
記住我
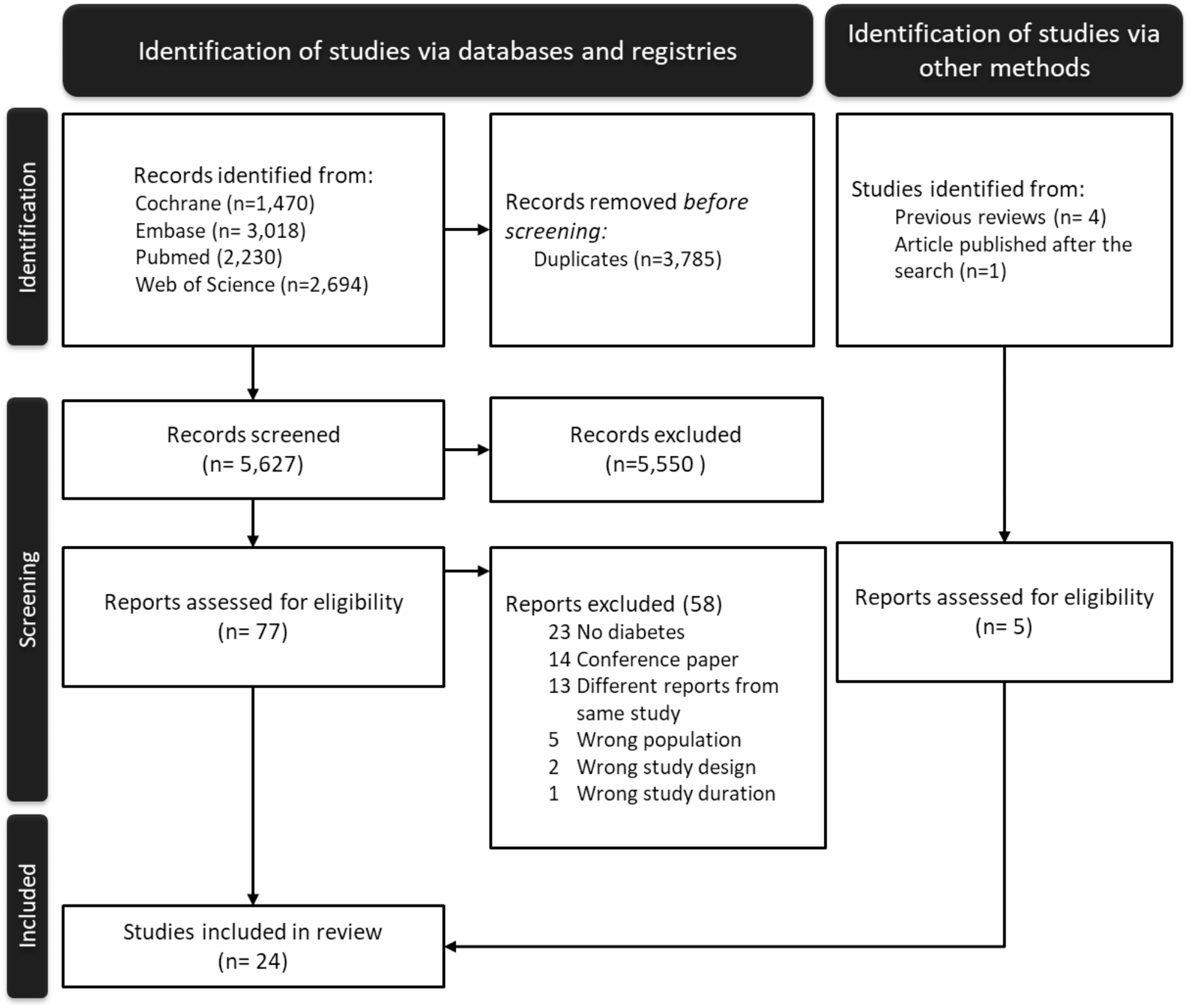
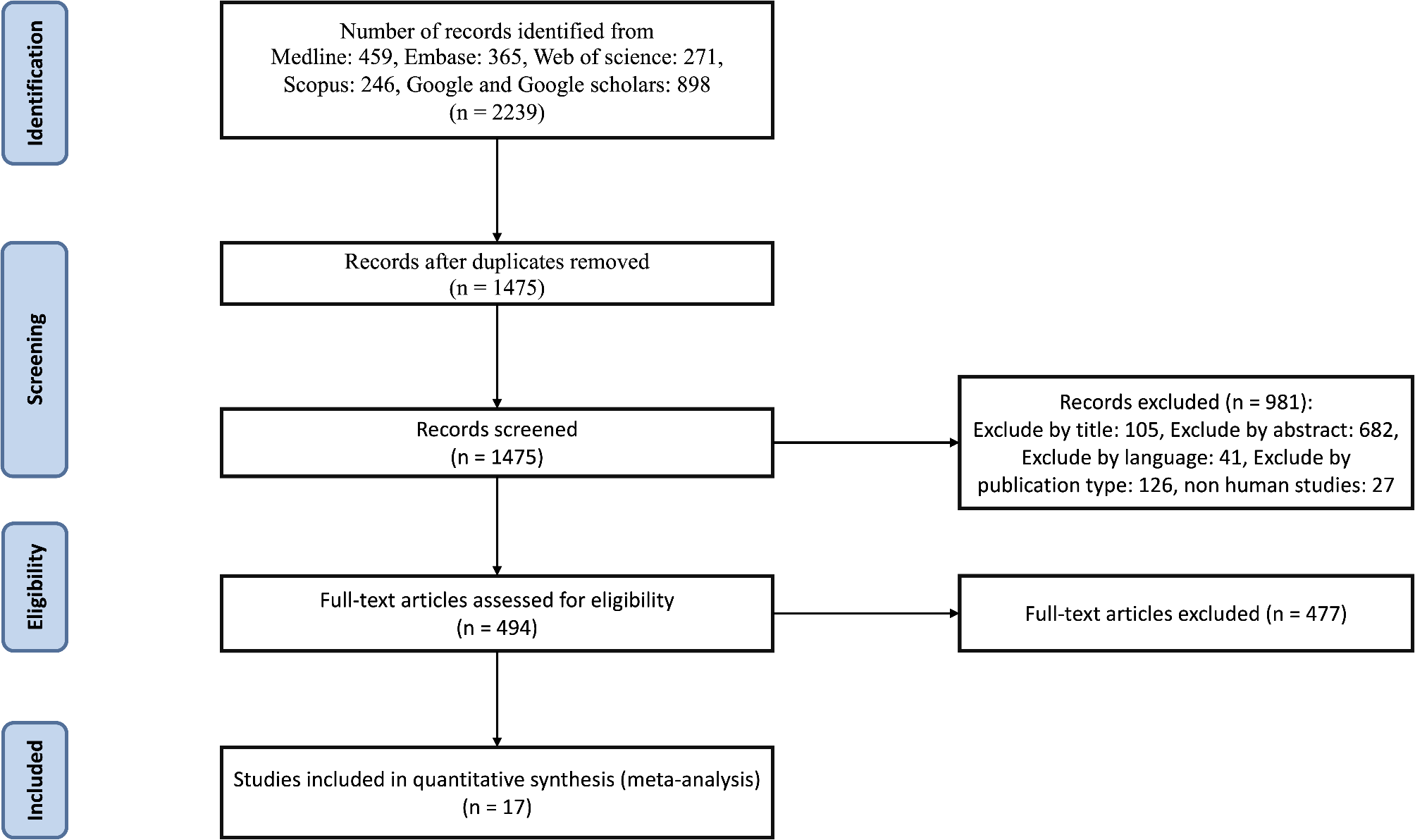
As seen in Fig. 1, after removing 3,785 duplicates, we obtained 5,627 records for title and abstract scrutiny. We excluded 5,550 records, leaving 77 reports for more detailed checking and evaluation, including full-text scrutiny. After excluding 58 reports for not presenting relevant data (Supplementary Table 2) and adding five reports (four identified from previous systematic reviews [24,25,26,27] and one recently published by three coauthors) [10], we identified a total of 24 studies with sufficient information to estimate the incidence of diabetes [21, 24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46].
