
記住我
Angioedema is a nondependent, nonpitting edema that can involve the airway and is potentially life-threatening. It is a relatively uncommon chief concern in the emergency department (ED),1-4 with an estimated 117,000 ED visits annually3 and up to 30% of patients with angioedema utilizing the ED at least once in their lifetime.4 Angioedema can present from multiple etiologies with a variety of symptoms and can result in outcomes ranging from mild swelling to death.4-8 The fatality associated with angioedema is due to airway obstruction,6-9 which can present rapidly,6-9 making the prompt diagnosis and treatment of these patients by the emergency provider critical.6-9 Thus, tools to aid in the risk assessment and management would be of considerable importance.
One such tool, described by Ishoo et␣al.9 in 1999, reported a staging system based on the anatomic site of angioedema that correlated with patient disposition and need for airway intervention. However, this staging system has not been externally validated in the era of targeted pharmacological therapy. Validation in the contemporary ED setting is required before it can assist in guiding future management strategy,6-8 including in expedited airway intervention, appropriate disposition,6-8 and selection of pharmacologic treatment ranging from conventional options such as antihistamines, steroids, epinephrine to newer targeted agents.10-13 Establishment of such validity can assist emergency medicine providers in assessing risk for airway compromise and tailoring management and disposition for patients with angioedema to achieve optimal outcomes.
In this study, we aim to evaluate the predictive value of the Ishoo staging system in the modern era ED as a method of predicting the potential for airway compromise.
METHODS DesignThis study is a retrospective chart review of ED patients of all ages with angioedema that presented to an academic ED between August 1, 2006, and January 31, 2018. The institutional review board deemed this study as a minimal risk and waived a consent.
SettingThe study site is a tertiary academic care facility and statewide referral center with an annual census of 60,000. The facility has access to board-certified allergy immunologists, otolaryngologists, critical care services, and ED pharmacists. Targeted pharmaceutical agents for angioedema became available in our institution in 2009.
VariablesData on the following variables were collected during the presentation of angioedema: patient demographics, anatomical site of swelling while in the ED, symptoms at presentation, suspected etiology of angioedema if one could be identified, comorbidities, treatment setting (prehospital vs hospital), pharmacological management, airway evaluation and interventions if performed, patient disposition, and in-hospital mortality.
Data sourcesWe extracted charts from the electronic medical record system if the patient had an ED encounter with a primary diagnosis of angioedema, using the ICD9 diagnosis of 995.1 and ICD10 diagnosis of T78.3XXA. Then, we reviewed the records and collected data from the beginning of the ED visit through discharge from the hospital and entered into the electronic data collection form. Each ED visit with an associated diagnosis of angioedema for a given patient was entered separately.
Staging criteria and outcomesOur staging system was based on the stages previously described by Ishoo et␣al.9 with minor modifications due to a retrospective study design (Fig. 1). Stage 1 included angioedema of the lips and face (including periorbital region) similar to the Ishoo et␣al.’s study; however, we also included extremity and total body/diffuse swelling in stage 1 and did not include facial rash. Stage 2 included angioedema localized to the soft palate consistent with the previously described stage 2; however, we also included posterior pharynx (not including the tongue). Also consistent with the previously described staging system, stage 3 included tongue angioedema and stage 4 included laryngeal edema. Patients with angioedema localizing to more than one stage were categorized into the higher stage. Outcomes of interest included disposition (discharge, floor, intensive care unit [ICU]) and airway intervention (endotracheal intubation, cricothyrotomy, or tracheotomy). The study location did not have an ED observation unit. The disposition of discharge was based on the ED provider’s stability assessment. When the ED provider did not think the patient was not stable, the disposition was admission to the inpatient floor. When a patient required a close airway monitoring or airway intervention such as endotracheal intubation, the ED provider transferred the patient to ICU. The author (SL) verified the disposition of all patients in the EMR.
