
記住我
Based on the pre-test data estimation [18,19,20], 30–40 participants were included in each group, totalling approximately 90–120 cases.
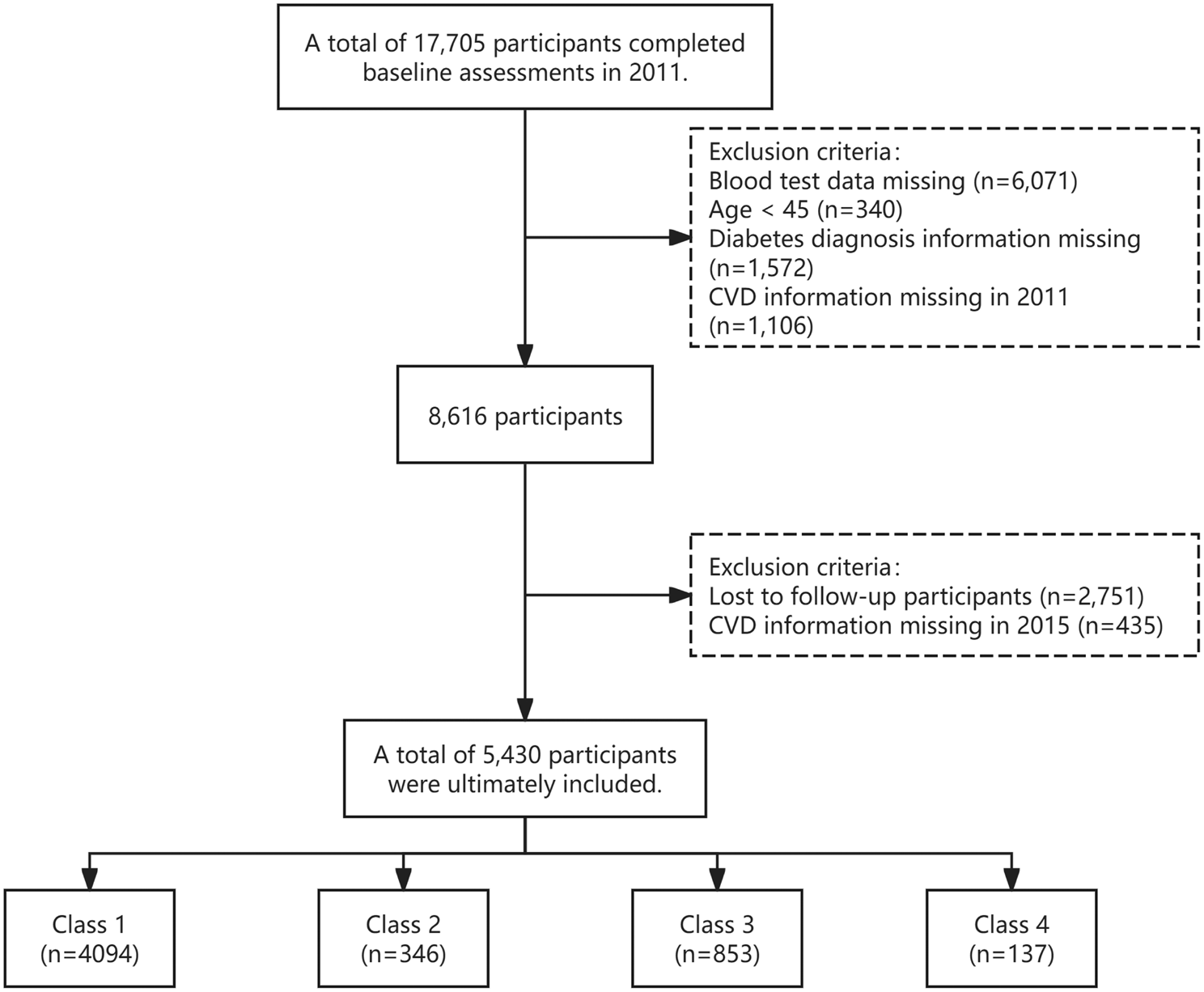
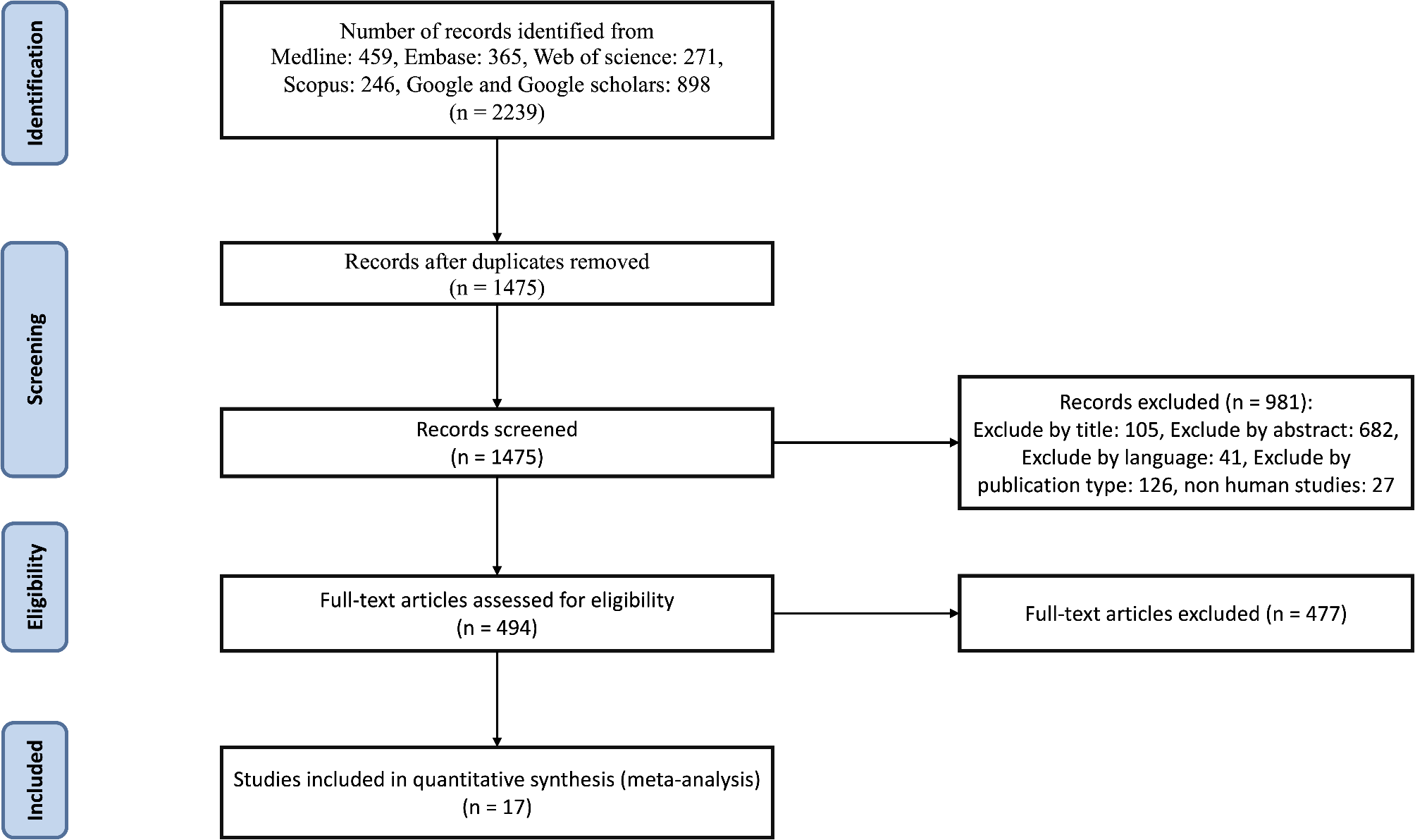
ParticipantsThis trial was conducted in Chongqing, China, between July 2021 and December 2021; 100 participants who were eligible for the test were selected from the Sihai Community Health Service Center of Chongqing Nanan District People's Hospital and the Health Management (Physical Examination) Center of the Second Affiliated Hospital of Chongqing Medical University. The flow diagram depicting the enrolment of the participants in the study is shown in Fig. 1.
