Our case series demonstrates that PH severity improved in 54% and 72% of neonates after 1 and 2 weeks of bosentan treatment, respectively. Even non-responders demonstrated a significant improvement of PH severity after 2 weeks of treatment (p = 0.029). The study also reveals a significant improvement in the RVD/LVD ratio, which normalized in 55.3% after 1 week and 67.4% after 2 weeks of bosentan treatment. Based on the study design and dynamic changes in the individual treatment, it is not possible to conclusively link the improvement in the RVD/LVD ratio to bosentan treatment alone. However, a presumed decrease in the pulmonary arterial pressure might be associated with a normalization of morphological changes such as RV dilatation or ventricular disproportion. This is supported by the finding that non-responders demonstrated a significantly higher RVD/LVD ratio after 2 weeks of treatment. In terms of respiratory outcome; 8 patients showed improvement after 1 week, and an additional 9 patients improved after 2 weeks. Irrespective to responder or non-responder, the respiratory status improved in both groups over the course of 2 weeks. The need for ECMO therapy declined, with no patients receiving ECMO after 2 weeks. However, a risk of overestimating the therapeutic effect of bosentan persists, as 8 patients were still on ECMO at 1 week after starting bosentan.
To our knowledge, this is the first retrospective study investigating the effect of adjunctive bosentan therapy on the clinical course in CDH neonates. In the past, inhaled nitric oxide (iNO) and intravenous sildenafil have been widely used to treat CDH-PH, but not all patients respond sufficiently. This is often due to the underlying pathophysiology of the lung, insufficient lung recruitment, hyperinflation and differences in LV dysfunction and shunting. Current treatment of CDH-PH often relies on clinical experience rather than evidence from RCTs. Although a few case reports and exploratory RCTs on the effect of bosentan in newborns with PH have been published, these studies primarily included PPHN or preterm premature rupture of membranes (pPROM). A recent systematic review by Gao et al. [26] of nine RCTs and one retrospective study on the effect of bosentan in the treatment of PPHN revealed mixed results. While early trials showed favourable responses without any adverse events, the lack of iNO or ECMO therapy in some trials and the small sample sizes limit the strength of these findings [18]. Bosentan as an endothelin-1 receptor antagonist is however suggested as a potential therapeutic option for CDH-PH by following research showing that dysregulation of ET-A receptors and elevated ET-1 may contribute to CDH-PH. ET-1 acts as a potent pulmonary vasoconstrictor by binding to endothelin-A (ET-A) and endothelin-B (ET-B) receptors. ET-A receptors, located on vascular smooth muscle cells, cause vasoconstriction, whereas ET-B receptors mediate vasodilatation [6, 10]. De Lagausie et al. and Mous et al. have shown a significant overexpression of ET-A and ET-B receptors in the lungs of CDH patients or newborns with PPHN, with a predominance of ET-A compared to ET-B receptors [5, 11]. Additionally, higher ET-1 plasma levels have been associated with higher disease severity and poorer outcome in CDH neonates [12,13,14]. Contrary to the abovementioned echocardiographic findings and respiratory status, we observed only minor changes in oxygenation status and ventilator settings. Several physiological and clinical factors could explain this, such as the transition from more invasive to less invasive respiratory support, which might increase FiO2 requirements despite the improved PH. The OI as a useful marker of oxygenation status is limited to neonates receiving mechanical ventilation. When transitioning to less invasive modalities such as CPAP, this index cannot be applied. Further, the preexisting underdeveloped alveolar structures and pulmonary vasculature inherent to CDH may be limiting gas exchange capacity even if the PVR decreases. Also, prolonged mechanical ventilation can induce ventilator-associated lung injury, resulting in impaired gas exchange, even after ventilator support is de-intensified. Bosentan and other pulmonary vasodilators could potentially worsen oxygenation by reducing hypoxic pulmonary vasoconstriction (Euler-Liljestrand mechanism) [4]. These agents may increase blood flow to under-ventilated or non-aerated areas of the lung, which increases intrapulmonary shunting and reduces the efficiency of gas exchange, leading to higher FiO2 requirements despite improvements in PH. Thus, while PH is improved due to reduced PVR, the mismatch between ventilation and perfusion is exacerbated, contributing to the lack of improvement in oxygenation. Although the difference of patient’s characteristics including foetal markers of CDH severity were not significantly different between responders vs. non-responders, factors such as lower o/e LHR, intrathoracic liver, less isolated forms of CDH and a lower gestational age at birth might have had a cumulating effect on the disease course. This may result in a higher degree of lung hypoplasia and more aberrant pulmonary vascular development among non-responders, which could cause a lower response rate to bosentan therapy. Our dosage of 2 mg/kg/day aligns with previous literature, but recent findings suggest that up to 5 days of dosing may be required to reach therapeutic levels [18, 22, 26, 27]. This supports our observation of minimal response within the first 72 h after starting bosentan. Pharmacokinetic variability between patients may further explain the difference in response rate, as we were unable to measure bosentan levels in our cohort.
