Sexually transmitted infections (STI) are a significant burden of disease in the United States, with an estimated 19.7 million incident infections in 2008.1 Although most STIs are asymptomatic or cause transient inflammation, some STIs, such as Chlamydia trachomatis and Neisseria gonorrhoeae, may be associated with significant reproductive harms.2,3
Accumulating evidence suggests that Mycoplasma genitalium, a common cause of male urethritis,4 may be associated with cervicitis, endometritis, pelvic inflammatory disease, and possibly tubal factor infertility in women.4–8 Although screening for C. trachomatis may effectively prevent pelvic inflammatory disease (PID) and subsequent infertility,9 the benefit of screening high-risk women for M, genitalium remains unclear and controversial.8 This may be because of limited knowledge on the potential reproductive harms associated with an asymptomatic infection, and because the burden of M. genitalium infections at the population level in the United States remains unclear. We therefore aimed to describe the overall and age-specific prevalence of M. genitalium, and the proportion of cases coinfected with other bacterial STIs in a population-based sample.
METHODS
We conducted a population-based, cross-sectional study using liquid-based cytology (LBC) residuals, with selections performed through collaboration with the New Mexico HPV Pap Registry (NMHPVPR).
Samples were obtained from 3 volunteering that who perform cervical screening tests on approximately 70% of the women receiving cervical cancer screening statewide (80% screening coverage10). After routine clinical testing, discarded LBC residuals were deidentified and subsequently stored at 4°C until testing. Using the NMHPVPR data resource, an age- and cervical cytology–stratified random sample of residual LBC specimens was selected for STI analysis (Table 1). This study was deemed exempt from approval by the University of New Mexico Human Research Review Committee.
TABLE 1 -
Sampling Fractions, Intended and Adjusted for Missing Values
Intended Sampling Design
Actual Sampling Design*
Cytology
Age, y (15 Strata)
Intended
Sampling Fraction, %
Sampling Weight
Age, y (13 Strata)
Actual Sample
Adjusted Population†
Sampling Fraction, %
Sampling Weight
Sample
Population
Normal
15–20
113
1529
7.39
13.53
21–24
683
7589
9.00
11.11
21–24
653
7589
8.60
11.62
25–30
1110
12472
8.90
11.24
25–30
1,071
12472
8.59
11.65
31–34
334
8350
4.00
25.00
31–34
318
8350
3.81
26.26
35–39
356
8476
4.20
23.81
35–39
347
8476
4.09
24.43
40–44
333
8538
3.90
25.64
40–44
323
8538
3.78
26.43
45–49
322
8474
3.80
26.32
45–49
308
8474
3.63
27.51
50–54
356
9368
3.80
26.31
50–54
343
9368
3.66
27.31
55–59
329
8436
3.90
25.64
55–59
316
8436
3.75
26.70
60–64
267
6846
3.90
25.64
60–64
251
6846
3.67
27.27
65+
201
5289
3.80
26.31
Total normal
4404
85,367
3930
78,549
ASCUS
All
2312
4624
50.00
2
21–64
2,124
4396
48.32
2.07
LSIL
All
732
1464
50.00
2
21–64
635
