
記住我

Rates of bacterial sexually transmitted infections (STIs) in the United States among sexual and gender minorities such as cisgender men who have sex with men (MSM) and transgender women (TGW) have been steadily increasing since the mid-1990s.1–3 In addition, between 2015 and 2019, the rates of Neisseria gonorrhoeae (GC) and Chlamydia trachomatis (CT) diagnoses among all men, including cisgender men who have sex with women, have gone up by 60.6% and 32.1%, respectively.4 The observed changes in rates of both GC and CT are likely to be multifactorial and may be partly attributable to increased screening among MSM at extragenital sites, more frequent screening (e.g., for MSM who take HIV preexposure prophylaxis [PrEP]), and greater sensitivity of diagnostic tests, although increased transmission is likely to contribute.4
The current standard for diagnosing GC/CT infection uses nucleic acid amplification testing (NAAT), which offers increased sensitivity compared with bacterial culture and can be performed more rapidly.5 Routine bacterial STI NAAT typically takes 3 to 5 days to result with reported sensitivity of greater than 90% and specificity of 98% (routine NAAT).3,6–8 The time taken to receive results of GC/CT testing directly impacts the time between testing and treatment.9 The average time to treatment for GC or CT using routine NAAT modalities varies in the literature, ranging from 7 to 30 days.10–12 Minimizing the time to treatment is important as approximately 50% of patients with positive GC/CT test results, even if symptomatic, continue to have sex in the interval between diagnosis and treatment.11,13 Although empiric treatment pending STI test results is an option, 2 inner-city emergency departments showed that this approach resulted in both overtreatment of more than 45% of participants without infection and undertreatment of participants with infection.14,15 Any increase in time delay between testing and treatment is highly undesirable for several reasons including a risk for loss to follow-up, secondary STI transmission, complications of untreated infection, and increased risk of acquiring or transmitting other infections such as HIV.16,17
The polymerase chain reaction Cepheid GeneXpert (Sunnyvale, CA) test provides rapid diagnosis and differentiation between GC and CT resulting within 90 minutes, making same-day diagnosis and treatment possible (rapid NAAT).18 Studies evaluating cost-effectiveness of and implementation strategies for rapid NAAT testing in a US public health system are lacking.19 Rapid NAAT STI testing has been shown to be cost-effective when taking into consideration cost of sequelae of untreated infections, decrease in inappropriate treatment, and transmissions prevented in studies conducted in the United Kingdom that included persons regardless of sex assigned at birth, gender identity, and sexual orientation.9,20–22 It remains unclear, however, if this strategy would be cost-effective if implemented in the United States among MSM and TGW.
We evaluated the impact on time to treatment of rapid NAAT compared with routine NAAT.10–12 We also evaluated the incremental cost per infectious day averted of rapid NAAT testing compared with routine NAAT and the total cost of implementing this new modality at scale at the public STI clinics of the County of San Diego Health and Human Services Agency (SD-HHSA).
MATERIALS AND METHODS Time to TreatmentTime to treatment estimates for rapid NAAT were abstracted from data collected as part of the National Institutes of Health–funded Primary Infection Resource Consortium study. Briefly, between November 2018 and February 2021, adult MSM and TGW in San Diego, CA, were screened with the “total test” for bacterial (GC, CT, and syphilis) and viral (HIV, hepatitis B virus, and hepatitis C virus) STIs in a community-based sexual health clinic. Study participants provided self-collected samples from 3 anatomical sites (urethral, oropharyngeal, and rectal) and underwent phlebotomy for syphilis testing.
