
記住我
Aeromonas spp. are gram-negative anaerobic rods primarily found in water. Respiratory infections with Aeromonas spp. are rare, but the mortality rate is high.1-3 We encountered a patient with septic shock due to infection with Aeromonas caviae, which he contracted during a near-drowning accident in river water. In such cases, combination therapy should be considered when previously treatment with antimicrobial agents do not provide sufficient improvement.
CASE REPORTA 43-year-old man fell into river water following an automobile accident. He was immediately rescued and intubated orally by a physician at Yokohama Work Station Doctor Car (http://www-user.yokohama-cu.ac.jp/~er-urahp/WS_doctor_car.html), and transported to our hospital with airway and ventilator management. He was previously in good health, with no medical history prior to the day of the accident.
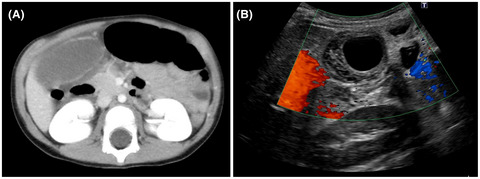
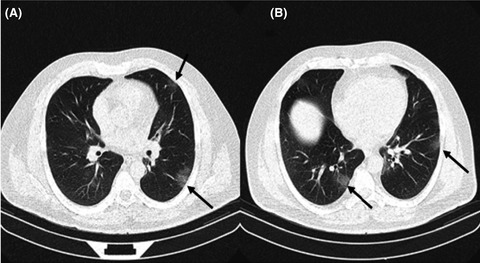
On admission, he was comatose, hypothermic, and in respiratory failure. His consciousness was assessed as E1VtM1 based on the Glasgow Coma Scale. His pulse rate was 91 b.p.m., with a blood pressure of 147/83 mmHg and a body temperature of 35°C. Physical examination revealed no evidence of trauma. Coarse crackles were noted throughout the lung field. His plain chest radiographs showed decreased permeability in all the lung fields (Fig. 1). Chest computed tomography showed consolidation in both lower lobes (Fig. 1). Arterial blood gas findings on a 100% fraction of inspired oxygen (FiO2) under volume control ventilation (positive end-expiratory pressure, 0.49 kPa; tidal volume, 480 ml; respiratory rate, 15/min) were as follows: pH, 6.678; partial pressure of oxygen (PaO2), 253.1 mmHg; partial pressure of carbon dioxide, 139.3 mmHg; calculated bicarbonate concentration, 16.0 mmol/L; base excess/deficit, −24.4 mmol/L; and lactate dehydrogenase, 13.71 mmol/L. The PaO2 / FiO2 ratio was 253. The patient’s laboratory findings are shown in Table 1. The Sequential Organ Failure Assessment score was 18 points. Using diagnostic criteria for disseminated intravascular coagulation established by the Japanese Association for Acute Medicine, he had a score of 4 points.

Plain chest radiography and chest computed tomography on days 1, 28, and 59 of admission of a 43-year-old man with severe respiratory infection due to Aeromonas caviae.
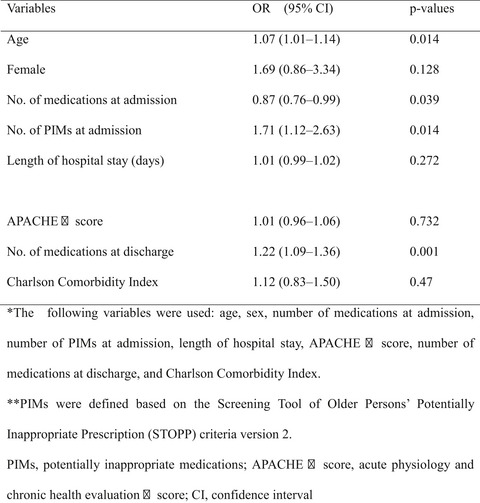
Table 1. Laboratory findings on admission of a 43-year-old man with severe respiratory infection due to Aeromonas caviae WBC 9,640/mm3 Hgb 16.3 mg/dl Hct 52.3% PLT 19.2 × 104/µl BUN 19.1 mg/dl Cre 1.27 mg/dl Total bilirubin 0.5 mg/dl AST 105 IU/L ALT 39 IU/L LDH 1268 IU/L CRP <0.04 mg/dl APTT 89.9 s PT-INR 1.87 Fibrinogen 182 mg/dl D-dimer 97.1 µg/ml Abbreviations: ALT, alanine aminotransferase; APTT, activated partial thromboplastin time; AST, aspartate aminotransferase; BUN, blood urea nitrogen; Cre, serum creatinine; CRP, C-reactive protein; Hct, hematocrit; Hgb, hemoglobin; LDH, lactate dehydrogenase; PLT, platelets; PT-INR, prothrombin time-international normalized ratio; WBC, white blood cell.The patient was initially treated with ampicillin/sulbactam (ABPC/SBT), volume expansion, vasopressors (noradrenaline and dobutamine), and glucocorticoids. However, he immediately developed septic shock, disseminated intravascular coagulation, and acute kidney injury. He became anuric and was diagnosed with stage 3 acute kidney injury, according to the Kidney Disease Improving Global Outcomes criteria. Continuous renal replacement therapy was then initiated.