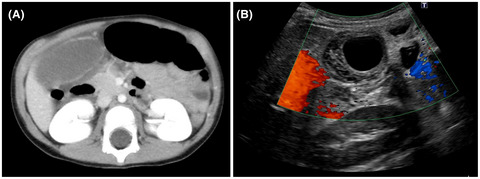
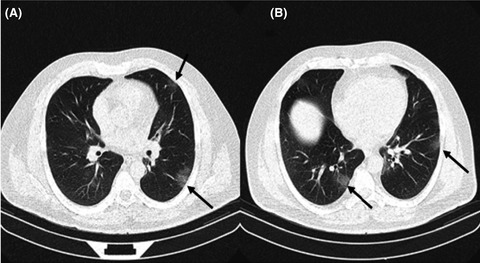
 Presentation of angioedema in the emergency department. (A) Facial/lip edema (Ishoo stage I). (B) Palatal edema (Ishoo stage II). A and B obtained from www.haeimages.com.
Bias
Presentation of angioedema in the emergency department. (A) Facial/lip edema (Ishoo stage I). (B) Palatal edema (Ishoo stage II). A and B obtained from www.haeimages.com.
Bias
Informational bias was minimized by the principal investigator reviewing the first 20 records with the reviewers (MM and CD) and standardizing the data extraction and interpretation. We discussed any difficult cases (about 10%) by email and in-person meetings throughout the study period. Each reviewer completed a review of assigned patients.
Statistical methodsThe demographic information was summarized using descriptive statistics. We set the predictor variables, outcomes as four categories (discharge, inpatient admission, ICU admission, and airway intervention), and performed logit analysis to measure the probability of outcomes based on the predictors.
RESULTS Demographic dataDuring the study period, there were 328 patients who had an ED primary diagnosis of angioedema. Of those, 320 were included in this study (Fig. 2). The median patient age was 44 years (interquartile range 28–58) and 54.4% were female. Etiology of the angioedema was attributed to angiotensin-converting enzyme inhibitors in 100 cases (31.3%), histamine-mediated angioedema in 92 (28.8%), hereditary angioedema in 5 (1.6%), and acquired angioedema in 1 case (0.3%). No etiology was identified in 122 cases (38.1%) (Table 1).

Flow chart of the study. DRESS, drug reaction with eosinophilia and systemic symptoms; ED, emergency department.
Table 1. Patient characteristics and clinical features Patient characteristics Values Median age (years), IQR (range) 44 (28–58, 0–94) Female, n (%) 174 (54.4) Comorbidities, n (%) Respiratory disease (asthma, COPD) 55 (17.2) Diabetes 51 (15.9) Cardiovascular disease (ACS, CHF, cardiomyopathy, arrhythmia) 46 (14.4) Autoimmune disease 22 (6.9) Cancer (active and old) 19 (5.9) Clinical features, n (%) Etiology ACE inhibitors 100 (31.3) Histamine mediated 92 (28.8) Hereditary angioedema 5 (1.6) Acquired angioedema 1 (0.3) Unknown 122 (38.1) Signs and symptoms Odynophagia 86 (26.9) Pruritus 74 (23.1) Hives 66 (20.6) Dyspnea 52 (16.3) Voice change 42 (13.1) Stridor/Wheeze 13 (4.1) Flushing 10 (3.1) Hoarseness 10 (3.1) Diarrhea 5 (1.6) Stridor 5 (1.6) Hypotension/Syncope 4 (1.3) Hypoxemia 4 (1.3) Vomiting 4 (1.3) Nausea 3 (0.9) Swelling location Lip 192 (60.0) Tongue 105 (32.8) Face 85 (26.6) Periorbital 48 (15.0) Extremities 30 (9.4) Uvula 24 (7.5) Posterior pharynx 20 (6.3) Soft palate 14 (4.4) Larynx 4 (1.3) Total body/diffuse swelling 4 (1.3) ACE, angiotensin-converting enzyme; ACS, acute coronary syndrome; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; IQR, interquartile range.The most common presenting signs and symptoms were odynophagia (n = 86, 26.9%), pruritus (n = 74, 23.1%), hives (n = 66, 20.6), and dyspnea (n = 52, 16.3%). Other airway complaints were less common, with 42 (13.1%) reporting voice changes, 13 (4.1%) stridor or wheeze, and 10 (3.1%) hoarseness (Table 1). The anatomic location of edema also varied among patients (Table 1), with the specific sites being used to classify patients into one of four stages (Table 2).