Rapid NAAT for GC/CT was performed using Cepheid GeneXpert (Sunnyvale, CA). Participants who tested positive for GC/CT at any anatomic site were notified by text message or email within 90 minutes to 2 hours after STI testing with instructions to call and schedule an appointment immediately (ideally the same day) for treatment. Participants who did not respond within 24 hours were contacted by the study team to arrange treatment follow-up. Treatment was provided according to Centers for Disease Control and Prevention guidelines at the primary research facility located 2 miles from the community-based sexual health clinic.1 A questionnaire was completed at the time of treatment to assess site-specific symptoms consistent with bacterial STIs. Individuals were classified as symptomatic for urethral GC/CT if they reported abnormal urethral discharge, bleeding, pain during intercourse, pain or burning with urination, or discharge from penis, and classified as symptomatic for rectal GC/CT if they reported anorectal pain, discharge, or bleeding. Some with site-specific GC/CT infections reported vague and nonlocalizing symptoms that were not site-specific, so these data were not included in the final analysis. Individuals who received STI treatment at another facility or were lost to follow-up were excluded from the study analysis. Among those included in the treatment analysis, the median time from sample collection to treatment delivery was calculated.
As a comparator, estimates of historical time to treatment using routine NAAT among a broad population of cisgender men and women, TGW, and MSM were abstracted from the literature.10–12
Cost Analysis Cost of Rapid GC/CT TestingThe total unit cost per test for rapid NAAT was calculated using an ingredients-based micro-costing approach23 and based on the guidance from the Global Health Cost Consortium Reference Case for Estimating the Costs of Global Health Services and Interventions.24 We estimate the financial cost from a health care provider perspective. We estimated costs for 1 year (2019). Cost data were classified as recurrent (i.e., personnel and nonpersonnel) and nonrecurrent (capital). Equipment and laboratory test costs were obtained from the manufacturer, and the remaining costs were collected from financial records. Capital costs consisted of price of the rapid GC/CT instrument. As recommended by the GHCC Reference Case, capital costs should be amortized using straight line depreciation to reflect the expected life of the capital input. Therefore, the cost of equipment was divided by the expected life span of the instrument provided by the supplier to determine an annual capital cost.
Recurrent nonpersonnel costs included costs of building space, supplies, utilities, and services such as maintenance and security. Recurrent personnel costs included laboratory technicians and housekeeping. To calculate the time used to perform rapid GC/CT testing, 3 sexual health clinic laboratory technicians were given time logs to document the time spent doing GC/CT testing duties during a period of 9 days. We multiplied laboratory technician hourly wages by the average time in hours spent performing a GC/CT test to determine personnel costs. Because the clinic was devoted to other activities in addition to rapid GC/CT testing, we attributed a fraction of the yearly cost for cleaning, rent, utilities, security, Wi-Fi, and phone to the rapid testing by multiplying these total costs by the proportion of clinic space occupied by the rapid GC/CT equipment.
We then summed the total annual costs of the intervention and divided by the total GC/CT tests run per year to determine the unit cost per test (in 2019 US dollars). To account for potential differences in cost depending on intervention scale, we performed a sensitivity analysis on how unit cost changes with different annual testing volumes.
Cost of Routine GC/CT NAAT Using the Aptima Combo-2 Assay at the County of San Diego HHSAUnit costs per routine GC/CT NAAT were provided by HHSA for the fiscal year 2019 (at each of the 4 STI clinics) to provide cost data before patient testing restrictions associated with the global COVID-19 pandemic. Unit costs were obtained from HHSA and included recurrent personnel and nonpersonnel costs. Recurrent personnel costs included laboratory technicians and staff. Recurrent nonpersonnel included cost of equipment, supplies, and overhead.
We did not include the purchase price of the Aptima machine itself, as it is used to perform a variety of tests and is not used solely for GC/CT NAAT. We assumed equivalent time spent for individual education and sample collection for rapid and routine NAAT.
Cost-Effectiveness AnalysisWe performed a cost-effectiveness analysis comparing rapid GC/CT NAAT with routine NAAT. Costs were identified in monetary terms and the effect in number of infectious days averted described in an incremental cost-effectiveness ratio (ICER) expressed by the equation:
ICER=C1-C2/E1-E2
where C1 and E1 are the cost (2019 US dollars) and effect (time from sample collection to treatment) of rapid GC/CT NAAT, and C2 and E2 are the cost and effect of routine GC/CT NAAT. The outcome reported is therefore the incremental cost per untreated day averted.