1348
47.11
2.12
ASC-H
All
223
223
100.00
1
21–64
199
209
95.22
1.05
HSIL
All
196
196
100.00
1
21–64
170
184
92.39
1.08
Total abnormal
3463
6507
3128
6137
Total
7867
91,874
7058
84,686
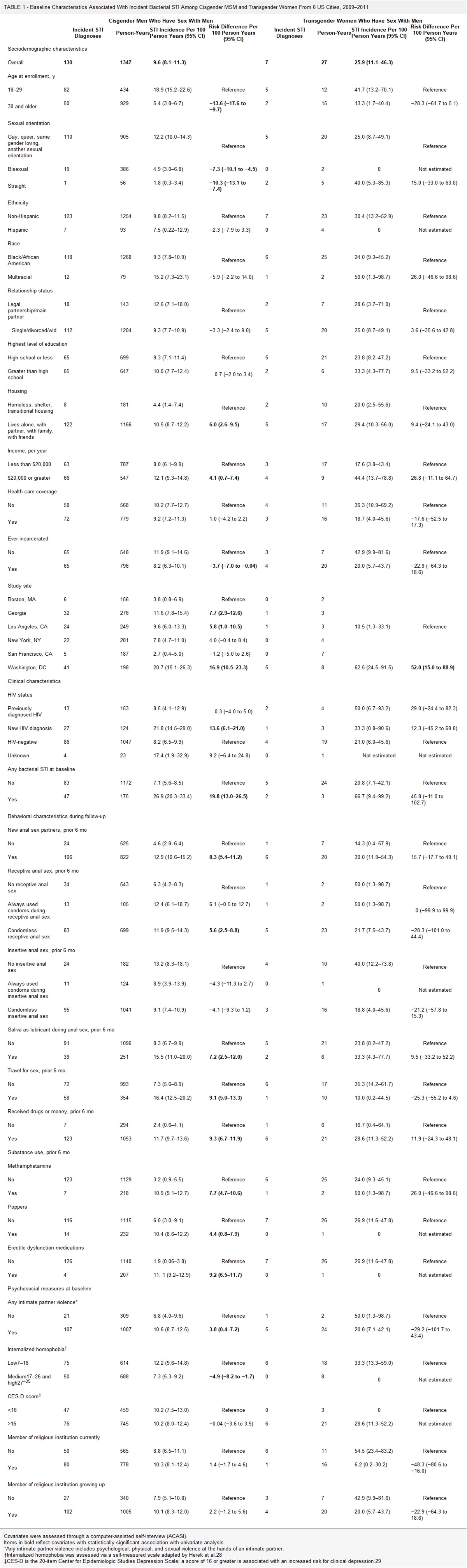
The table summarizes details on the intended and actual sampling design fractions and resulting weights used in the analysis to estimate population-level statistics. Actual sampling design weights in the last column were used.
*Actual sampling design adjusts for missing data.
†Population estimates as supplied by the NMHPVPR adjusted to reflect routine screening age.
The study population consisted of women who attended cervical cancer screening in New Mexico from August 1, 2013, to July 31, 2014. The sampling design was set up with the intention of oversampling younger women and women with abnormal cervical cytology to allow for the future estimation of cervical intraepithelial neoplasia risk associated with prevalent STIs (Table 1). Women were eligible for final analysis if they were aged 21 to 64 years and had valid test results for C. trachomatis, M. genitalium, Trichomonas vaginalis, Neisseria gonorrhoeae, and human papillomavirus (HPV).
From each LBC sample, we removed 1 mL and placed in an Aptima specimen transport kit (Hologic, cat. no. 301154c) according to the in vitro diagnostics product insert. Samples subsequently underwent testing at our University of New Mexico research laboratory for C. trachomatis and N. gonorrhoeae using the US Food and Drug Administration (FDA)–approved Aptima Combo2 assay (Hologic), for T. vaginalis using the FDA-approved Aptima T. vaginalis assay (Hologic), and for HPV using the FDA-approved Aptima HPV assay (Hologic). Testing for M. genitalium was performed using a prototype of the Aptima M. genitalium assay (Hologic), which received FDA approval January 23, 2019. All STI analyses were performed on the Panther platform, a fully automated system, following the manufacturer's instructions. Results were recorded as positive, negative, invalid, or equivocal (C. trachomatis only). Invalid test results were excluded from final analysis as missing (n = 297). Equivocal results on C. trachomatis (n = 1) were considered positive.
We calculated weighted population prevalence estimates of M. genitalium, including 95% confidence intervals (CIs), overall and by age (21–24, 25–30, 31–34, 35–39, and 40–64 years; Table 1). Estimates were calculated by weighting back to 84,686 women with an available LBC residual. Weighted logistic models were fit to test for trend in prevalence with increasing age. The sampling fractions and weights (inverse of the sampling fractions) were adjusted to reflect missing data. In addition, we calculated the prevalence of pairwise coinfections between M. genitalium and C. trachomatis and between M. genitalium and T. vaginalis. Analyses were conducted in Stata version 13 (StataCorp. College Station, TX) using the Survey (SVY) commands.