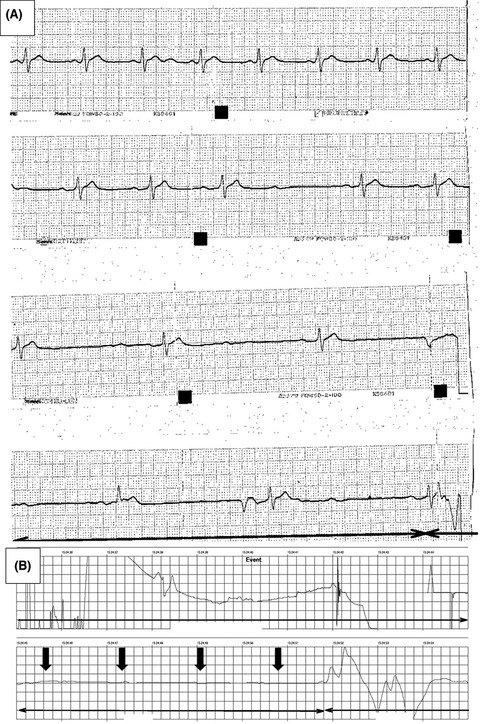
Acute respiratory distress syndrome (ARDS) was diagnosed based on the Berlin criteria (PaO2 / FiO2, <100) on day 2 of hospitalization. Prone position therapy was initiated (>12 h), and the patient was ventilated using the airway pressure release ventilation method. On day 7, Aeromonas caviae was detected in his blood and sputum cultures. The antimicrobial regimen was switched from ABPC/SBT to tazobactam/piperacillin (TAZ/PIPC), as susceptibility tests indicated resistance to the former and susceptibility to the latter (minimum inhibitory concentration [MIC] ≤ 8 µg/ml). On day 9, levofloxacin (LVFX; MIC ≤ 1 µg/ml) was given based on previous recommendations.4 However, on day 13, A. caviae was again detected in his blood culture. On day 20, the antimicrobial regimen was switched from TAZ/PIPC to meropenem (MEPM; MIC ≤ 1 µg/ml), and his condition improved. On day 26, however, MEPM was discontinued due to the appearance of a drug rash. By day 36, LVFX alone had failed to control the infection, with A. caviae growing in blood cultures. On day 39, cefepime (CFPM; MIC ≤ 1 µg/ml) with LVFX improved the inflammatory response. On day 43, his blood culture tested negative, and his fever was alleviated. By day 45, the patient’s C-reactive protein level had decreased to below the normal level. Cefepime was discontinued on day 51, with no observable worsening of symptoms (Fig. 2). On day 34, a tracheostomy was carried out for long-term ventilator management, from which he was weaned on day 43 and transferred to a rehabilitation hospital on day 60.

Clinical course of a 43-year-old man with severe respiratory infection due to Aeromonas caviae. ABPC/SBT, ampicillin/sulbactam; APRV, airway pressure release ventilation; CFPM, cefepime; CRP, C-reactive protein; CRRT, continuous renal replacement therapy; LVFX, levofloxacin; MEPM, meropenem; P/F, PaO2/FiO2; TAZ/PIPC, tazobactam/piperacillin; WBC, white blood cell. Black arrow, positive blood culture; white arrow, negative blood culture.