Cost of Scale-Up of Rapid NAAT Across the County of San Diego HHSA STI ClinicsWe estimated the cost of scale-up of rapid NAAT across the county of San Diego HHSA STI Clinics. Scale-up costs of rapid GC/CT NAAT at HHSA STI clinics included the costs of GeneXpert equipment purchase for each of the 4 clinics. The size and therefore the cost of rapid testing equipment (C. Meyrath, personal communication [Cepheid]) used at each of the 4 STI clinics were selected based on the average number of tests per day performed at each site during the period January 2019–May 2019. The annual recurrent costs after implementation of the rapid testing program were based on our estimate of cost of rapid testing supplies as well as costs provided by HHSA including cost for personnel required to perform testing at each clinic, maintenance, and overhead. We replaced supply costs for routine testing with supply costs specific for rapid NAAT to calculate a total unit cost per test.
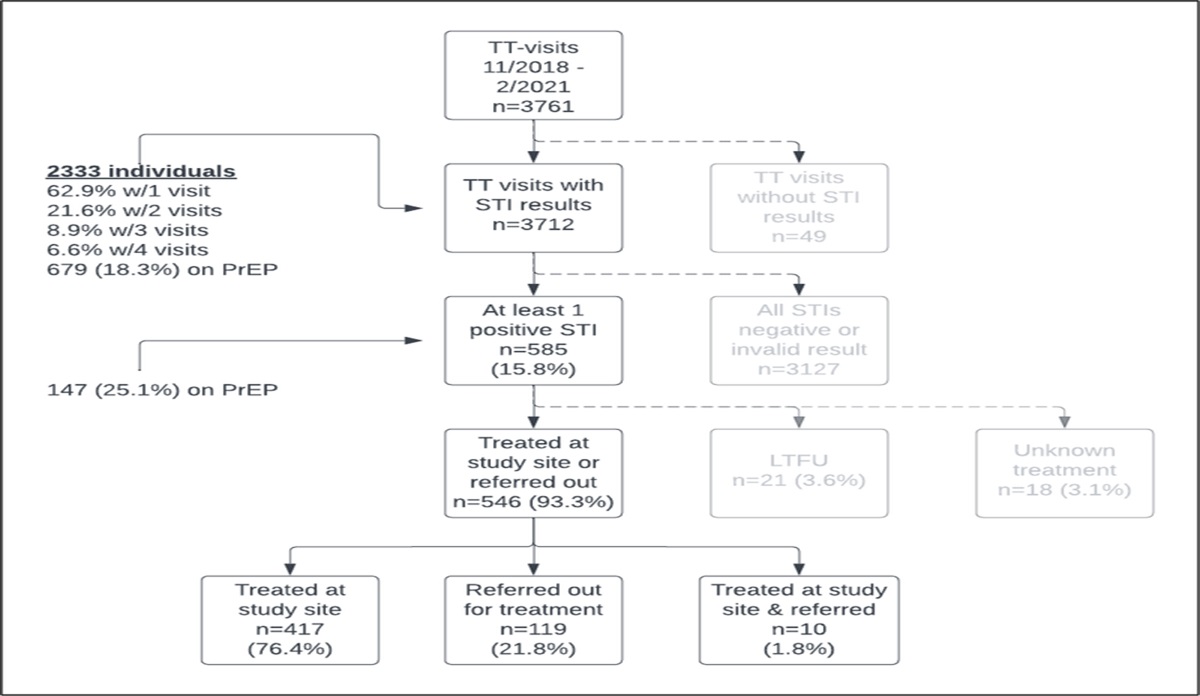
RESULTSBetween November 26, 2018, and February 28, 2021, a total of 2333 individuals received 3761 rapid NAAT results for GC or CT reported as positive, negative, or invalid with 49 results missing or unknown (Figure 1). Most participants were White, non-Hispanic (43.2%), and assigned male sex at birth (98.2%) (Table 1). From 585 positive test results, 21 were lost to follow-up, treatment ascertainment was missing for 18, and 119 were referred to outside providers for treatment. The remaining 427 positive results from 377 individuals were treated at the study site and were included in the time to treatment analysis (some individuals received treatment more than once).
