
記住我

Patients with tuberous sclerosis complex (TSC) have varied pulmonary manifestations ranging from the most common lymphangioleiomyomatosis (LAM) to the lesser known multifocal micronodular pneumocyte hyperplasia (MMPH).1 TSC is an autosomal dominant disorder caused by loss-of-function mutations in TSC1 or TSC2 genes on chromosome 9q34 or 16p13, respectively.2 TSC remains a rare disease with an incidence of 1:6000.3 Patients with TSC have multi-systemic involvement, with skin manifestations (Shagreen patch, ungual fibromas and hypomelanotic macules) being the most common.4
MMPH presents radiologically as diffuse small solid and ground-glass nodules in a random distribution. The radiological differentials range from infectious to malignant conditions where there is no pathognomonic feature for either. Obtaining an accurate diagnosis is hence a challenge but yet paramount in ensuring appropriate care is delivered. Here, we describe the features of MMPH in a patient with TSC who has co-existing LAM and MMPH.
CASE REPORTA 50-year-old Chinese female presented with a 1-week history of dyspnoea and cough. There was no associated chest pain, fever or haemoptysis. Systemic review was negative for loss of weight or appetite. She is a non-smoker with no family history of lung diseases. Her only other past medical history is Graves' disease.
Physical examination revealed a slim female with a body mass index of 17 kg/m2. She was mildly tachypnoeic with a blood pressure of 172/102 mmHg, heart rate of 97 beats per minute and oxygen saturation of 95% on room air. Examination of the chest was remarkable for reduced air-entry on the right. Cardiac and abdominal examination were normal. There was no digital clubbing or cervical lymphadenopathy. Of note, there were bilateral small erythematous papules on her cheeks and nasolabial folds.
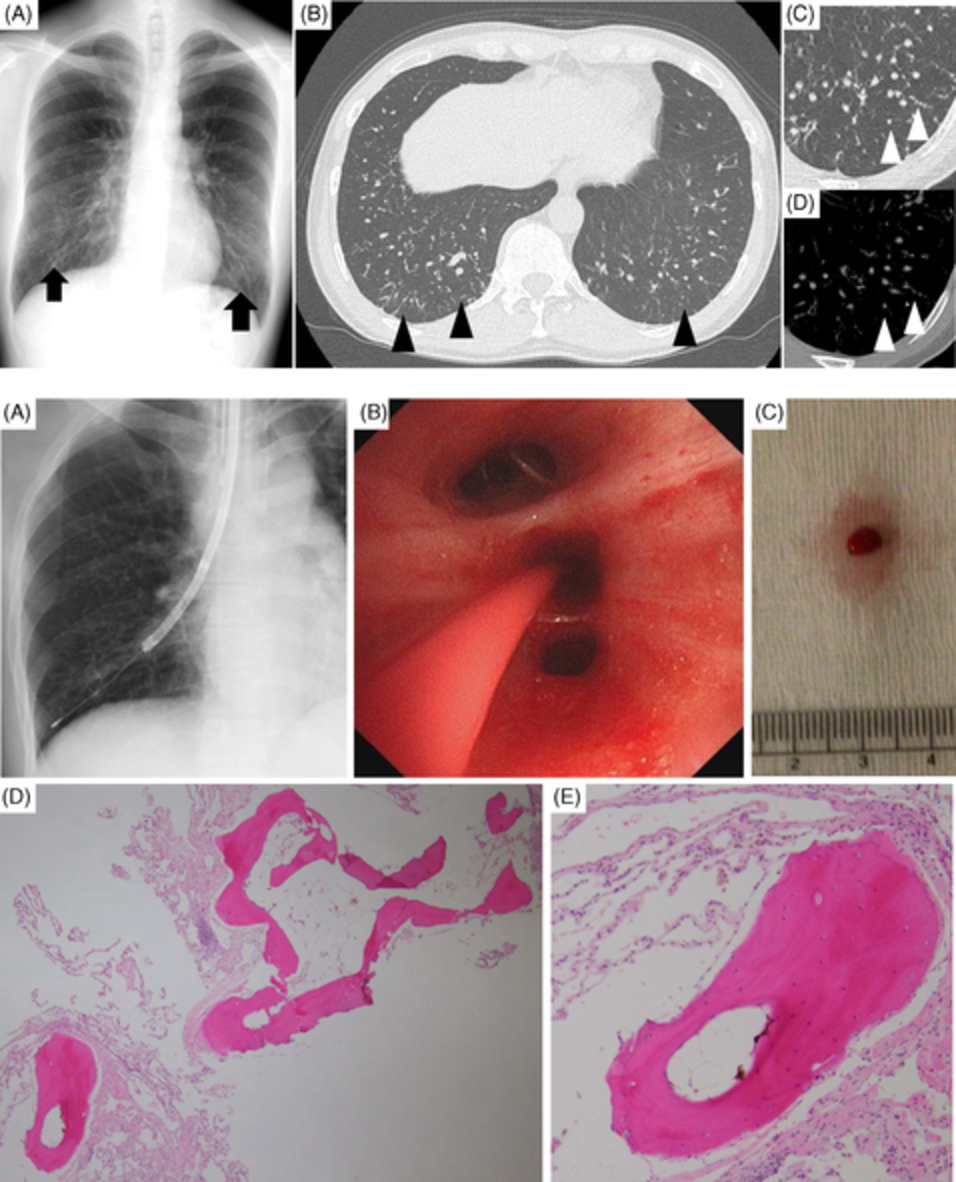
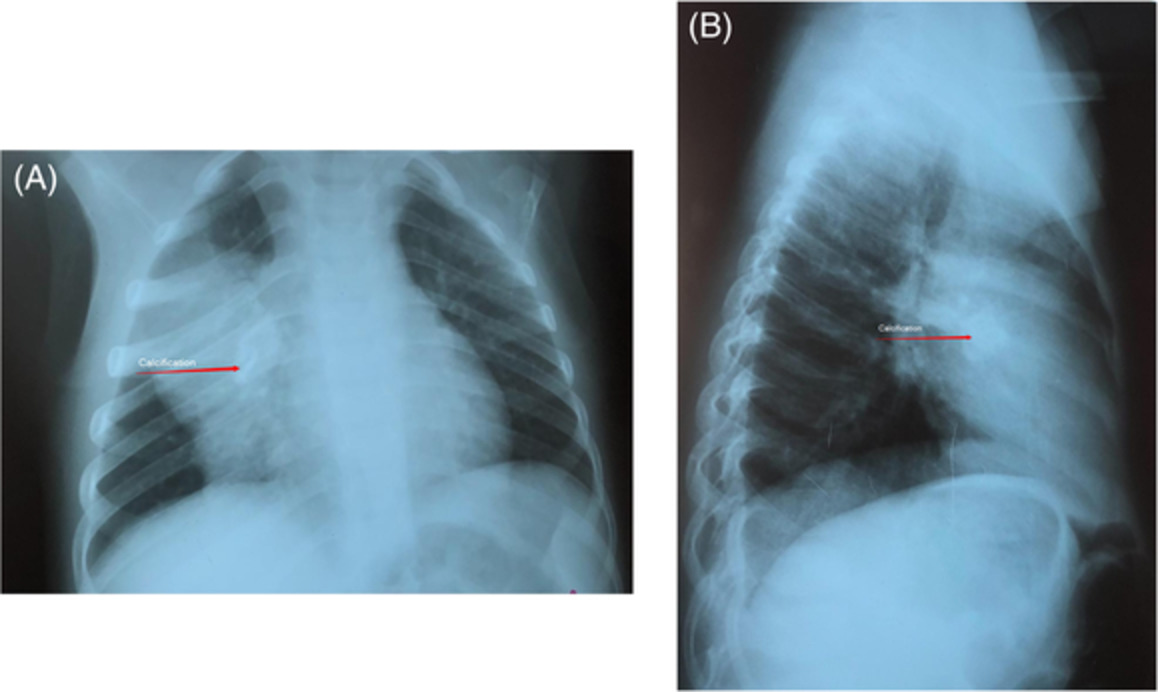
Chest radiograph (Figure 1) showed a large right pneumothorax with no mediastinal shift or tracheal deviation. Diffuse reticular-nodular opacities were noted in the left lung. Laboratory results were unremarkable.