Table 2. Staging by site Stage Site Value, n (%) I Lip, face, periorbital, extremities, total body/diffuse swelling 188 (58.8) II Soft palate, posterior pharynx 25 (7.8) III Tongue 103 (32.2) IV Larynx 4 (1.25) ED, emergency department; ICU, intensive care unit. Outcome dataA total of 44 patients had airway evaluation by fiberoptic or video laryngoscopy in the ED. Almost all patients received some type of medical management (n = 313; 97.8%), while only 20 required airway intervention: 18 (5.6%) by intubation and 2 (0.6%) by tracheotomy. Medications used include 285 (89.1%) instances of H1 antagonist, 174 (54.4%) of H2 antagonist, 253 (79.1%) of corticosteroids, 124 (38.8%) of epinephrine, and 6 (1.9%) of biological agents (recombinant C1 esterase inhibitor and bradykinin receptor antagonist). Five (1.6%) patients received fresh frozen plasma. There were no patient deaths during the recorded ED or in-hospital encounter.
Main analysisMost cases were treated in the ED and discharged (n = 219, 68.4%), although 52 patients (16.3%) were admitted to a non-ICU floor, and 49 patients (15.3%) were admitted to the ICU. Next, we estimated the probability of each disposition based on the stage. When disposition was correlated, patients in stage 1 were more likely to be treated in the ED and discharged (probability 85%) compared with requiring ICU care without (2.5%) and with (0.1%) airway intervention. These 4 cases had concomitant conditions (sepsis, postoperative complication, stroke status post-tissue plasminogen activator, and subsequent deterioration after hospitalization) that required ICU admission. Conversely, patients in stage 4 were more likely to require ICU care without (17%) and with (67%) airway intervention compared with being treated in the ED and discharged (0%). Patients in stage 4 were also more likely to require airway intervention (67%) compared with other stages (stage 1, 0.1%; stage 2, 8.6%; stage 3, 16%) (Table 3).
Table 3. Number and predictive probabilities of disposition and airway intervention based on stage Stage Treated in ED and discharged Non-ICU admit ICU (any) ICU (without airway intervention) ICU (with airway intervention) n (%) PP n (%) PP n (%) PP n (%) PP n (%) PP 1 160 (73) 0.85 24 (46.2) 0.13 4 (8.2) 0.02 4 (13.8) 0.025 0 0.001 2 13 (5.9) 0.52 7 (13.5) 0.28 5 (10.2) 0.2 5 (17.2) 0.086 0 0.086 3 46 (21) 0.45 21 (40.4) 0.2 36 (73.5) 0.35 18 (62.1) 0.21 18 (90) 0.16 4 0 0 0 0 4 (8.2) 1.0 2 (6.9) 0.17 2 (10) 0.67 ED, emergency department; ICU, intensive care unit; PP, predictive probability. DISCUSSIONThis study evaluated a staging system based on anatomical location of angioedema for patients presenting with angioedema in a single academic ED. We found the staging system to be highly correlated with level of care and need for airway intervention. Laryngeal and tongue edema (stages 3 and 4) were most associated with the need for ICU-level care and airway intervention. By contrast, soft palate and posterior pharynx (stage 2) and lip, face, periorbital, extremities, and total body/diffuse swelling (stage 1) were least associated with ICU admission or airway intervention.