 Figure 1:
Figure 1: Study design. Total test (TT) visits were from November 26, 2018, to February 28, 2021, and were included in the analysis. Time to treatment data only included participants who were treated at the study site. Participants who were exclusively referred out were excluded from time to treatment calculations. LTFU indicates lost to follow-up; TT, total test.
TABLE 1 - Demographics of Participants Undergoing Rapid NAAT for Neisseria gonorrhoeae and Chlamydia trachomatis n (%) Sex at birth Male 2291 (98.2) Female 41 (1.8) Unknown 1 (0.04) Race/ethnicity White, non-Hispanic 1009 (43.2) Black, non-Hispanic 150 (6.4) Hispanic 813 (34.8) Asian/PI (non-Hispanic) 245 (10.5) Native American/Alaskan Native (non-Hispanic) 4 (0.2) Other (includes multiracial) 93 (4.0) Unknown 19 (0.8) Risk factors among those treated on-site Condomless, penetrative anal intercourse 364 (85.4) Condomless, receptive anal intercourse 248 (58.2)Of the individuals with GC/CT results included in the analysis, there were 205 positive tests for GC from 152 individuals (6.6% of all tests) and 256 positive tests for CT from 225 individuals (9.8% of all tests; see Supplementary Data for testing site breakdown, https://links.lww.com/OLQ/B74). Among individuals with a positive GC/CT result, 85.4% reported condomless penetrative anal intercourse in the past 3 months, 25.1% were taking HIV PrEP, and the median number of sexual partners in the past 3 months was 4 (range, 0–58).
The median time from specimen collection to STI treatment for rapid GC/CT NAAT was 2 days (range, 0–16 days), and the time to treatment for routine GC/CT NAAT using conservative estimates from literature review was 7 to 14 days.10–12 Use of rapid NAAT therefore resulted in a reduction in posttesting transmission risk duration of approximately 5 to 12 days compared with routine NAAT strategies. For all calculations, the range of 5 to 12 days of posttesting risk duration was used to evaluate incremental cost-effectiveness.
Rapid and Routine GC/CT NAAT Unit Cost Per TestThe total unit cost of rapid GC/CT NAAT was $57.86 compared with $18.38 (Table 2) for routine GC/CT NAAT. For rapid NAAT, recurrent nonpersonnel costs represented the most substantial component with individual cartridges costing $38.00 per test. Purchase of the rapid NAAT (GeneXpert) instrument represented the largest start-up cost to a rapid GC/CT testing program and contributes to the high unit cost per test. At the sexual health study clinic, the 16-cartridge GeneXpert instrument had a cost of $174,000 with an average life span of 10 years. Recurrent nonpersonnel costs were the biggest contributor to cost of routine GC/CT NAAT as well, but the total unit cost per test was cheaper compared with rapid GC/CT NAAT.
TABLE 2 - Cost Per Test Per Year for Rapid and Routine GC/CT NAAT Rapid GC/CT NAAT Fixed cost (capitol) $6.68 Recurrent costs (personnel) $3.54 Recurrent costs (nonpersonnel) $47.64 Total unit cost per test $57.86 Routine GC/CT NAAT Labor and supply costs per test $17.71 Services costs per test $0.67 Total unit cost per test $18.38The median number of infectious days was reduced by 5 to 12 days using rapid GC/CT NAAT compared with routine NAAT, although it was costlier. The ICER for rapid GC/CT NAAT ranged from $5.12 to $12.30 per infectious day averted when 1000 tests were run per year. Rapid NAAT became more cost-effective by increasing the number of tests run per year with the ICER ranging from $2.43 to $5.82 per infectious day averted when running 10,000 tests per year (Figure 2). Based on 10 minutes required to prepare, load, and unload a specimen and 90 minutes for a test to run, the total capacity of a 16-chamber instrument during a 5-day work week is 384 tests or more than 19,000 tests per year.
 Figure 2:
Figure 2: Incremental cost per infectious days averted.