Chest radiograph showing a large right hydropneumothorax with no mediastinal shift or tracheal deviation. Diffuse reticular-nodular opacities are noted in the aerated left lung
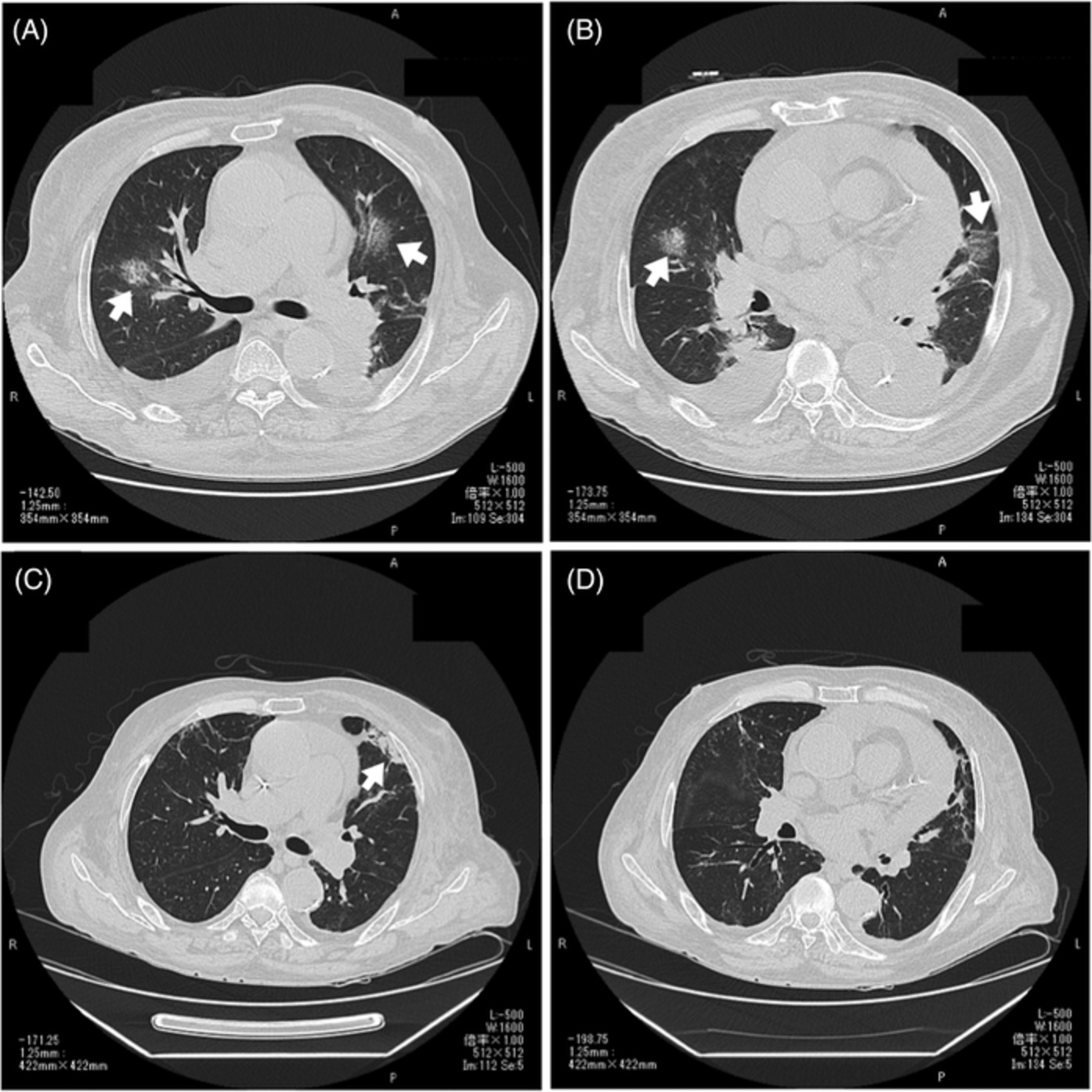
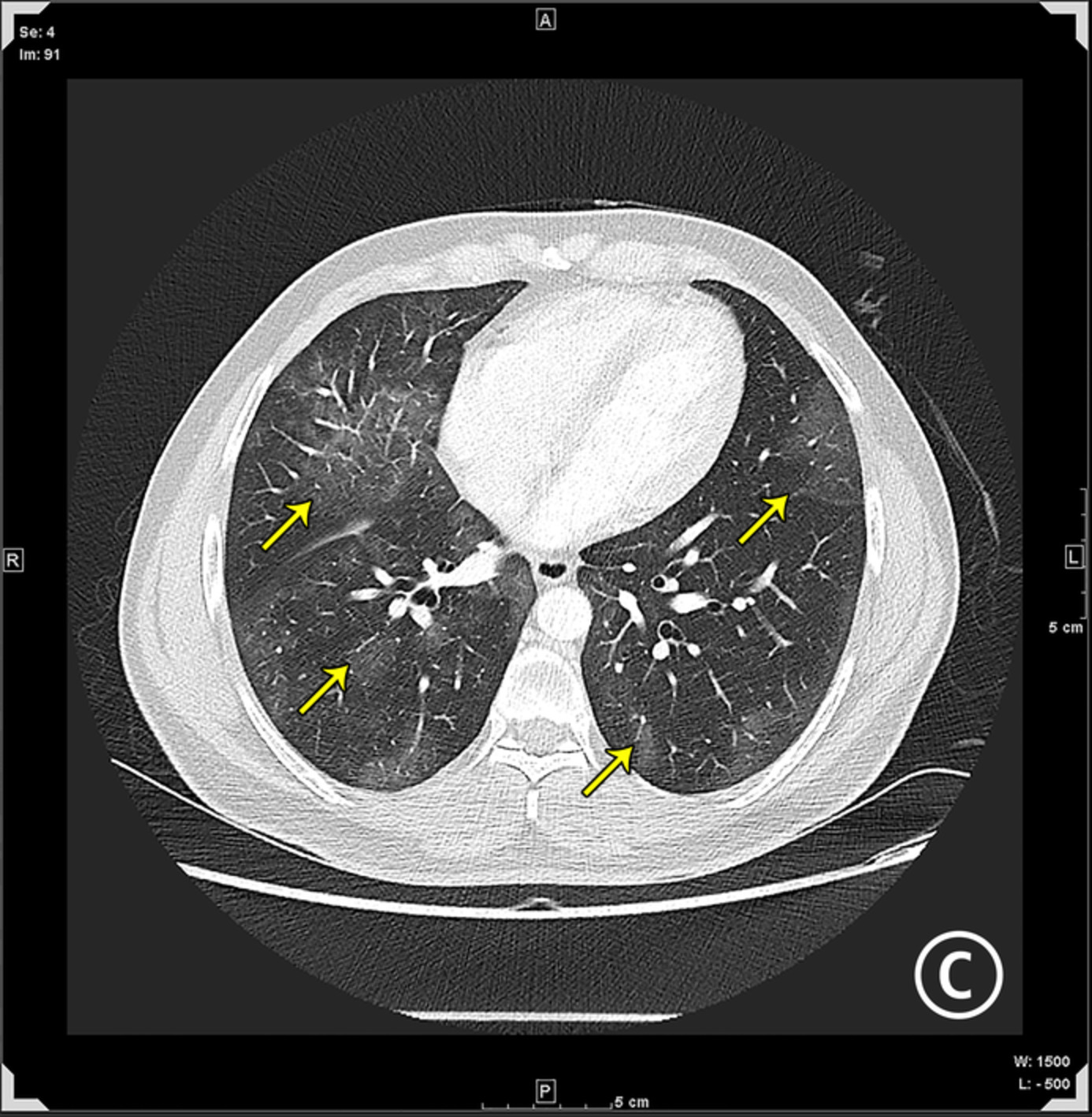
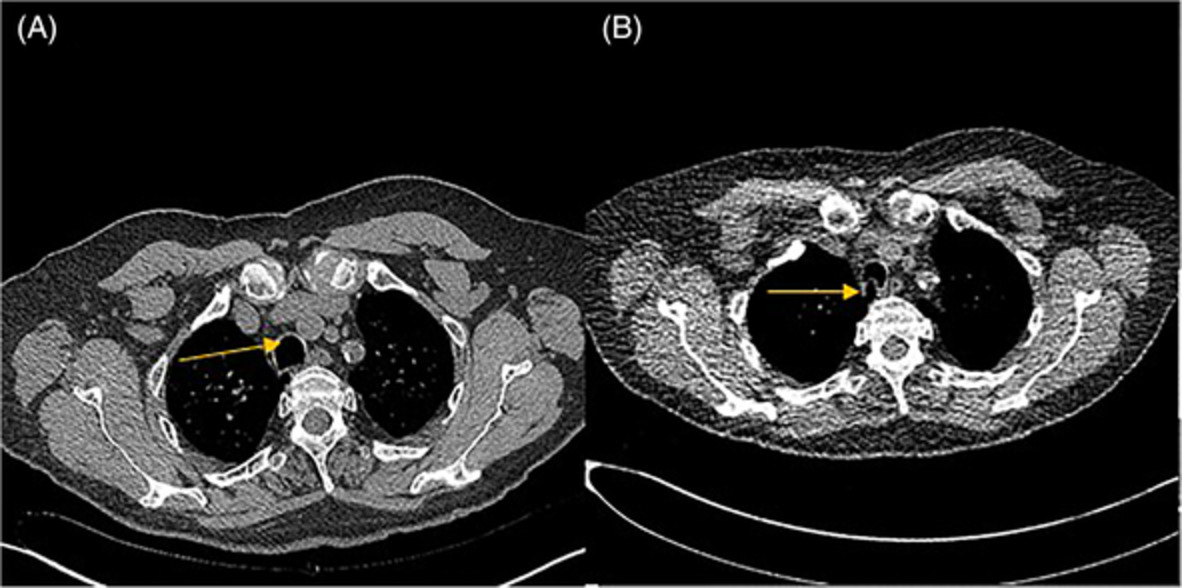
A chest tube was inserted into the right pleural cavity with re-expansion of the right lung. Her symptoms resolved and the chest tube was removed after the pneumothorax resolved. A high-resolution computed tomography (CT) scan (Figure 2A,B) revealed multiple round thin-walled cysts with multiple tiny (<4 mm) ground-glass and solid nodules. Visualized sections of the kidney also showed multiple fat density lesions (Figure 2C,D) consistent with renal angiomyolipomas.

(A, B) High-resolution computed tomography (CT) scan of the thorax showing multiple round thin-walled cysts (yellow arrows with yellow outline) with mild interlobular septal thickening and tiny (<4 mm) ground-glass and solid nodules (red arrows with red outline) in the axial and coronal plane, respectively. (B) Right pneumothorax is noted (white arrow with red outline). (C, D) CT scan showing multiple fat density lesions (white arrows with white outline) in bilateral kidneys in the axial and coronal plane