The observation that significantly fewer responders were discharged on bosentan compared to non-responders can likely be explained by the practice of weaning responders to sildenafil monotherapy after achieving clinical improvement. In the responder group, bosentan was discontinued earlier following significant improvements in clinical condition and echocardiographic findings. In contrast, bosentan was often continued in non-responders due to a lack of improvement or was administered until death. A notable limitation of this study is that bosentan therapy was not consistently discontinued in cases where no response was observed after 2 weeks of treatment. The duration of ECMO support, mechanical ventilation, and hospital stay did not differ significantly between responders and non-responder. This lack of significant difference could be influenced by other contributing factors beyond elevated PVR, such as lung injury from prolonged ventilation and lung hypoplasia, opioid withdrawal syndrome or feeding difficulties.
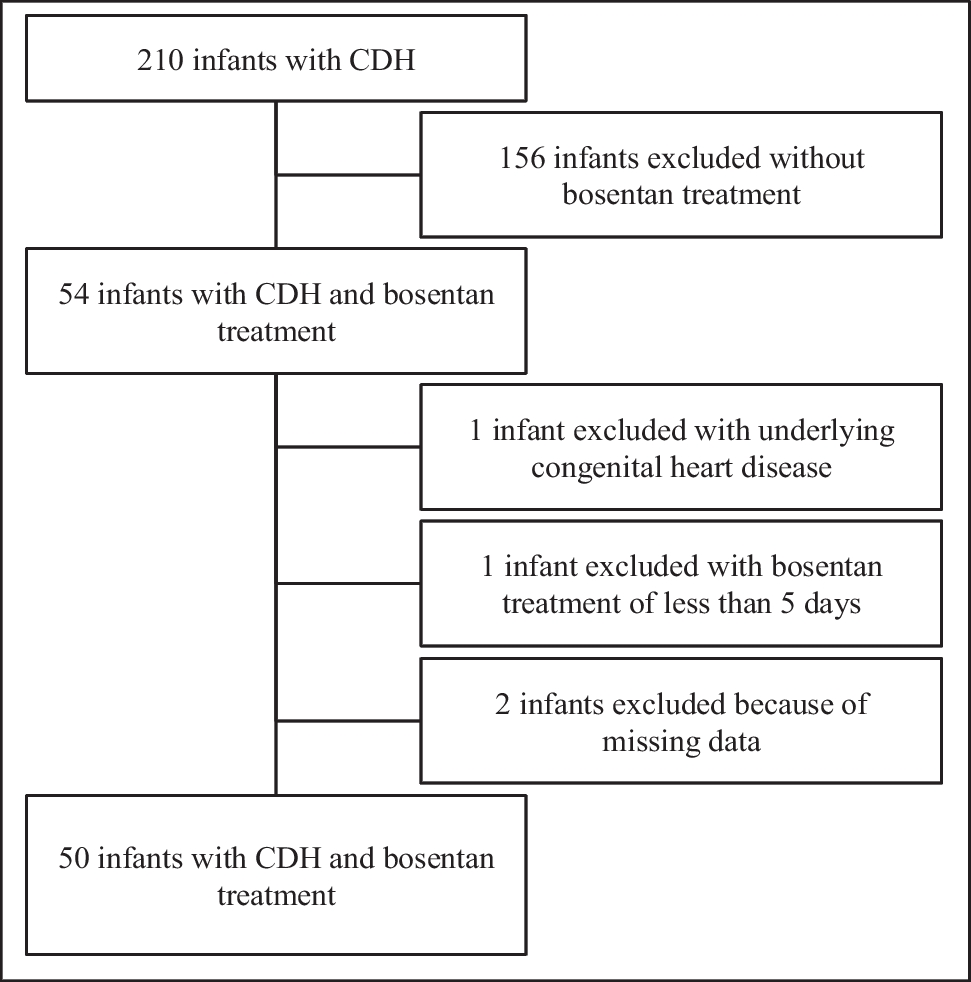
This cohort was highly selective, as only 54 of 210 (25.7%) CDH newborns at our institution received bosentan, resulting in a relatively high mortality rate of 42% in the study cohort, despite a reduction in ECMO use. This discrepancy indicates that mortality was primarily caused by underlying pulmonary pathophysiology or other causes of death, for which extended ECMO support would not have improved survival. Notably, no patients in this cohort required a second ECMO run. The elevated mortality rate among the 27 patients (54%) who responded favourably to bosentan therapy may be attributed to factors unrelated to PH, including chronic ventilator-induced lung injury, lung hypoplasia or cardiac dysfunction. Importantly, responders and non-responders were classified based on improvement of PH after 1 week of therapy; later improvements, which may take longer to manifest, were not evaluated. In an attempt to quantify LV dysfunction, we compared the LV-GLS between responders and non-responders at baseline and after 1 week of treatment. Although an abnormal LV-GLS demonstrated LV dysfunction in 25.9% of responders and 39.1% of non-responders at baseline, this difference was not statistically significant. Whether, LV dysfunction may contribute to non-responding to bosentan in CDH neonates, as it has been described in other pulmonary vasodilators such as sildenafil or iNO, needs to be investigated in future trials. However, in most patients LV dysfunction was not severe, presumably not contributing to increased mortality. Finally, 44% of the neonates in this cohort had non-isolated CDH with varying comorbidities, such as DiGeorge syndrome, ventricular septal defect or pulmonary sequestration, all of which could have contributed to the elevated mortality rate.