Replacing Routine NAAT With Rapid GC/CT NAAT at the County of San Diego HHSAImplementing and scaling up rapid GC/CT testing in the HHSA of San Diego County would eliminate the need for specimens to be sent to the central public health laboratory by allowing each clinic to perform tests on-site. The personnel needed to perform rapid GC/CT NAAT at each testing site is already available, so hiring new testers is not required. Of the 4 STI clinics in HHSA, the Rosecrans clinic performed the greatest mean daily tests (N = 29) and would require the largest rapid GC/CT testing equipment. The other STI clinics averaged between 1 and 4 tests per day and would need the smallest rapid testing machine to function (see Supplementary Data, https://links.lww.com/OLQ/B74). Purchasing rapid GC/CT NAAT for all 4 county STI clinics in San Diego would cost $307,600 with annual recurrent costs estimated to be $621,204 across all sites (Table 3).
TABLE 3 - Cost of Implementing and Maintaining Rapid GC/CT NAAT at Public Health Service Centers Public Health STI Clinic Cost of Rapid GC/CT Testing Equipment Annual Recurrent Cost Central Region PH Center $44,400 $73,841.28 North Coastal PH Center $44,400 $50,687.98 Rosecrans STD $174,400 $476,468.03 South Region PH Center $44,400 $20,206.34 Combined centers $307,600 $621,203.63Our study demonstrated that implementing a rapid NAAT testing strategy can reduce the time lag between testing and treatment for GC and CT STIs by up to 12 days compared with routine NAAT standard of care. If testing volumes were increased to 10,000 tests per year in San Diego County, we estimated that the cost per infectious day averted could be in the range from $2.43 to $5.82. To implement this strategy across 4 public health testing sites in San Diego would cost approximately $307,600 in initial outlay with $621,204 in recurrent costs each year.
Previous work has estimated that direct medical costs of treatment for CT and GC are around $151 and $85, respectively (2016 dollars) in addition to productivity loss from individuals presenting for testing and/or treatment.25 When combined with our results indicating that individuals were at ongoing high risk for STI transmission and previous data suggesting that most persons continue to have sex between testing and treatment, it is likely that the costs of each infectious day averted might be partially or completely offset by infections averted.11,13 These potential cost benefits of rapid NAAT testing are in addition to providing a faster and more convenient STI health service.
Sexual health clinics such as the Dean Street Express clinic in the United Kingdom have reported similar findings regarding decreased time to treatment with rapid GC/CT NAAT from over a week to just a few hours.20 They also demonstrated a substantial decrease in partner attendance and decreases in GC and/or CT transmissions.20 In a similar fashion, the New York City public health department reduced the time to treatment from 8 to 2 days after replacing routine NAAT with rapid GC/CT NAAT (GeneXpert).10
As with many new technologies, our study shows that rapid GC/CT NAAT is more costly than routine NAAT but reduces infectious days. As the volume of tests increased, the cost per infectious day averted decreased. In the current health care model, many health care systems with multiple clinics send GC/CT laboratory specimens to a central laboratory and can run tests in batches. Rapid GC/CT NAAT supports immediate on-site testing. The issue then becomes whether a clinic runs enough tests to justify the cost as even the smallest GeneXpert instrument requires a substantial investment. A pilot study for rapid GC/CT testing and same-day treatment among MSM found that most participants felt positive about receiving test results quickly, which may lead to more diagnostic testing and treatment thus potentially justifying the investment even in smaller clinics.26
Other than cost alone, clinics should consider other factors when deciding whether to implement this testing modality. The convenience of offering self-collected 3-site GC/CT NAAT, combined with the ability to receive same-day results, likely would be preferred by patients and potentially increase access to care allowing greater treatment of GC/CT. A clinic in Los Angeles, CA, offered rapid GC/CT NAAT and immediate treatment to patients and found an increase in same-day treatment for positive test results from 3.6% to 21.1%.27 Rapid NAAT has the potential to increase provision of GC/CT treatment and provide the immediate infrastructure for additional prevention services to interrupt transmission of GC/CT that could also impact transmission and acquisition of HIV.