DISCUSSIONAeromonas spp. are gram-negative rods that are widely distributed in fresh water. Diarrheal disease is the most common manifestation of infection due to Aeromonas spp.,4 which has also been associated with several extraintestinal manifestations. The organisms are implicated in osteomyelitis, meningitis, respiratory infections, pelvic abscesses, and peritonitis. Sepsis occurs in older adult patients with hematologic malignancies, severe hepatobiliary disease, certain immunocompromised conditions, or trauma.5, 6 Respiratory infections due to Aeromonas sp. are rare. A rapid worsening of the disease and a high mortality rate in healthy patients infected with Aeromonas sp. has been reported in near-drowning incidents.2
We initially administered ABPC/SBT, used to treat aspiration pneumonia, as we suspected that the main cause of ARDS was due to water aspiration. However, A. caviae was later detected in his blood and sputum cultures. Most Aeromonas sp. are resistant to penicillin, ampicillin, carbenicillin, and ticarcillin but susceptible to fluoroquinolones, third- and fourth-generation cephalosporins, aminoglycosides, carbapenems, chloramphenicol, and tetracyclines.4 Furthermore, TAZ/PIPC was selected based on susceptibility testing. However, as the patient’s condition failed to improve, LVFX was introduced based on a previous report4 and the susceptibility test results. Aeromonas caviae is susceptible to LVFX, but there are reports of infections associated with fluoroquinolone resistance.7, 8 In our patient, LVFX was only partially effective against A. caviae; therefore, we included MEPM, which was later discontinued due to the appearance of a drug rash. The blood cultures finally tested negative after treatment with CFPM plus LVFX. The use of combination antimicrobial therapy for severe respiratory tract infections due to Aeromonas sp. has not previously been reported. Treatment with LVFX alone was ineffective in producing negative blood cultures, a temperature 37°C or less, or decreasing C-reactive protein levels, whereas the addition of CFPM led to more positive results. Therefore, combination therapy should be considered for patients who do not improve sufficiently with previously administered antimicrobials.
We note that treatment an antimicrobial regimen comprising ABPC/SBT, customarily used to treat aspiration pneumonia, for several days was ineffective in achieving any significant improvement in his septic shock status due to infection with A. caviae. Therefore, due to the high mortality risk of Aeromonas sp.-related respiratory infections,1-3 fluoroquinolones and carbapenems should be started early if a near-drowning incident is suspected. Moreover, in severe respiratory infections due to Aeromonas sp., antimicrobial agents should be switched or combined if there is no improvement, even if the susceptibility testing is favorable.
CONCLUSIONSWe encountered a patient with severe respiratory infection and ARDS due to A. caviae after a near-drowning accident in river water. We recommend that when patients develop a respiratory infection from aspiration of river water, empiric antimicrobial therapy should be immediately given to manage Aeromonas sp. infection.
ACKNOWLEDGMENTSWe thank Editage for English language editing.
DisclosureApproval of the research protocol: N/A.
Informed consent: Informed consent was obtained from the patient to publish this case report and any accompanying images.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflicts of interest: None.
REFERENCES
1Nagata K, Takeshima Y, Tomii K, Imai Y. Fulminant fatal bacteremic pneumonia due to Aeromonas hydrophila in a non-immunocompromised woman. Intern. Med. 2011; 50: 63– 5. 2Miyake M, Iga K, Izumi C, Miyagawa A, Kobashi Y, Konishi T. Rapidly progressive pneumonia due to Aeromonas hydrophila shortly after near-drowning. Intern. Med. 2000; 39: 1128– 30. 3Ishida T, Miyazaki K, Hikone M, Sugiyama K, Tanabe T, Hamabe Y. Successful support by veno-arterial extracorporeal membrane oxygenation for severe septic shock caused by Aeromonas hydrophila. Acute Med. Surg. 2019; 6: 305– 7. 4Aravena-Román M, Inglis TJJ, Henderson B, Riley TV, Chang BJ. Antimicrobial susceptibilities of Aeromonas strains isolated from clinical and environmental sources to 26 antimicrobial agents. Antimicrob. Agents Chemother. 2012; 56: 1110– 2. 5Honda M, Okamura H, Inoue T, Maekawa T. A case of surviving the fulminant form of Aeromonas hydrophilia pneumoniae due to aspiration of river water (in Japanese). JJAAM 2014; 25: 717– 22. 6Parker JL, Shaw JG. Aeromonas spp. clinical microbiology and disease. J. Infect. 2011; 62: 109– 18. 7Patel KM, Svestka M, Sinkin J, Ruff P 4th. Ciprofloxacin-resistant Aeromonas hydrophila infection following leech therapy: a case report and review of the literature. J. Plast. Reconstr. Aesthet. Surg. 2013; 66: e20– 2. 8Alcaide E, Blasco MD, Esteve C. Mechanisms of quinolone resistance in Aeromonas species isolated from humans, water, and eels. Res. Microbiol. 2010; 161: 40– 5.
留言 (0)