RESULTS
A total of 84,686 residual LBC samples from New Mexico laboratories were available for testing, from which 7867 (9.3%) were originally selected for STI analysis using stratified random sampling (Table 1). From these, we excluded samples from women outside of the age range for routine cervical screening <21 (n = 297) and >64 years (n = 305) and samples with incomplete STI panel results (missing sample aliquots [n = 111], invalid test runs with one or more STI panel [n = 217]), leaving 7057 with complete test results in the final analysis.
The overall weighted population prevalence of M. genitalium was 1.95% (95% CI, 1.62%–2.34%), with significant differences by age group. The prevalence was highest in women aged 21 to 24 years (6.12%; 95% CI, 4.72%–7.92%) and declined steadily as women aged, to 0.48% (95% CI, 0.25%–0.94%) in women aged 40 to 64 years (Ptrend < 0.0001; Table 2). Overall, the prevalence of coinfections was low (0.25% for M. genitalium and C. trachomatis and 0.29% for M. genitalium and T. vaginalis). Highest rates of M. genitalium and C. trachomatis coinfection were in women aged 21 to 24 years (1.26%; 95% CI, 0.70%–2.27%) and declined significantly with increasing age (Ptrend = 0.003; Table 2). Similarly, highest rates of M. genitalium and T. vaginalis coinfection were in women aged 21 to 24 years (0.78%; 95% CI, 0.37%–1.66%), with declining rates as age increased (Ptrend = 0.012).
TABLE 2 -
Weighted Prevalence Estimates of Mycoplasma genitalium and Chlamydia trachomatis and Trichomonas vaginalis Coinfections Among Women Aged 21 to 64 Years Attending Routine Cervical Cancer Screening in New Mexico
Age, y
n
Mycoplasma genitalium Prevalence, % (95% CI)
Coinfection Prevalence, % (95% CI)
Chlamydia trachomatis
Trichomonas vaginalis
All
84,686
1.95 (1.62–2.34)
0.25 (0.15–0.43)
0.29 (0.18–0.47)
21–24
8765
6.12 (4.72–7.92)
1.26 (0.70–2.27)
0.78 (0.37–1.66)
25–30
13,916
3.65 (2.78–4.77)
0.12 (0.03–0.49)
0.66 (0.35–1.23)
31–34
9069
2.72 (1.50–4.87)
0.59 (0.15–2.28)
0.05 (0.01–0.18)
35–39
9180
1.61 (0.78–3.32)
0.05 (0.01–0.18)
0.27 (0.04–1.87)
40–64
43,756
0.48 (0.25–0.94)
0.06 (0.01–0.43)
0.13 (0.03–0.48)
DISCUSSION
In this population-based study, we assessed the weighted population prevalence of M. genitalium among women aged 21 to 64 years, attending routine cervical cancer screening in New Mexico. We found an overall M. genitalium prevalence of 1.95%, with highest rates among women aged 21 to 24 years (6.12%). The majority of M. genitalium infections across all ages occurred as single infections.
The observed prevalence of M. genitalium was more than 2-fold higher than the prevalence reported in a previous population-based US study in which asymptomatic individuals aged 18 to 27 years were tested (2.0% vs. 0.8%),11 although the latter test used different tests and sample types, which may have affected their test sensitivity relative to more recently validated tests. The prevalence in our study was much lower than prevalence rates based on individuals with symptoms or seeking care at STD clinics (2.0% vs. up to 26%).12–14 The high M. genitalium prevalence in the present study, particularly among the youngest women, is concerning because these estimates may reflect a significant number of asymptomatic women. If these infections remain undetected and untreated, these women may not only be at risk for future disease themselves but may also provide a reservoir for further transmission.