One of the main limitations of our analysis was a lack of data to inform more robust modeling of downstream transmission pathways. This limitation prevented us from formally evaluating cost-effectiveness against thresholds that use quality-adjusted life years or disability-adjusted life years as metrics.28 More sophisticated analyses informed by data on transmission risk before and after diagnosis could inform more detailed modeling on the number of infections averted and formal economic evaluation. Second, we note that our results are specific to San Diego County and therefore may not necessarily be generalizable to other areas, both in terms of costs and impact. Additional studies examining the cost of and outcomes using rapid NAAT in other settings are warranted. We note that our estimated cost of routine NAAT testing ($18/test) was less than previous studies that have estimated costs of NAAT using insurance claims data or Medicaid reimbursement rates ($39–$65/test),29,30,31 but our estimate was obtained directly from the county HHSA and estimated based on actual provider cost, which would be expected to differ from claims or reimbursement rates. We additionally perform sensitivity analysis examining the impact of volume on cost-effectiveness, but further work examining the impact and costs of rapid NAAT strategies would aid in understanding whether our results translate to other settings.
This study supports the implementation of rapid GC/CT NAAT in clinics serving a large proportion of MSM and TGW patients. This testing modality is more expensive than routine GC/CT NAAT; however, the benefit of increased infectious days averted and probable reduction in onward transmission combined with likely improved health care service quality for patients argue a strong case for implementation.
REFERENCES 1. Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015; 64(Rr-03):1–137. 2. Unemo M, Bradshaw CS, Hocking JS, et al. Sexually transmitted infections: Challenges ahead. Lancet Infect Dis 2017; 17:e235–e279. 3. Tuddenham S, Hamill MM, Ghanem KG. Diagnosis and treatment of sexually transmitted infections: A review. JAMA 2022; 327:161–172. 4. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018. 2019. Available at: https://www.cdc.gov/std/stats18/STDSurveillance2018-full-report.pdf. 5. Whiley DM, Tapsall JW, Sloots TP. Nucleic acid amplification testing for Neisseria gonorrhoeae: An ongoing challenge. J Mol Diagn 2006; 8:3–15. 6. Levett PN, Brandt K, Olenius K, et al. Evaluation of three automated nucleic acid amplification systems for detection of Chlamydia trachomatis and Neisseria gonorrhoeae in first-void urine specimens. J Clin Microbiol 2008; 46:2109–2111. 7. Su WH, Tsou TS, Chen CS, et al. Are we satisfied with the tools for the diagnosis of gonococcal infection in females? J Chin Med Assoc 2011; 74:430–434. 8. Fisk KM, Derouin A, Holm G, et al. Getting it right: The impact of point-of-care testing for gonorrhea and chlamydia in the urgent care setting. J Nurse Pract 2020; 16:388–393. 9. Turner KME, Round J, Horner P, et al. An early evaluation of clinical and economic costs and benefits of implementing point of care NAAT tests for Chlamydia trachomatis and Neisseria gonorrhoea in genitourinary medicine clinics in England. Sex Transm Infect 2014; 90:104–111. 10. Jamison KBS, Rakeman J, Daskalak D, et al. Life in the fast lane: Express STI testing, notification, and treatment at the Chelsea Sexual Health Clinic, 2018–2019. Sex Transm Dis 2020; 47(Suppl 2):S31–S32. 11. Kennedy R, Winter AJ. Reducing time to treatment of bacterial sexually transmitted infections in an HIV cohort. BMJ Open Qual 2020; 9:e000603. 12. Wingrove I, McOwan A, Nwokolo N, et al. Diagnostics within the clinic to test for gonorrhoea and chlamydia reduces the time to treatment: A service evaluation. Sex Transm Infect 2014; 90:474. 