The association between need for airway intervention in laryngeal and tongue angioedema (stage 3 and 4) and the lack of need for airway intervention in face and lip angioedema (stage 1) is consistent with previous reports.9, 14-17 Although not investigated in this study, others have also noted multiple affected sites to be associated with the need for airway intervention.14, 17, 18 Taken together, the airway should be closely monitored in stage 3 and 4 patients and those presenting with multiple affected sites. Considering this early in the treatment course could help with management planning as well as more quickly mobilizing the appropriate resources and personnel to care for these patients.
Airway management in these patients can be difficult. Although there are not universally accepted guidelines, consensus parameters endorsed by the American College of Allergy, Asthma and Immunology and the Society for Academic Emergency Medicine suggest patients should receive general monitoring similar to other respiratory or airway complaints.8 They add that the decision to intubate can include clinical gestalt, but objective measures such as direct visualization should be done on all patients with tongue, soft palate, or floor of mouth swelling, if easily available.8 Fiberoptic and video laryngoscopy, when done with history and examination, has been shown to be reliable in determining those at high risk of need for airway intervention8, 19, 20 and as a safe method of intubation.6, 8, 20, 21 These findings highlight that the extent of angioedema involvement is the key to subsequent intervention and ED clinicians should consider early direct airway visualization when appropriate.
This study had a large number of patients discharged from the ED, which differs from other reports.9, 15-19 This difference is likely related to the lower number of stage 4 angioedema cases, presumably from selection bias. This report, unlike many of the others, was not conducted with otolaryngology and did not require angioedema be of the head and neck. It is also possible that clinicians are more aware of appropriate management of angioedema; however, the use of targeted pharmacotherapy for angioedema remained rare, and further education and input from allergist may be of benefit.
This study does show that ambiguity remains for stage 2 and 3 angioedema. These patients require careful consideration of other aspects of presentation, including concurrent symptoms, disease progression, response to therapy, and other comorbidities. It is prudent that these patients undergo airway assessment by an ED provider or other specialist to determine the need for intervention and higher level of care. It also implies the potential utility of targeted pharmaceutical therapy to prevent the progression of disease into larynx.
It should be noted that other staging criteria for angioedema have been reported.22, 23 These staging schemes have primarily been studied in instances of angiotensin-converting enzyme inhibitor–associated angioedema, although limited studies do report some use in other settings.18 Similar to the Ishoo criteria, however, these have not been validated and would need further study before being used to guide management decisions.
LimitationsThis study has several limitations. First, this was a retrospective review, so we relied on the accuracy of clinical data documented in the chart. Second, the physical examination was not standardized, so there may have been variation in details of the examination between physicians. The predicted probability correlated with stage, however, so we believe that the study results are still valid. Third, assessment of etiology of angioedema was not standardized and was reported by physicians of different specialties, resulting in a clinical variability. Fourth, we employed a complete case analysis, so we did not account for cases that included missing values. Finally, many patients did not follow-up with allergy and immunology, but we identified many cases of angioedema based on the chart review.
CONCLUSIONIn summary, our study evaluated the angioedema staging system proposed by Ishoo et␣al. by confirming that the stages were valid predictors of disposition and need for airway intervention in patients presenting to the ED with angioedema. Although further study is required, we suggest, as others have,7, 9, 15 that when presentation is limited to predental structures (stage 1), ED management is likely sufficient for the majority of cases. When presentation includes the larynx (stage 4), ICU and the potential for airway intervention should be anticipated. Patients presenting with stage 2 or 3 should have careful airway assessment to help with decision of further intervention and disposition. Using these staging criteria could be of benefit to the triage and management of patients presenting with angioedema; however, prospective validation will be imperative before dissemination.
ACKNOWLEDGEMENTSWe appreciate statistical analysis by Karisa Harland, MPH, PhD for this study. This study received a seed grant from the Department of Emergency Medicine at the University of Iowa Carver College of Medicine.
DISCLOSUREApproval of the Research Protocol: This research was approved by the University of Iowa Institutional Research Board.
Informed Consent: Waived as the study was considered minimal risk.
Registry and the Registration No. of the Study/Trial: Not applicable.
Animal Studies: Not applicable.
Conflict of Interest: None declared.
留言 (0)