Among women aged 21 to 24 years, the prevalence of M. genitalium was 2-fold higher than the prevalence of C. trachomatis reported in the 2007–2012 National Health and Nutrition Examination Survey (6.1% vs. 2.9%),15 but similar to the C. trachomatis prevalence in the present study (6.12% vs. 6.22%). Whereas efforts are made to reduce the burden of C. trachomatis and associated disease by screening individuals,16 no efforts are currently in place to reduce the burden of M. genitalium, despite that screening for STI may be efficacious at prevalence rates greater than 3.1%.17 Screening and treatment of C. trachomatis are associated with a lower risk of PID and infertility,2,9,18 but screening for M. genitalium remains controversial, mainly because PID is more commonly attributed to C. trachomatis than M. genitalium.8 However, these estimates were based on much lower prevalence rates. Well-designed prospective studies are needed to assess the potential impact of screening for M. genitalium on reproductive harms.19
The relatively low rate of coinfections between M. genitalium and C. trachomatis may be partially explained by treatment effects on M. genitalium in women with screen-detected C. trachomatis infections. This may also explain the reported increase in macrolide resistance for M. genitalium over time, up to 42% to 69% in the United States, with an increased risk of resistance among individuals with coinfections and with important differences by sex, race, and sexual orientation.14,20–23 To reduce the burden of M. genitalium and risk of treatment failure, increased awareness of this emerging pathogen and correct diagnostics are critical. Routine testing for M. genitalium should be considered when women present with symptoms or clinical evidence of infection, particularly in case of treatment failure. Testing may also be considered before invasive procedures among women at high risk for being infected, such as women undergoing surgical abortion, as this would allow for adequate diagnostics and treatment, which subsequently may reduce risk for postoperative complications, including PID.24 This may be critical, as the prophylaxis used in conjunction with surgical abortion (i.e., doxycycline)25 does not confer antimicrobial eradication of M. genitalium.
Our sampling frame reflects women attending cervical screening in New Mexico. Although we believe that this provides a stronger population-based sample compared with clinic-based data, it cannot be taken as a true population-based sample. Prevalence rates may be underestimated, as women not attending cervical cancer screening may have a higher prevalence of STI because of lower access to care and, possibly, shared risk factors. On the other hand, prevalence rates may be overestimated, as women undergoing screening may have been screened because of symptoms. Finally, we cannot rule out that rates of C. trachomatis and M. genitalium coinfections may have been underestimated, as we have no knowledge on previous testing and treatment of C. trachomatis.
REFERENCES
1. Satterwhite CL, Torrone E, Meites E, et al. Sexually transmitted infections among US women and men: Prevalence and incidence estimates, 2008. Sex Transm Dis 2013; 40:187–193.
2. Hoenderboom BM, van Benthem BHB, van Bergen J, et al. Relation between Chlamydia trachomatis infection and pelvic inflammatory disease, ectopic pregnancy and tubal factor infertility in a Dutch cohort of women previously tested for chlamydia in a chlamydia screening trial. Sex Transm Infect 2019; 95:300–306.
3. Reekie J, Donovan B, Guy R, et al. Risk of pelvic inflammatory disease in relation to chlamydia and gonorrhea testing, repeat testing, and positivity: A population-based cohort study. Clin Infect Dis 2018; 66:437–443.
4. Falk L, Fredlund H, Jensen JS. Signs and symptoms of urethritis and cervicitis among women with or without Mycoplasma genitalium or Chlamydia trachomatis infection. Sex Transm Infect 2005; 81:73–78.
5. Lis R, Rowhani-Rahbar A, Manhart LE. Mycoplasma genitalium infection and female reproductive tract disease: A meta-analysis. Clin Infect Dis 2015; 61:418–426.
6. Cohen CR, Manhart LE, Bukusi EA, et al. Association between Mycoplasma genitalium and acute endometritis. Lancet 2002; 359:765–766.
7. Cohen CR, Mugo NR, Astete SG, et al. Detection of Mycoplasma genitalium in women with laparoscopically diagnosed acute salpingitis. Sex Transm Infect 2005; 81:463–466.
