt Diabetologie, Offenbach/Main Innere Medizin, Oschersleben MEDIGREIF Bördekrankenhaus, Ottobeuren Kreiskrankenhaus, Pfullendorf Innere Medizin, Pirmasens Städtisches Krankenhaus Innere, Plauen Vogtlandklinikum, Prenzlau Krankenhaus Innere, Rastatt Kreiskrankenhaus Innere, Reutlingen Klinikum Steinenberg Innere, Rodalben St. Elisabeth, Rosenheim Innere Medizin, Rosenheim Schwerpunktpraxis, Rostock Universität Innere Medizin, Rottweil Gemeinschaftspraxis, Ruit Medius-Kliniken Innere, Saaldorf-Surheim Diabetespraxis, Scheidegg Prinzregent Luitpold, Schwerin Innere Medizin, Schwäbisch Hall Diakonie Innere Medizin, Spaichingen Innere, Stuttgart Sana Klinik Bethesda, Tettnang Innere Medizin, Timmendorfer Strand, Traunstein diabetol. Schwerpunktpraxis, Trostberg Innere, Ulm Agaplesion Bethesda-Krankenhaus, Ulm Schwerpunktpraxis Bahnhofsplatz, Viersen internist. Praxis, Villingen-Schwenningen Schwarzwald-Baar-Klinikum Innere, Wangen Oberschwabenklinik Innere Medizin, Weisswasser Kreiskrankenhaus, Wernberg-Köblitz SPP, Witten Kinderarztpraxis, Wittenberg Innere Medizin, Wittlich DSP, Wolgast Innere Medizin, Worms Schwerpunktpraxis, Wörth am Main SPP, and Zweibrücken Ev. KH. Innere. This work was supported by the German Centre of Diabetes Research (DZD) funded by the Federal Ministry of Education and Research (FKZ 82DZD14A02). The German Diabetes Association (DDG), the Robert Koch Institute (RKI), the Innovative Medicines Initiative 2 Joint Undertaking (INNODIA, grant agreement 115797), and INNODIA Harvest (grant agreement 945268) provided further financial support for the DPV registry. Open Access funding enabled and organized by Projekt DEAL.
DISCLOSURESThe authors declare none.
ETHICAL STANDARD STATEMENTThe registry was conducted in accordance with Good Epidemiology Practice and applicable regulatory requirements. The protocol of DPV was approved by the ethics committee of Ulm University (approval no. 202/09), and data collection was approved by local review board.
REFERENCES
1Akturk HK, Kahramangil D, Sarwal A, Hoffecker L, Murad MH, Michels AW. Immune checkpoint inhibitor-induced type 1 diabetes: a systematic review and meta-analysis. Diabet Med. 2019; 36: 1075- 1081. https://doi.org/10.1111/dme.14050 2Camacho LH. CTLA-4 blockade with ipilimumab: biology, safety, efficacy, and future considerations. Cancer Med. 2015; 4: 661- 672. https://doi.org/10.1002/cam4.371 3Ikegami H, Kawabata Y, Noso S. Immune checkpoint therapy and type 1 diabetes. Diabetol Int. 2016; 7: 221- 227. https://doi.org/10.1007/s13340-016-0276-9 4Byun DJ, Wolchok JD, Rosenberg LM, Girotra M. Cancer immunotherapy - immune checkpoint blockade and associated endocrinopathies. Nat Rev Endocrinol. 2017; 13: 195- 207. https://doi.org/10.1038/nrendo.2016.205 5Chuang P, Chao T, Hsieh Y. Type 1 diabetes mellitus with diabetic ketoacidosis after immune checkpoint inhibitor therapy. J Cancer Res Pract. 2018; 5: 153- 155. https://doi.org/10.1016/j.jcrpr.2018.08.003 6Bajwa R, Cheema A, Khan T, et al. Adverse effects of immune checkpoint inhibitors (programmed Death-1 inhibitors and cytotoxic T-lymphocyte-associated protein-4 inhibitors): Results of a retrospective study. J Clin Med Res. 2019; 11: 225- 236. https://doi.org/10.14740/jocmr3750 7Hasegawa T, Ozaki Y, Inoue T, et al. Nivolumab-related severe thrombocytopenia in a patient with relapsed lung adenocarcinoma: a case report and review of the literature. J Med Case Rep. 2019; 13:316. https://doi.org/10.1186/s13256-019-2245-y 8de Filette JMK, Pen JJ, Decoster L, et al. Immune checkpoint inhibitors and type 1 diabetes mellitus: a case report and systematic review. Eur J Endocrinol. 2019; 181: 363- 374. https://doi.org/10.1530/EJE-19-0291 9Castinetti F, Albarel F, Archambeaud F, et al. French Endocrine Society guidance on endocrine side effects of immunotherapy. Endocr Relat Cancer. 2019; 26: G1- G18. https://doi.org/10.1530/ERC-18-0320 10Kapke J, Shaheen Z, Kilari D, Knudson P, Wong S. Immune checkpoint inhibitor-associated type 1 diabetes mellitus: case series, review of the literature, and optimal management. Case Rep Oncol. 2017; 10: 897- 909. https://doi.org/10.1159/000480634 11Maamari J, Yeung SJ, Chaftari PS. Diabetic ketoacidosis induced by a single dose of pembrolizumab. Am J Emerg Med. 2019; 37: 376.e1- 376.e2. https://doi.org/10.1016/j.ajem.2018.10.040 12Alrifai T, Ali FS, Saleem S, et al. Immune checkpoint inhibitor induced diabetes mellitus treated with insulin and metformin: evolution of diabetes Management in the era of immunotherapy. Case Rep Oncol Med. 2019; 2019:8781347. https://doi.org/10.1155/2019/8781347 13Petersmann A, Müller-Wieland D, Müller UA, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes. 2019; 127: S1- S7. https://doi.org/10.1055/a-1018-9078 14Fathallah N, Slim R, Larif S, Hmouda H, Ben Salem C. Drug-induced Hyperglycaemia and diabetes. Drug Saf. 2015; 38: 1153- 1168. https://doi.org/10.1007/s40264-015-0339-z 15Karges B, Schwandt A, Heidtmann B, et al. Association of Insulin Pump Therapy vs insulin injection therapy with severe hypoglycemia, ketoacidosis, and glycemic control among children, adolescents, and young adults with type 1 diabetes.
留言 (0)