Fig. 1 Inclusion criteria
Inclusion criteriaThe inclusion criteria were: (1) age between 50 and 75 years; (2) residence near the hospital without any plan to change residence or leave the city during the trial; (3) patients with type 2 diabetes and hypertension comorbidity, currently on consistent antihypertensive and anti-glycaemic medications, adhering to the criteria outlined in the "Chinese Guidelines for the Prevention and Control of Hypertension, Revised Edition, 2018" [21] and the diagnostic criteria for diabetes as per the "Chinese Guidelines for Prevention and Control of Type 2 Diabetes, 2017 Edition" [22]; (4) commitment to strictly consuming the two daily meals provided during the trial; (5) signing of informed consent by the participants and their cohabitating family members.
Exclusion criteriaWe excluded the following from this study: (1) individuals with malignant tumours, recent acute-phase heart attack, stroke within the past 3 months, or other serious illnesses with a life expectancy of less than 1 year; (2) individuals with hypercortisolism or aldosteronism; (3) those experiencing acute-phase illnesses such as upper respiratory tract infections, fever, severe diarrhoea; (4) those with hearing impairments, dementia, or other disabilities that hinder normal communication, as well as severe depression or other mental disorders; (5) individuals with mobility issues preventing timely follow-up, or failure to complete follow-up after enrolment; (6) patients with chronic renal failure of stage 3 or higher, or undergoing renal replacement therapy; (7) individuals with abnormal liver function, evidenced by alanine aminotransferase or aspartate aminotransferase levels more than twice the upper limit of normal, or total bilirubin levels exceeding the normal upper limit; (8) individuals with abnormal potassium levels, below 3.5 mmol/L or above 5.5 mmol/L, or those taking potassium-sparing diuretics; (9) pregnant individuals or those likely to become pregnant, and others unsuitable for the trial product; (10) individuals consuming low-sodium salt or participating in other clinical studies deemed inappropriate for trial inclusion by the investigator; and (11) individuals considered unsuitable for enrolment with the trial product by the investigator.
Study designThis study used a randomized, controlled, single-blind trial with a semi-open design. A total of 100 patients with hypertension and type 2 diabetes were recruited and enrolled through community hospitals. The participants were allocated into three groups: Group A, the control group (CM-DASH diet + common salt, n = 34); Group B, the 23% salt group (CM-DASH diet + 23% sodium-restricted formula salt, n = 33); and Group C, the meal packs group (CM-DASH technology package + 23% sodium-restricted formula salt, n = 33).
Salt consumption was maintained at 5 g/day per capita in all groups, aligning with World Health Organization-recommended salt standards. After completing the baseline survey and physical examination, an 8-week dietary intervention was initiated. This intervention comprised the dietary guidance phase during weeks 1 and 2 (distribution of salt + CM-DASH dietary recipes), centralized meal feeding phase during weeks 3 and 4 (meals provided in the hospital cafeteria), and home health care phase during weeks 5–8 (distribution of salt + CM-DASH dietary recipes). Weekly follow-up visits were conducted to gather data on blood glucose levels, salt consumption, and adverse events, as well as to reinforce adherence to recommended salt intake and dietary guidelines. Questionnaires and physical examinations were repeated at week 4 and at the conclusion of the intervention.