Fig. 1
Flowchart for the identification of trials of lifestyle interventions offered to women following a pregnancy complicated by gestational diabetes that reported the incidence of type 2 diabetes
Description of studiesAs seen in Table 1, the initial trial was published in 1999. After a decade, new trials were published almost yearly, ten during the last five years. Studies originated from most regions of the world -- five from Europe, four from American regions (three from North and one from South America), three from Oceania, and 12 from Asia. Half of the studies were from low- and middle-income countries. Although focusing our search on randomized trials, we did include one study that used historical controls to compare with the women receiving the experimental intervention. Three studies were cluster randomized trials, and 20 were individually randomized trials. There were six pilot or feasibility trials.
Table 1 Characteristics of studies evaluating a lifestyle intervention program for the prevention of type 2 diabetes after a pregnancy complicated by gestational diabetes mellitus (GDM)The diagnostic criteria for GDM varied. Five studies [35, 39, 40, 44, 45] used the International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria [47], three [33, 42, 43] the World Health Organization criteria [48], three [25, 30, 38] the Carpenter & Coustan criteria [7], three other criteria [36, 37, 41], and 10 did not specify the criteria used.
In nine studies, eligibility criteria required participants not only to have GDM, but to have an additional indication of being at higher risk for type 2 diabetes: having postpartum intermediate hyperglycemia (seven studies) and/or requiring medication to treat gestational diabetes (two studies).
Most studies intervened on diet and physical activity (22 studies), one only on diet and one only on physical activity, with variable delivery modes including onsite and at-home individual and group sessions, telephone sessions/chats, apps, or web-based platforms. Although interventions were predominantly delivered after pregnancy, generally starting soon after the postpartum glycemic reevaluation (less than two years), in five, they began during pregnancy, and in two, they allowed initiation up to four to five years after pregnancy. Interventions were not intensive and lasted from four months to four years.
The control group also received some degree of lifestyle intervention considered necessary by trial investigators, the intensity of which increased in more recent trials. This intervention included, among others, management by clinicians outside of the trial and written materials.
The incidence of diabetes was the primary outcome in nine studies. In the remaining studies, diabetes was a secondary or exploratory outcome or, though not listed as an outcome, was reported when new cases were detected. In five studies, the assessment of diabetes was done over less than one year of follow-up, in the remaining over approximately one year (10 studies), two years (four studies), or three or more years (five studies).
Risk of biasA detailed description of the risk of bias assessments is provided in the Supplementary Tables 3 and 4 and Supplementary Figs. 1 and 2.
For the incidence of diabetes, we evaluated 24 studies, six we judged as having a high risk of bias [27, 29, 34, 37, 44, 46], six as having a low risk of bias [21, 30, 32, 41, 42, 45], and the remaining 12 studies as presenting some concern. Among high-risk bias studies, the high risk arose from the randomization process in three, was due to deviations from the intended intervention in two, and was due to missing outcome data in four. The 12 studies with some bias concerns presented less severe problems in one or more of the above three dimensions.
For the weight change outcome, we gathered results from 16 studies, five of which had a high risk of bias. Among the 11 studies without a high risk of bias, we considered four to be of some concern and seven to have a low risk of bias. The risk of bias we identified regarding the outcome weight change occurred in the exact dimensions of those found in the articles on the incidence of diabetes.
Effect of LSI on the incidence of diabetesThe 24 studies analyzed (9017 women) provided 762 incident cases of diabetes over an average follow-up time of 19.4 months. LSI reduced the incidence of diabetes by 24% (RR = 0.76; 95% CI 0.65–0.89).
To enhance certainty, we did not include the six studies with a high risk of bias in the analyses producing our main results. As seen in Fig. 2, of the remaining 18 studies (8,357 women, 727 incident cases), all but two favored LSI. Individually, most studies did not achieve statistical significance, with effects ranging from RR = 0.09 (0.01, 1.60) to RR = 2.87 (0.12, 66.60). Over an average follow-up time of 21.8 months, LSI reduced the incidence of diabetes by 19% (RR = 0.81; 0.71, 0.93). The effect was numerically higher (p = 0.52) in the eight studies selecting women with GDM having a particularly higher risk of type 2 diabetes (RR = 0.78; 0.65, 0.94), compared to studies selecting all women with GDM, irrespective of diabetes risk (RR = 0.85; 0.70, 1.04).
