Design
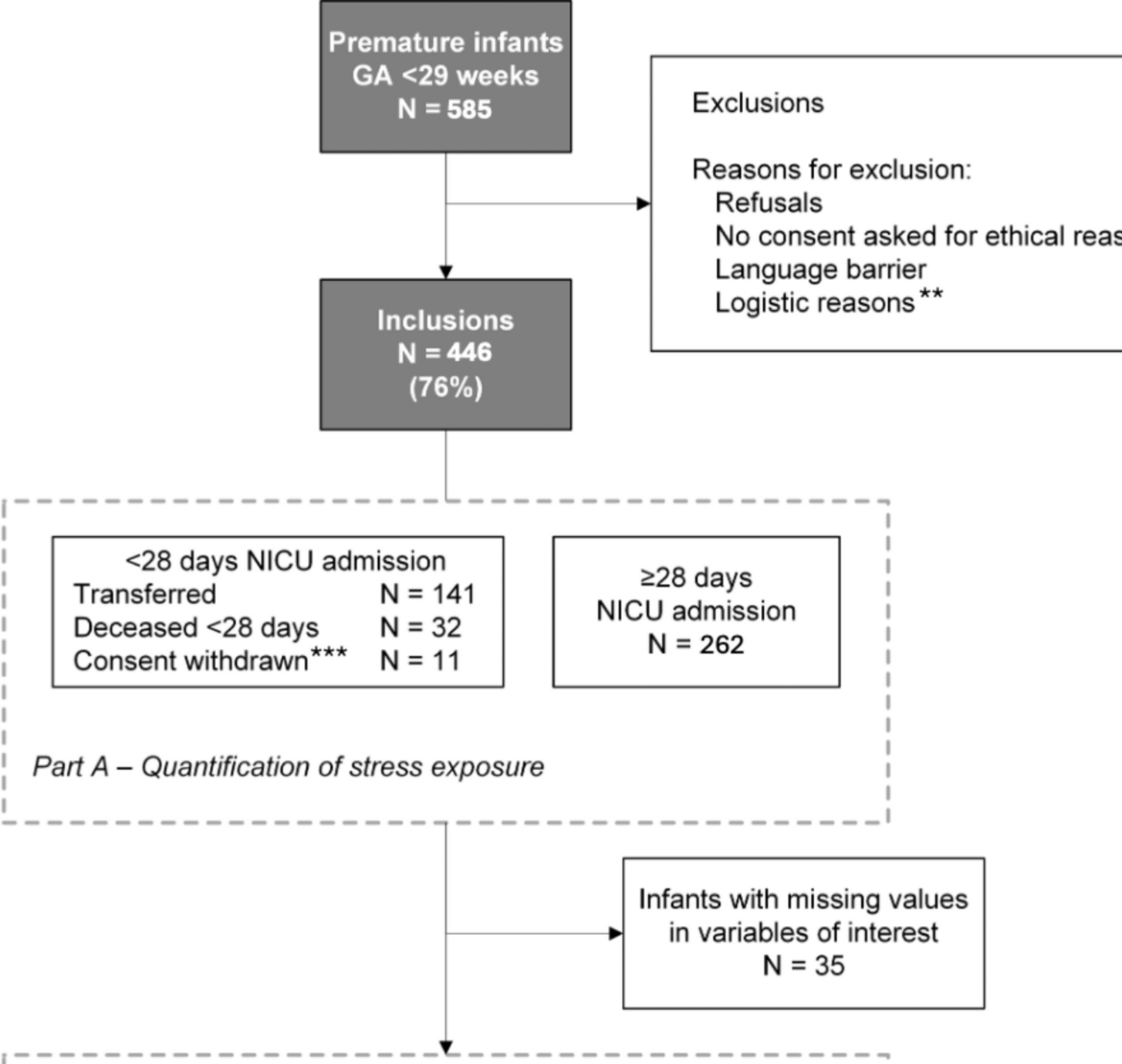
This national multicentre observational cohort study (Happiness for the Improvement of Premature and Parental outcome — HIPPO study, Dutch trial register NL8939) followed preterm infants prospectively during their NICU admission. Data collection for all eligible patients started immediately after birth (day 1) and continued until the 28th day of life, since most stressors occur during this period. Moreover, most children are transferred to a post-NICU centre from a gestational age of 30 weeks onwards. Parents were informed about this study as early as possible. Data collection stopped before day 28 if parental consent was not granted or after death or NICU discharge.
