
記住我
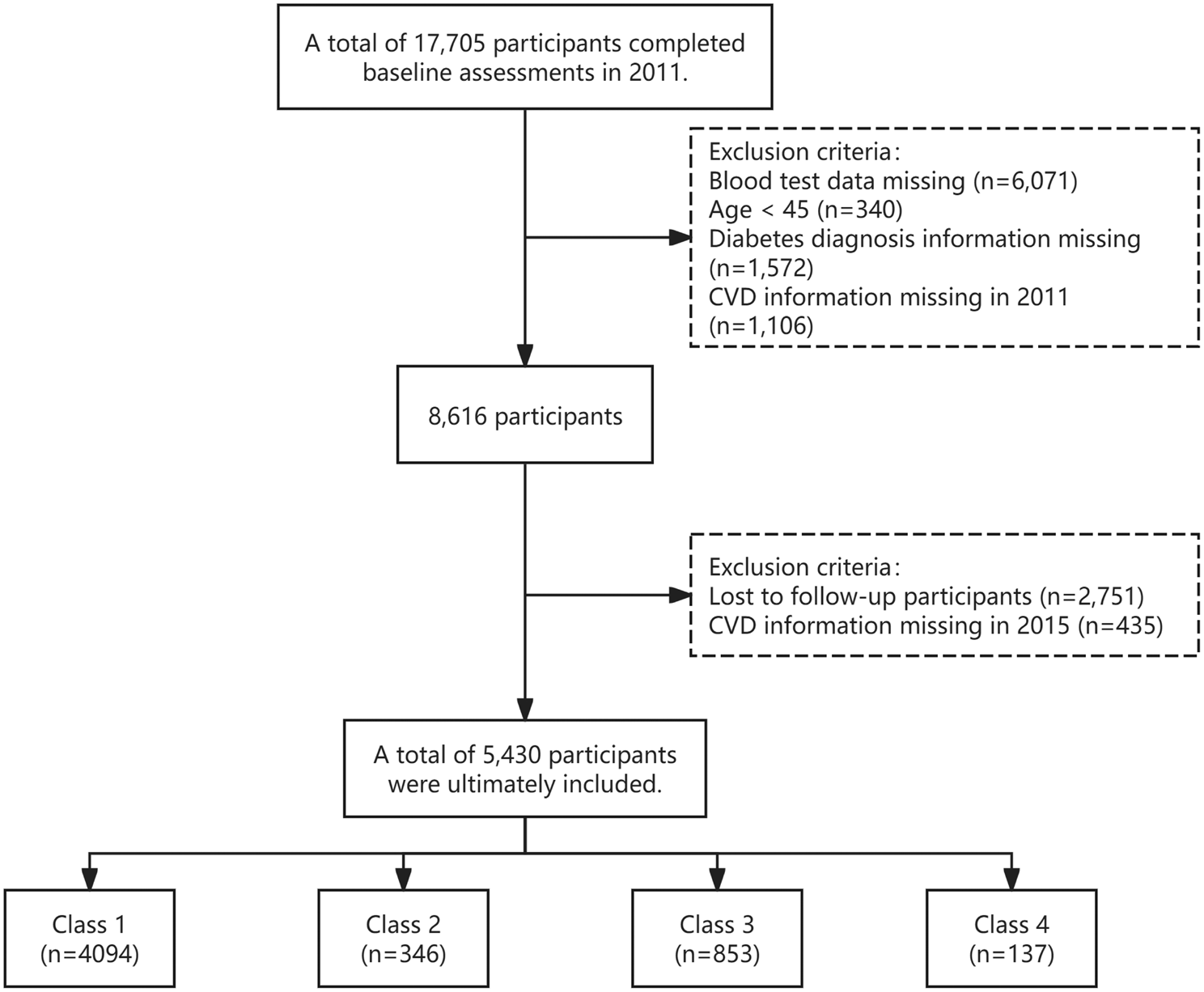
In our study, we conducted a retrospective analysis of data from the ACCORD trial, which was funded by the National Heart, Lung, and Blood Institute. The ACCORD trial adopted a multicenter, randomized, and double 2 × 2 factorial design approach with the aim of elucidating the impact of three distinct medical treatment strategies. These strategies encompassed the glycemia trial, the lipid trial and the blood pressure trial, and sought to assess their effects on the morbidity and mortality of the study participants. The trial included a total of 10,251 middle-aged and older individuals diagnosed with type 2 diabetes, with a mean glycated hemoglobin level of 8.3% and a median diabetes duration of 10 years. Recruitment for the ACCORD trial took place between June 2001 and October 2005 at 77 research sites located across the United States and Canada. All participants were characterized by a high risk of CVD events, either due to the presence of clinical CVD, a high likelihood of CVD, or the presence of two or more high-risk factors for CVD. The specific inclusion and exclusion criteria for the study can be found in the original ACCORD study [20]. Participants who were missing the baseline remnant-C values were excluded from our study. It’s important to note that the use of the ACCORD dataset in this study has been approved by the National Heart, Lung, and Blood Institute and the institutional review board of Xiangya Hospital, Central South University, ensuring adherence to ethical and regulatory standards.