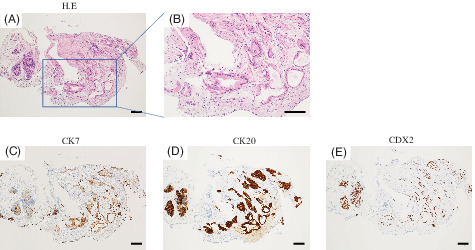
Unfortunately, she re-presented with a recurrence of the right pneumothorax a week later and underwent video-assisted thoracoscopy (VATS) with lung biopsy and pleurodesis. Intraoperative findings (Figure 3) revealed a spongy lung with small cysts on the surface. Histological analysis (Figure 4A–D) showed a multi-cystic appearance with foci of spindle cell proliferation which were positive on immunohistochemistry for human melanoma black-45 (HMB-45), smooth muscle actin (SMA) and estrogen receptor (ER), confirming the diagnosis of LAM. The presence of several nodular proliferations of type II pneumocytes along thickened septa raised the diagnosis of co-existing MMPH (Figure 4G). These pneumocytes had mildly enlarged nuclei, but with preservation of normal nuclear to cytoplasmic ratios, and were accompanied by occasional aggregates of intra-alveolar macrophages (Figure 4H). Ziehl–Neelsen stain for acid-fast bacilli (AFB) was negative and there was no evidence of caseating granulomas on histology.

Video-assisted thoracoscopy intraoperative image showing subpleural cysts on the fissural surface of the right upper lobe with dense adhesions