Fig. 2
Effectiveness (risk ratios) of a lifestyle intervention program to prevent type 2 diabetes after a pregnancy complicated by gestational diabetes in the 18 studies without high risk of bias. Top: Women with GDM at higher risk. Bottom: Women with GDM. *Estimated from the annual risk in each group and multiplied by the study median length of follow-up
Figure 3 shows the overall absolute risk difference for the 18 studies (RD = − 0.018 (95% CI -0.027; -0.008), translating into an NNT of 56. However, in studies for women with GDM with a particularly high risk of type 2 diabetes, we found a numerically larger (p = 0.16) effect (RD = − 0.032; 95% CI -0.050, -0.014), translating into an NNT of 31. These findings contrasted with the non-significant risk difference found (RD = − 0.014; 95% CI -0.030, 0.002; NNT = 71) in studies of women with GDM, irrespective of risk.
Fig. 3
Effectiveness (risk differences) of a lifestyle intervention program to prevent type 2 diabetes after a pregnancy complicated by gestational diabetes in the 18 studies without high risk of bias. Top: Women with GDM at higher risk. Bottom: Women with GDM. *Estimated from the annual risk in each group and multiplied by the study median length of follow-up
Effect of LSI on postpartum weight changeFor two studies, there was no information to assess weight change in the publication reporting the incidence of diabetes, and we extracted it from other publications of these studies [49, 50]. As seen in Fig. 4, the effect of LSI on postpartum mean weight change was assessed in 16 studies having the appropriate information. Differences in weight varied from 4.4 kg less to 3.4 kg greater weight gain with LSI in the individual studies. With an average follow-up time of 10.5 months, the overall summary difference was − 0.88 kg (-1.52, − 0.23), I2 = 66%.
Fig. 4
Effectiveness (weight difference, kg) of a lifestyle intervention program to prevent type 2 diabetes after a pregnancy complicated by gestational diabetes in the 11 studies without high risk of bias
When we excluded the five studies with a high risk of bias, the overall mean difference in the remaining 11 studies after 11.5 months of follow-up was − 0.62 kg (-1.21; − 0.02), I2 = 65%.
Sensitivity analysesAs seen in Table 2, the protective effect in reducing the incidence of diabetes decreased as the quality of studies increased. The six studies with a high risk of bias had the greatest protection (RR = 0.19; 95% CI 0.08–0.50), and the six studies with a low risk of bias had the lowest protection, which was borderline statistically significant (RR-0.86; 0.73, 1.00). In an additional analysis, studies having at least one year of follow-up had a somewhat larger protective effect (RR = 0.73; 0.59, 0.90). Finally, the effects found with fixed effect models were similar to those found using random effect models. Thus, our main finding of an RR = 0.81 (95% CI 0.71, 0.93) in the 18 studies without high risk of bias was robust in these various sensitivity analyses.
Table 2 Sensitivity analyses of the effectiveness of lifestyle interventions to prevent type 2 diabetes after a pregnancy complicated by gestational diabetesAlthough evaluated in a lower number of studies, the effect of weight change was also robust in various sensitivity analyses, the mean difference being somewhat lower in studies without a high risk of bias.
Publication biasA funnel plot (Supplementary Fig. 3) showed asymmetry in estimating the effects of LSI on the incidence of diabetes (Egger’s test p = 0.01). However, trim and fill analyses adding six hypothetical studies to compensate for the six asymmetric studies identified by the plot resulted in little change in the effect size (RR = 0.83; 95% CI 0.72, 0.96), demonstrating that the asymmetric, small-sized studies included in the meta-analysis caused only a minimal imbalance.
Certainty of the evidenceIn Supplementary Table 5 we present the evaluation of the quality of the evidence using the GRADE system.
The evidence for the incidence of diabetes outcome based on the 18 studies without high risk of bias encompassed 8,357 women and 727 events. Starting from high certainty, as defined by the studies with randomized design, we lowered certainty to moderate, given that 12 of the 18 studies presented some concerns in our evaluation of the risk of bias. No reduction was necessary for heterogeneity, imprecision, indirectness, or publication bias.
For weight change, the evidence provided was based on the 11 studies that did not present a high risk of bias, encompassing 7,104 women. Starting from high certainty, as defined by the studies’ randomized design, we lowered certainty to moderate due to heterogeneity. No reduction was necessary for risk of bias, imprecision, indirectness, or publication bias.
留言 (0)