Data collection and outcomesThe collected data encompassed a range of variables, including demographics (such as age, sex, race, education levels, smoking habits, alcohol consumption, and body mass index), common clinical indicators (including blood pressure, HbA1c, duration of diabetes, history of cardiovascular disease, blood lipid profiles, heart rate, and treatment regimens), and traditional kidney risk factors (serum creatinine, estimated glomerular filtration rate, and urinary albumin levels). To compute remnant-C levels, we utilized the following formula: remnant-C = Total Cholesterol (TC) - Low-Density Lipoprotein Cholesterol (LDL-C) - High-Density Lipoprotein Cholesterol (HDL-C). Among the initial cohort of 10,251 patients with type 2 diabetes, individuals lacking remnant-C values were excluded, resulting in the analysis of 10,196 patients with T2DM in the current study. Our study focused on three specific adverse renal outcomes, each previously defined based on ACCORD criteria: the development of albuminuria, indicated by a urinary albumin level equal to or exceeding 30 mg/dL; the occurrence of worsening renal function, defined as a doubling of serum creatinine levels or a decrease in estimated glomerular filtration rate by more than 20 mL/min/m2; progressing to renal failure, defined as the occurrence of end-stage renal disease or serum creatinine levels exceeding 3.3 mg/dL. Kidney microvascular events were prespecified outcomes in ACCORD, and the original definitions are used [21].
Statistical analysisIn our study, we used either mean (standard deviation) or median (interquartile range) to describe continuous variables and proportions (percentage) for categorical variables to provide an overview of the demographic information. To compare groups, the analysis of variance (ANOVA) or Kruskal-Wallis test was employed for continuous variables, while the chi-squared (χ2) test was used to compare categorical variables. Participants were stratified into four distinct remnant-C groups, denoted as quartile 1, quartile 2, quartile 3, and quartile 4, based on the interquartile range of remnant-C values within the entire cohort. To elucidate the relationship between remnant-C and various adverse renal outcomes, Kaplan-Meier estimates were utilized to calculate the survival probabilities of adverse renal outcomes based on remnant-C quartiles. Differences in these estimates were then compared using the log-rank test, which assessed whether there were significant disparities in outcomes among the quartiles. To assess the association between remnant-C and the incidence of adverse renal outcomes, we applied Cox proportional hazard models. In the establishment of multivariable models, variables with a P-value<0.05 in the univariate analyses, as well as those clinically linked to adverse renal outcomes, were included in the multivariable analyses. We employed three multivariate models with progressive adjustments to account for potential confounding factors related to adverse renal outcomes. Model 1 was adjusted for age, sex, education levels, race, systolic blood pressure (SBP), diastolic blood pressure (DBP), smoking, alcohol consumption, and body mass index (BMI). Model 2 included the covariates from model 1 and added glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), duration of diabetes, serum creatinine, and urinary albumin (log-transformed). Model 3 further adjusted for the history of CVD and the treatment regimens. Furthermore, we employed restricted cubic spline analysis, which allowed for the exploration of both linear and nonlinear associations. Finally, several sensitivity analyses were conducted to assess the robustness of our findings. First, we excluded 2747 patients who had used fenofibrate at baseline to weaken the impact of fenofibrate on outcomes. Second, we excluded 3585 participants who had a history of CVD at baseline. In addition, to deal with missing baseline covariates, we used imputation methods such as single imputation. All analyses were conducted using R version 4.3.0. A two-sided P-value<0.05 was considered statistically significant in our analysis.
Baseline characteristics by quartiles of remnant-CIn Table 1, we presented the baseline characteristics of the 10,196 participants included in the study. The average age of the participants was 62.77 years, 61.5% were male, and 62.5% identified as White. The average body mass index was 32.23 kg/m2 and additional baseline characteristics are detailed in Table 1. Regarding baseline blood lipid levels, our study found that the mean TC was 183.31 mg/dL, triglycerides (TG) median was 155.00 mg/dL, LDL-C averaged 104.9 mg/dL, and HDL-C was found to have an average of 41.87 mg/dL. Notably, the remnant-C was observed to be 31.00 mg/dL. We stratified the baseline characteristics of the participants based on quartiles of remnant-C levels. It was important to highlight that baseline remnant-C levels were associated with various demographic and clinical factors, including age, race, smoking status, alcohol consumption, education levels, BMI, duration of diabetes, SBP, DBP, heart rate, use of ACEI, HbA1c, fasting plasma glucose, blood lipid profiles (TC, TG, LDL-C, HDL-C), serum potassium, serum creatinine, eGFR, urinary albumin, urinary creatinine, urinary albumin-to-creatinine ratio (UACR), glycemia trial, blood pressure trial and lipid trial.