Common adverse effects of bosentan include elevated LFT, liver failure, anaemia, leukopenia and thrombocytopenia [28]. However, it remains unclear if this was drug-related or due to other factors, such as sepsis or liver bleeding. No patients discontinued treatment due to adverse effects, suggesting a consistent safety profile with previous studies [18,19,20,21,22]. This study is limited by its retrospective design, small sample size and single-centre setting, which may reduce statistical significance of our findings. Additionally, we did not routinely measure ET-1 level or cardiac biomarkers such as proBNP, which have been associated with disease severity in CDH neonates [14, 29]. Furthermore, the lack of a control group receiving alternative therapies or no bosentan therapy limits our ability to compare outcomes directly. Neonates in this study received bosentan predominantly for moderate to severe PH, which introduces potential selection bias. Differences in disease severity or treatment eras likely influenced the decision to use bosentan, making direct comparisons with non-treated patients difficult and subject to confounding factors. Another important limitation is the potential for natural improvement in PH and respiratory status in some patients, independent of bosentan therapy. This possibility highlights the inherent limitations of retrospective case series in determining treatment efficacy. Although bosentan is generally well-absorbed, variability in feeding schedules and gastrointestinal function in neonates with CDH may have impacted the bioavailability of the drug, leading to inconsistent responses among the study population. Lastly, the timing of bosentan initiation could have influenced response rates, particularly in relation to the surgical CDH repair. While this cohort received bosentan early, the exact timing relative to hernia repair (pre- or post-repair) was not standardized and may have contributed to differences in outcomes. Earlier initiation of bosentan, potentially before repair, may have the potential to reduce the need for ECMO more, though further investigation is needed to clarify this hypothesis.







留言 (0)