CM-DASH recipesAccording to the recommendations of the Chinese Guidelines for the Prevention and Control of Type 2 Diabetes (2018 Edition) and the Chinese Guidelines for the Prevention and Control of Hypertension (2017 Revision), respectively, patients with diabetes should adopt a diversified dietary pattern that is "cereal-based, with a high intake of dietary fibre, and low in salt, sugar, and fat," whereas patients with hypertension should consume mainly fruits, vegetables, low-fat dairy products, whole grains rich in dietary fibre, and vegetable-derived protein, and reduce the intake of saturated fat and cholesterol. The researchers formulated a collection of recipes tailored for Chinese patients suffering from hypertension and type 2 diabetes, drawing upon the dietary habits prevalent within the Chinese population. This approach aligns with the strategies outlined in that paper [20]. All participants cooked food at home (during the first, second, and fifth to eighth weeks) using the recommended recipes (Table 1).
Table 1 Nutrient composition of CM-DASH (Chinese Modified Dietary Approaches to Stop Hypertension) dietMeal packsThe meal packs (CM-DASH Nutritional Meal Packs, produced by Chongqing Shanshun Biotechnology Co., Ltd., adhering to Product Standard GB/T29603; Food Production License No. SC12450023228393) are designed for the dietary treatment of type 2 diabetes and hypertension. They are tailored to the dietary structure and habits of Chinese people, incorporating principles of dietary management for hypertension and diabetes. This includes the selection of traditional Chinese medicines used in treating these conditions, as well as modern nutritional medicines for hypertension and diabetes. It uses mixed-grain and homogenized meals as the core of the nutritional intervention treatment and was provided as an intervention for Group C. It included the following items: CM-DASH Homogenized Meal Solid Drink (homogenized meal for breakfast), CM-DASH Solid Drink (Normal Companion), and CM-DASH Eight Treasures Rice (Rice for Mid-Dinner). The ingredients of each item are shown in Table 2.
Table 2 The meal packs (CM-DASH Nutrition Dietary Packs) compositionSalt useThe test salt was used throughout the trial as a substitute for the participants' household salt. Group A received common salt ("Jing Xin," manufactured by Chongqing Salt Industry Group Co., Ltd. Name: purified salt; product standard: NY/T1040; sodium chloride content: > 99%). Groups B and C received 23% low-sodium salt ("Shan Yi Kang" manufactured by Chongqing Shanshun Biotechnology Co., Ltd. Name: solid compound condiment, standard of execution: Q/SWS 0025S, food production license number: SC10650012000709; main ingredients include potassium chloride [56%], sodium chloride [23%], and protein [3.0%]). We provided participants with dosing spoons to help them manage their salt intake at home, ensuring it did not exceed 5 g per person per day. Additionally, an electronic scale with a precision of 0.1 g was utilized to monitor weekly salt consumption, from which the daily salt intake for each family member was estimated.
Blood glucose measurementParticipants attended follow-up appointments in the hospital once a week. Glycaemia (standardized meal tolerance test) was measured by professionally trained researchers using a medical blood glucose meter (Dahl C type, GM505RAB). The researchers made the measurements strictly following the clinical application guideline for blood glucose monitoring in China (2021 edition). All participants were asked to complete a fasting blood glucose measurement at 8:00 a.m., and postprandial blood glucose was measured 2 h (counted from the first bite of breakfast eaten) after breakfast was distributed on site.
The glycaemic control rate was defined as a fasting blood glucose level of < 7.0 mmol/L and a postprandial blood glucose level of < 10.0 mmol/L.
Statistical analysisThe Kolmogorov–Smirnov test was used to test the normality of the data, and the Levene test was used to test the chi-square of the groups. Normally distributed continuous variables were expressed as the mean ± standard deviation using the independent samples t-test; skewed continuous variables were expressed as median and interquartile range using the Kruskal–Wallis H test. Categorical variables were expressed as counts and percentages using Pearson's chi-square test or continuous corrected chi-square test. The continuously measured blood glucose value were analysed using generalized estimating equations. All statistical analyses were performed using SPSS 27.0 (IBM, Armonk, NY, USA) statistical software, and the tests were two-sided, with differences considered statistically significant at P < 0.05.
留言 (0)