Table 1 Subject baseline characteristics by quartiles of remnant-C levelsThe risk of adverse renal outcomes was related with quartiles of remnant-C levelsThe risk of adverse renal outcomes based on quartiles of remnant-C levels were illustrated in Fig. 1, as determined by Kaplan-Meier survival analysis. Notably, the figure indicated that patients with lower levels of remnant-C had a higher survival probability, which suggested a more favorable kidney prognosis for this group. To further assess the statistical significance of these disparities, we employed the log-rank test. The results of this test demonstrated that individuals with higher levels of remnant-C had a significantly increased risk of albuminuria (P < 0.001) and worsening renal function (P < 0.001) when compared to those with lower levels. However, the association between remnant-C and renal failure was found to be statistically insignificant (P = 0.37).
Fig. 1
Kaplan - Meier survival analysis for adverse renal outcomes according to quartiles of remnant-C levels. A. Albuminuria; B. Worsening renal function; C. Renal failure
Baseline remnant-C levels and adverse renal outcomesIn our study, we conducted the Cox proportional regression analysis using three different models with progressive adjustments to assess the risk of adverse renal outcomes. With full adjustments made in Model 3 in table 2, our study revealed the baseline remnant-C levels were associated with the risk of albuminuria [HR 1.23 (95% CI 1.06–1.43), P = 0.007] and worsening renal function [HR 1.15 (95% CI 1.05–1.25), P = 0.002] between quartile 1 and quartile 4, but not the risk of renal failure [HR 1.11 (95% CI 0.74–1.64), P = 0.621]. Moreover, as the quartiles of remnant-C increased, the risk of albuminuria (P for trend = 0.001) and worsening renal function (P for trend < 0.001) also increased, revealing a graded association between remnant-C levels and the risk of albuminuria and worsening renal function, while it was not significant for renal failure (P for trend = 0.649). Furthermore, when remnant-C levels were treated as a continuous variable, a 1-standard deviation increase in remnant-C was associated with a 6% higher risk of albuminuria and an 9% higher risk of worsening renal function (P = 0.010 and P < 0.001, respectively) after adjusting for all potential confounders. However, there was no significant association between remnant-C as a continuous variable and the risk of renal failure (P = 0.455). Our results indicated that the remnant-C could be served as a promising indicator for adverse renal outcomes. Significant differences in albuminuria and worsening renal function were still observed between quartile 1 and quartile 4, but not renal failure in the model 3. These findings were consistent with Kaplan-Meier curves and log rank test. Compared with patients with a lower remnant-C levels, those with a higher remnant-C levels had a higher probability of poor patient outcomes (P < 0.05). Overall, our study revealed a significant association between baseline remnant-C levels and adverse renal outcomes, suggesting that it may serve as a promising prognostic marker for patients with type 2 diabetes.
Table 2 Risk of incident adverse renal outcomes for baseline remnant-C levelsThe linear or nonlinear relationship between remnant-C and adverse renal outcomesIn this study, we aimed to elucidate the linear or nonlinear relationship between remnant-C and various adverse renal outcomes. To achieve this, we employed restricted cubic spline analysis to explore the associations. Our findings revealed that there was a linear relationship between remnant-C and worsening renal function (P for nonlinear = 0.2760) and renal faiure (P for nonlinear = 0.9784), as depicted in Fig. 2. However, in the case of albuminuria, we observed a nonlinear relationship (P for nonlinear = 0.0237). This implied that the risk of this particular adverse renal outcome does not follow a consistent linear pattern but rather exhibits a more complex relationship with remnant-C levels.
Fig. 2
The linear or nonlinear relationship between remnant-C and adverse renal outcomes by performing Restricted cubic spline analysis. (A) Albuminuria; (B) Worsening renal function; (C) Renal failure
Sensitivity analysesThe association between remnant-C and the risk of adverse renal outcomes in sensitivity analyses remained robust. A consistent association was observed when (1) excluding 2747 patients who had used fenofibrate at baseline (Figure S1 and Table S1); (2) excluding 3586 patients who had a history of CVD at baseline (Figure S2 and Table S2); (3) Furthermore, after education levels, BMI, duration of diabetes, alcohol consumption status, smoking status, systolic pressure, diastolic pressure, HbA1c, UACR were imputed, the results remained consistent after imputation (Table S3).
留言 (0)