13. Mercer CH, Sutcliffe L, Johnson AM, et al. How much do delayed healthcare seeking, delayed care provision, and diversion from primary care contribute to the transmission of STIs? Sex Transm Infect 2007; 83:400–405. 14. Gaydos CA, Ako MC, Lewis M, et al. Use of a rapid diagnostic for Chlamydia trachomatis and Neisseria gonorrhoeae for women in the emergency department can improve clinical management: report of a randomized clinical trial. Ann Emerg Med 2019; 74:36–44. 15. Holley CE, Van Pham T, Mezzadra HM, et al. Overtreatment of gonorrhea and chlamydial infections in 2 inner-city emergency departments. Am J Emerg Med 2015; 33:1265–1268. 16. Sexton J, Garnett G, Røttingen JA. Metaanalysis and metaregression in interpreting study variability in the impact of sexually transmitted diseases on susceptibility to HIV infection. Sex Transm Dis 2005; 32:351–357. 17. Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: The contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999; 75:3–17. 18. Gaydos CA, Van Der Pol B, Jett-Goheen M, et al. Performance of the Cepheid CT/NG Xpert Rapid PCR test for detection of Chlamydia trachomatis and Neisseria gonorrhoeae. J Clin Microbiol 2013; 51:1666–1672. 19. Adamson PC, Loeffelholz MJ, Klausner JD. Point-of-care testing for sexually transmitted infections: A review of recent developments. Arch Pathol Lab Med 2020; 144:1344–1351. 20. Whitlock GG, Gibbons DC, Longford N, et al. Rapid testing and treatment for sexually transmitted infections improve patient care and yield public health benefits. Int J STD AIDS 2018; 29:474–482. 21. Huang W, Gaydos CA, Barnes MR, et al. Comparative effectiveness of a rapid point-of-care test for detection of Chlamydia trachomatis among women in a clinical setting. Sex Transm Infect 2013; 89:108–114. 22. Rivard KR, Dumkow LE, Draper HM, et al. Impact of rapid diagnostic testing for chlamydia and gonorrhea on appropriate antimicrobial utilization in the emergency department. Diagn Microbiol Infect Dis 2017; 87:175–179. 23. Frick KD. Microcosting quantity data collection methods. Med Care 2009; 47(7 Suppl 1):S76–S81. 24. Vassall A, Sweeney S, Kahn J, et al. Reference case for estimating the costs of global health services and interventions. 2017. Global Health Cost Consortium. Available at: https://ghcosting.org/pages/standards/reference_case. Accessed April 29, 2024. 25. Kumar S, Chesson H, Gift TL. Estimating the direct medical costs and productivity loss of outpatient chlamydia and gonorrhea treatment. Sex Transm Dis 2021; 48:e18–e21. 26. Balendra A, Cousins E, Lamplough H, et al. Pilot study for the ‘Test n Treat’ trial of on-site rapid chlamydia/gonorrhoea tests and same day treatment. Sex Transm Infect 2017; 93:283. 27. Keizur EM, Goldbeck C, Vavala G, et al. Safety and effectiveness of same-day Chlamydia trachomatis and Neisseria gonorrhoeae screening and treatment among gay, bisexual, transgender, and homeless youth in Los Angeles, California, and New Orleans, Louisiana. Sex Transm Dis 2020; 47:19–23. 28. Vanness DJ, Lomas J, Ahn H. A health opportunity cost threshold for cost-effectiveness analysis in the United States. Ann Intern Med 2021; 174:25–32. 29. Owusu-Edusei KJ, Nguyen HT, Gift TL. Utilization and cost of diagnostic methods for sexually transmitted infection screening among insured American youth, 2008. Sex Transm Dis 2013; 40:354–361. 30. Ditkowsky J, Shah KH, Hammerschlag MR, et al. Cost-benefit analysis of Chlamydia trachomatis screening in pregnant women in a high burden setting in the United States. BMC Infect Dis 2017; 17:155. 31. Rönn MM, Li Y, Gift TL, et al. Costs, Health Benefits, and Cost-Effectiveness of Chlamydia Screening and Partner Notification in the United States, 2000–2019: A Mathematical Modeling Analysis. Sex Transm Dis 2023;50:351–358.For further references, please see “Supplemental References,” https://links.lww.com/OLQ/B75.
留言 (0)