COCPs, containing ethinyl-estradiol (EE) and progestins given cyclically or continuously have long being used for the treatment of endometriosis. They are effective in ameliorating endometriosis-associated pain and have been used post-surgery to prevent recurrence. They are one of the first line symptomatic treatments for women suffering from this condition [15, 23].
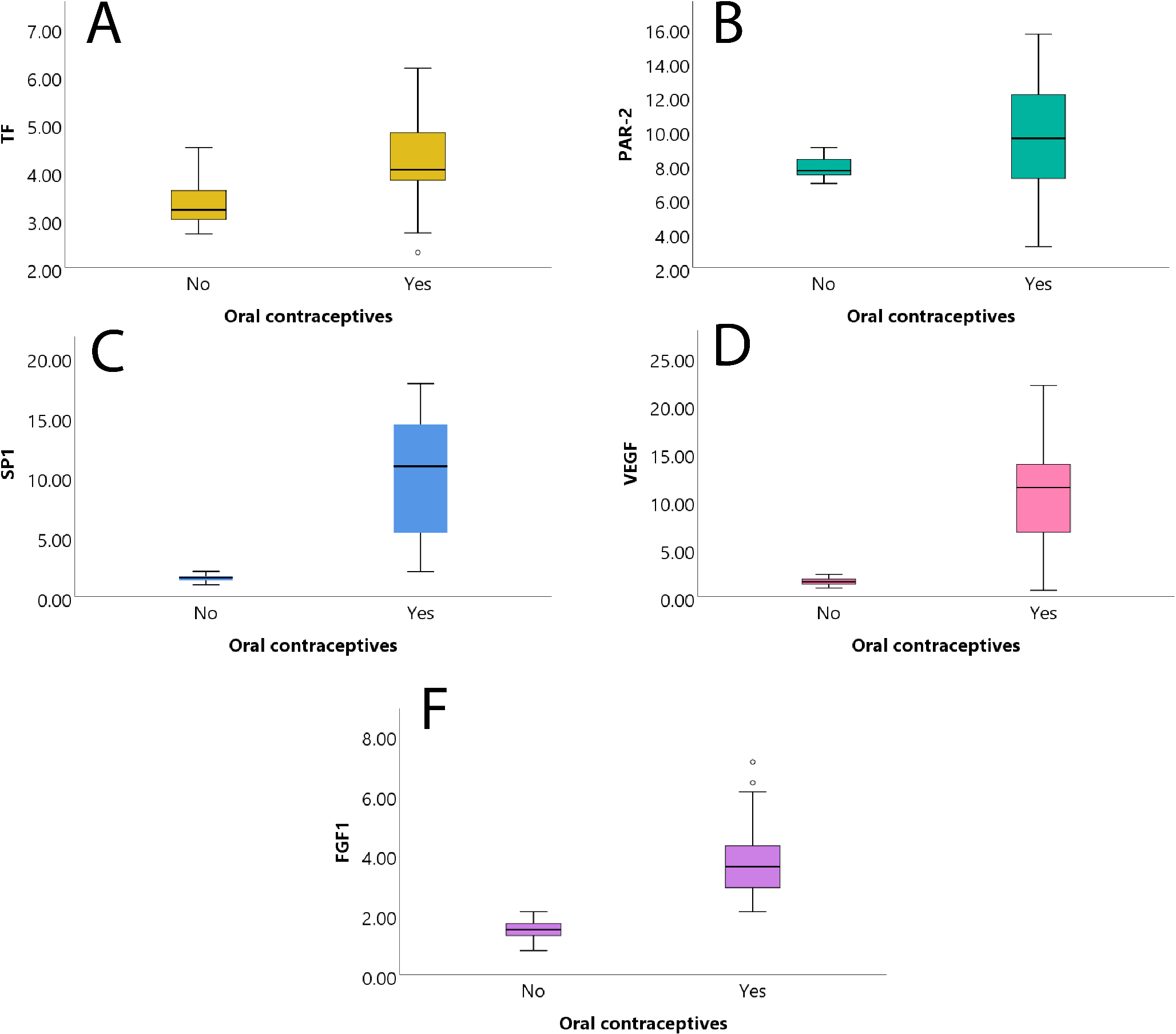
In the current study, we evaluated the effects of COCP administration on various angiogenic growth factors in women with endometriosis. Recently we showed that GnRH-a administration decreased the mRNA expression of VEGF-A, TF, and PAR-2 in endometriotic tissues from women with endometriosis [24]. Working upon this notion, we hypothesized that COCPs can also decrease the expression of angiogenic factors in women with endometriosis. On the contrary, we obtained the exact opposite result, observing that COCP administration given cyclically for 3 months significantly increases the mRNA expression of VEGF-A, TF, SP1, and FGF1 with a moderate increase of PAR-2. This might be due to the effect of estradiol on angiogenetic factors.
In women without endometriosis, estrogens increase the expression of angiogenic factors, whereas progesterone (P4) alone exerts a variety of angiogenic or antiangiogenic effects, with various influences on neovascularization. Both ovarian sex steroids, estradiol (E2) and progesterone (P4), play a role in angiogenesis in the endometrium, this being demonstrated in the difference in VEGF expression in the proliferative vs. the secretory phase [25]. VEGF expression has been found to be enhanced in the late proliferative and early secretory phase vs. the early proliferative phase, while in the late secretory phase, VEGF was moderately expressed, an event that correlated with the absence of E2 and P4 [25]. Similarly, another research work demonstrated lower VEGF mRNA expression during the secretory phase, correlating this finding with the presence of progesterone and the absence of estrogens [27]. When cultures of endometrial stromal cells were added to medroxyprogesterone acetate, the release of VEGF was inhibited [26]. Notably, mid-secretory expression of VEGF receptor is considered necessary for the proper implantation of the embryo [26]. Our results demonstrate that COCPs not only do not suppress mRNA VEGF-A expression but, in fact, upregulate it, since all the women we studied were in the proliferative phase. This is the first time, as far as we know, that the expression of VEGF-A mRNA has been studied in endometriomas after COCP use; the only bibliographic reference that has studied VEGF protein expression after COCP use using immunohistochemistry was in the endometrium of patients with myomas and menorrhagia [26]. In these patients, aged 35–49, VEGF protein expression was found to be diminished compared to that of patients in the proliferative phase and without a history of COCP use [27]. In general, it may be hypothesized that this result is due to the effect of progesterone rather than to that of estradiol.