Histological appearance of the wedge resection of the lung, with multiple subpleural cysts at low power (A, 10×) and medium power (B, 100×). A close-up of the wall of one of the cysts (C, 200×) shows a spindle cell proliferation, which on immunohistochemistry is positive for HMB-45 (D), SMA (E) and ER (F). Medium-power view (G, 100×) showing a nodule with type II pneumocyte proliferation and thickening of the interstitium. At higher magnification (H, 400×), the pneumocytes demonstrate at most mild nuclear atypia but with preserved nuclear to cytoplasmic ratios. An aggregate of macrophages is noted within the alveolar space
Pulmonary function test performed after pleurodesis revealed a restrictive defect and moderately reduced diffusing capacity for carbon monoxide (DLCO) (Forced expiratory volume in 1 s/Forced vital capacity [FEV1/FVC]: 86%, FEV1: 71%, FVC: 62%, total lung capacity: 84%, DLCO: 58%). Genetic screening for TSC resulted positive for TSC2 mutation, confirming the diagnosis of MMPH co-existing with LAM in a patient with TSC. Further CT imaging of the brain revealed multiple subependymal lesions, patchy bony sclerosis and multiple cutaneous skin lesions on the scalp compatible with stigmata of TSC. Our patient was started on sirolimus for LAM with stabilization of her lung function.