8. Lewis J, Horner PJ, White PJ. Incidence of pelvic inflammatory disease associated with Mycoplasma genitalium infection: Evidence synthesis of cohort study data. Clin Infect Dis 2020; 71:2719–2722.
9. Scholes D, Stergachis A, Heidrich FE, et al. Prevention of pelvic inflammatory disease by screening for cervical chlamydial infection. N Engl J Med 1996; 334:1362–1366.
10. Cuzick J, Myers O, Hunt WC, et al. A population-based evaluation of cervical screening in the United States: 2008–2011. Cancer Epidemiol Biomarkers Prev 2014; 23:765–773.
11. Manhart LE, Holmes KK, Hughes JP, et al. Mycoplasma genitalium among young adults in the United States: An emerging sexually transmitted infection. Am J Public Health 2007; 97:1118–1125.
12. Huppert JS, Mortensen JE, Reed JL, et al. Mycoplasma genitalium detected by transcription-mediated amplification is associated with Chlamydia trachomatis in adolescent women. Sex Transm Dis 2008; 35:250–254.
13. Bachmann LH, Kirkcaldy RD, Geisler WM, et al; MAGNUM Laboratory Working Group. Prevalence of Mycoplasma genitalium infection, antimicrobial resistance mutations, and symptom resolution following treatment of urethritis. Clin Infect Dis 2020; 71:e624–e632.
14. Khosropour CM, Jensen JS, Soge OO, et al. High prevalence of vaginal and rectal Mycoplasma genitalium macrolide resistance among female sexually transmitted disease clinic patients in Seattle, Washington. Sex Transm Dis 2020; 47:321–325.
15. Torrone E, Papp J, Weinstock H; Centers for Disease Control and Prevention (CDC). Prevalence of Chlamydia trachomatis genital infection among persons aged 14–39 years—United States, 2007–2012. MMWR Morb Mortal Wkly Rep 2014; 63:834–838.
17. Marrazzo JM, Celum CL, Hillis SD, et al. Performance and cost-effectiveness of selective screening criteria for Chlamydia trachomatis infection in women. Implications for a national chlamydia control strategy. Sex Transm Dis 1997; 24:131–141.
18. Moore MS, Golden MR, Scholes D, et al. Assessing trends in chlamydia positivity and gonorrhea incidence and their associations with the incidence of pelvic inflammatory disease and ectopic pregnancy in Washington state, 1988–2010. Sex Transm Dis 2016; 43:2–8.
19. Wiesenfeld HC, Manhart LE. Mycoplasma genitalium in women: Current knowledge and research priorities for this recently emerged pathogen. J Infect Dis 2017; 216(suppl_2):S389–S395.
20. Xiao L, Waites KB, Van Der Pol B, et al. Mycoplasma genitalium infections with macrolide and fluoroquinolone resistance-associated mutations in heterosexual African American couples in Alabama. Sex Transm Dis 2019; 46:18–24.
21. Getman D, Jiang A, O'Donnell M, et al. Mycoplasma genitalium prevalence, coinfection, and macrolide antibiotic resistance frequency in a multicenter clinical study cohort in the United States. J Clin Microbiol 2016; 54:2278–2283.
22. Romano SS, Jensen JS, Lowens MS, et al. Long duration of asymptomatic Mycoplasma genitalium infection after syndromic treatment for nongonococcal urethritis. Clin Infect Dis 2019; 69:113–120.
23. De Baetselier I, Kenyon C, Vanden Berghe W, et al. An alarming high prevalence of resistance-associated mutations to macrolides and fluoroquinolones in Mycoplasma genitalium in Belgium: Results from samples collected between 2015 and 2018. Sex Transm Infect 2021; 97:297–303.
24. Bjartling C, Osser S, Persson K. The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. BJOG 2010; 117:361–364.
25. Achilles SL, Reeves MF; Society of Family Planning. Prevention of infection after induced abortion: Release date October 2010: SFP guideline 20102. Contraception 2011; 83:295–309.


留言 (0)