While oral contraceptives (OCs) often reduce VEGF expression in the normal endometrium, endometriotic lesions present a more complex environment. One research paper has shown that 17β-estradiol drives VEGF via the Wnt/β-catenin pathway [27], this observation being supported by other studies highlighting the importance of hormone-Wnt signaling in reproductive tissues [28, 29]. However, endometriotic cells frequently exhibit progesterone resistance partly because of altered progesterone receptor expression and function [30,31,32]. This lack of responsiveness is further amplified by the chronic inflammatory state typical of endometriosis where cytokines such as IL-6 and TNF-α can work in tandem to elevate VEGF levels [1, 33]. Additionally, mounting evidence indicates that local steroid metabolism and nuclear receptor signaling diverge significantly in endometriotic lesions compared to the eutopic endometrium, altering how these tissues respond to OCs [34, 35]. As Bulun notes, the modified endocrine microenvironment in endometriosis can counteract progestin’s usual suppression of angiogenic factors [36]. Taken together, these findings explain why, in contrast to the inhibitory effect of OCs on VEGF in the eutopic endometrium, endometriotic lesions might maintain or even raise VEGF production.
In addition to its role in the hemostatic cascade, TF is involved in angiogenesis through signaling that utilizes the protease-activated receptor 2 (PAR-2) [37]. In previous studies, TF was found to be increased in the blood of women treated with COCPs, more specifically in monocytes [38]. In another study, antiprogestin RU486 was observed to inhibit the progestin-enhanced transcription of pTF 278 and pTF 111 promoter constructs; moreover, several studies have reported that TF is persistently upregulated in human endometrial stromal cell decidualized by progestins [39]. Our results are in accordance with those of the above studies since the administration of COCPs significantly increased the expression of TF mRNA focally on endometriomas.
PAR-2 contributes to the progression of endometriosis according to several studies [40]. PAR-2 is present on human vascular ECs and mediates EC proliferative responses when activated [41]. In a study published in 2014 in a mouse xenograft model of human endometriosis, PAR-2 inhibitor ENMD-1068 dose-dependently inhibited endometriotic lesion development and IL-6 and NF-κβ expression [40]. In our study, as regards PAR-2 mRNA expression after COCP use in woman with endometriosis, a slight decrease in expression was noted between OC + and the control group. In contrast, GnRH-a was found to significantly suppress PAR-2 expression in women with endometriomas [24]. Our findings have confirmed the fact that COCPs do not suppress endometriosis development and alleviate endometriosis-related symptoms solely via other mechanisms.
Specificity protein 1 (Sp1) is an important transcription factor that regulates many critical biological functions, including cell proliferation, apoptosis, invasion, and metastasis by binding to the promotor regions of its target genes. Previous studies have demonstrated that Sp1 is aberrantly expressed and plays important roles in cancer by stimulating the growth of tumor cells. However, the expression and role of Sp1 in endometriosis remains unknown.
SP1 is a transcription factor that regulates numerous functions, such as cell proliferation, apoptosis, and invasion [42]. Investigators have found that SP1 mRNA and protein are highly expressed in the ectopic endometrium compared with the normal endometrium, thus verifying that in endometriosis SP1 is upregulated [42]. Based on the above data, we studied the effect of COCPs on SP1 expression in endometriotic tissues and found that SP1 was even higher in the OC + group than in the control group. It appears that not only is SP1 expression not affected by COCP use but it is further enhanced. On the other hand, as recently published, GnRH-a has no effect on SP1 expression in endometriotic tissues [24].
The receptor FGFR1 is expressed in vascular ECs, its activation leading to activation of FGFR3 in the endothelium [14]. FGF signaling is hypothesized to influence the entire process of angiogenesis, while up-regulation of FGFR1 and FGFR2 promotes angiogenesis and vascular endothelial proliferation [43]. Extracellular matrix degradation, an important step of angiogenesis, is promoted by several FGFs, including FGF1, via upregulation of MMP expression in ECs [43]. That is why we chose FGF1 as an important protein and studied its gene expression in endometriosis while exploring how COCPs might affect it. Our results demonstrated a higher expression in the OC + group than in the control (OC-) group. This demonstrates that FGF1 expression is likely to be hormone-dependent and should be of concern to gynecologists treating women who suffer from endometriosis with COCPs since their role in angiogenesis is questionable.
The present study is of high originality given the fact that it is the first time, to the best of our knowledge, that a study has explored the impact of COCP treatment preoperatively on angiogenetic pathways in women with endometriosis. One disadvantage of the present study is that we examined only the mRNA expression of TF, PAR2, VEGF, SP1, and FGF1 and not their protein expression using Western blot, ELISA, or immunohistochemistry. COCPs do not clearly inhibit neoangiogenesis in endometriotic lesions; on the contrary, some angiogenetic pathways may be upregulated. Further research should be conducted to discover new, more effective treatments for endometriosis, a common disease that affects many women of reproductive age, and identifying ways to affect its angiogenesis holds much promise in this direction.







留言 (0)