DISCUSSIONMMPH differs from LAM in terms of its underlying epidemiology, radiology, pathology and prognosis.3 Unlike LAM which has a predilection for females, MMPH has an equal presentation in both genders and a prevalence of 40%–60% in patients with TSC.3, 5 Incidence of MMPH is more common in patients with TSC LAM versus sporadic LAM.3 Concomitant MMPH and LAM in patients with TSC have been described in literature with an incidence of 20%–31%.5-7
Radiologically, MMPH appears as multicentric diffuse and discrete small (2–14 mm) solid and ground-glass nodules with a random distribution.3, 8, 9 There have been no reported pathognomonic imaging feature of MMPH. Radiological differentials of MMPH include miliary tuberculosis (TB), atypical adenomatous hyperplasia (AAH), adenocarcinoma in situ (AIS) and pulmonary Langerhans cell histiocytosis (PLCH).8 Misdiagnosis of MMPH as miliary TB has been described as clinical differentiation is difficult.10, 11 Sputum AFB smears and cultures are typically negative in miliary TB due to its predominant haematogenous involvement. Therefore, the histological absence of caseating granulomas coupled with a negative Ziehl–Neelsen stain is important in excluding the diagnosis of miliary TB, especially due to its public health implications. Radiological stability over time and multicentric disease at onset favour MMPH over AAH/AIS.12, 13 Early-stage PLCH tends to have irregular and bizarre shaped cysts with sparring of the lung bases and costophrenic angles, whereas the cysts in LAM are diffuse, round and uniform with thin walls.14 Associated features of TSC such as LAM, renal angiomyolipomas and tuberous adenomas can help to clinch the diagnosis of MMPH.
Histologically, MMPH is distinct from the smooth muscle proliferation in LAM. MMPH is characterized by benign hamartomatous and nodular proliferation of type II pneumocytes along the alveolar septa with fibrous thickening.15, 16 These type II pneumocytes have preserved nuclear to cytoplasmic ratio and is often seen with focal aggregates of alveolar macrophages.13 In contrast, LAM has been described as a progressive disease of lung ‘metastases’ of LAM cells, where they secrete enzymes leading to matrix destruction and cyst formation.3
The presence of MMPH has not been shown to affect pulmonary function and it has been described as a benign disease in the current literature.6, 8, 12, 13, 17 Patients with MMPH are usually asymptomatic and it is largely diagnosed only upon presentation of the other manifestations of TSC.18 This is distinct from LAM which is a progressive symptomatic disease.3 MMPH itself does not require treatment due to its benign nature, but patients with concomitant LAM will benefit from mammalian target of rapamycin (mTOR) therapy.3
In our patient, the cystic changes of diffuse and uniform thin-walled cysts with the presence of renal angiomyolipomas are compatible with a clinical diagnosis of LAM.3, 14 However, the concomitant finding of multiple tiny ground-glass and solid nodules suggests the presence of another pathology. Our patient underwent VATS pleurodesis for definitive treatment of her secondary pneumothorax and an opportunistic lung biopsy was performed. Histological examination enabled us to confirm the diagnosis of co-existing MMPH and LAM as there was spindle cell proliferation with positive HMB-45, SMA and ER staining on immunohistochemistry (confirming the diagnosis of LAM) and presence of nodular proliferations of type II pneumocytes along thickened septa (confirming the diagnosis of MMPH) (Figure 4). Other differentials such as miliary TB and AAH/AIS were excluded as described above.
Here, we highlight the need for a high degree of suspicion coupled with the constellation of radiological and histological findings to clinch the diagnosis of LAM co-existing with MMPH in a patient with TSC.
AUTHOR CONTRIBUTIONDr Li Yan Sandra Hui obtained clinical data and conceptualized, designed and wrote the original draft. Dr Xin Min Cheng, Dr Ing Xiang Soo and Dr Su Ying Low obtained clinical data and conceptualized and revised the manuscript. All authors approved the final version of the manuscript.
ETHICS STATEMENTThe authors declare that appropriate written informed consent was obtained for the publication of this case report and accompanying images.
留言 (0)