Patients and setting
All preterm infants born at a gestational age below 29 weeks admitted to one of all 10 level III/IV NICUs across the Netherlands were eligible for inclusion. This cut-off for gestational age was chosen since infants may leave the NICU from a postmenstrual age of 30 weeks onwards. With an average of 600 to 700 preterm infants with a gestational age below 29 weeks admitted to Dutch NICUs annually, we aimed to include at least 400 infants.
Since NICUs started patient enrolment at different times, the total inclusion period spanned from July 1, 2020 until March 1, 2022, with each NICU having a 1-year inclusion period. Infants were recruited by the local research team and excluded only if parents could not read the written information (Dutch, English, Turkish, Arabic or Polish).
The medical ethical committee of the Erasmus MC waived the requirement for approval under Dutch Law on research with humans (MEC-2019–0574), as the study was deemed non-interventional and did not subject infants to procedures or additional behavioural rules. The medical ethical committees of the other participating NICUs subsequently adhered to this decision.
Data collection
All data were entered in Castor® Electronic Data Capturing system (Amsterdam, the Netherlands) by the local research teams, an online database that complies with Good Clinical Practice (GCP) guidelines.
NeO-stress score
We developed the NeO-stress score in preparation of the current study to gain insight into a preterm infant’s stress exposure and estimate the cumulative amount of stress [13]. Different instruments have been developed previously to quantify stress exposure. However, none of these instruments have been validated for NICU populations outside the US or Australia, and regarding face validity, Dutch NICU nurses and physicians were of the opinion that existing instruments such as the “Neonatal Infant Stressor Scale” (NISS), “Procedural Load Index” (PLI) and “Accumulated Pain/Stressor Scale” (APSS) [1, 14, 15] did not match their current clinical practice. We therefore developed an instrument to quantify very preterm infants’ daily cumulative stress level during the first 28 days of life. In brief, NICU professionals across the Netherlands scored the relevance and comprehensibility of 77 potentially stressful items as well as the comprehensiveness of the item list. Calculating the content validity per item (CVI-I) resulted in a list of 38 relevant items, of which 34 had a CVI-I if 0.78 or higher. One of these items was split into two items, and three items were added to improve comprehensiveness. In a second round, the participants rated the stressfulness of the items from 0 (not stressful) to 10 (extremely stressful). A stressfulness index — representing the median score — was calculated for each included item [13] (SI, see supplement 1). The NeO-stress score is calculated per day by multiplying the number of times each stressor occurred by the SI (NeO-stress = Nitem1 × SIitem1 + Nitem2 × SIitem2 + etc.) [13]. The stressors were registered prospectively in a study diary by the health caregivers or retrieved from the electronic health record system.
Since “Continuous Positive Airway Pressure (CPAP) respiratory support” accidently did not receive a SI in our initial instrument development study, we calculated the median SI for non-invasive respiratory support based on the rating of 12 nurses and 13 physicians from all Dutch NICUs and added this item to the NeO-stress score (non-invasive respiratory support for 24 h = SI 6).
Infant characteristics
Infant characteristics included gestational age, birthweight, sex, small for gestational age (< 10th percentile, Fenton 2013 growth charts[16]), inborn/outborn, singleton/twin/triplet and 5-min Apgar score. Maternal characteristics (antenatal administration of corticosteroids, magnesium sulfate (MgSO4) and smoking during pregnancy) were retrieved from patient records. We recorded the type of NICU admission: single beds (2 NICUs) or open bay (8 NICUs).
Statistical analysis
Infants’ characteristics are presented as median and interquartile range (IQR) for continuous non-normally distributed variables and as the number of participants (percentage) for categorical variables.
Part A — quantification of stress exposure during NICU admission
We calculated the cumulative NeO-stress scores per day per infant. In order to determine the contribution of each individual stressor, for each item we multiplied the number of times the item occurred during the first 28 days by the SI (Nitem × SIitem) and divided this score by the total cumulative NeO-stress score during the admission days (maximum 28 days).
Part B — factors associated with the level of stress exposureB.1 Infant characteristics associated with the level of stress exposure
a.
Linear mixed-effects modelling was applied with the NeO-stress scores per day as the outcome variable and infant and maternal characteristics as predictor variables based on their judged clinical relevance (Model 1). A random intercept and slope per infant were included in the model together with an AR(1) covariance matrix to account for within-infant correlations. Infants with missing data were excluded since these data might be missing not at random.
b.
The interaction term of postnatal age and gestational age was added in Model 2 in order to examine whether the change in stress exposure over time varied between infants of different gestational ages. Possible nonlinear effects of postnatal age and gestational age were assessed by including natural cubic splines of these variables. Because the spline variables did not improve the model fit, only linear terms of postnatal age and gestational age were retained in the final model.
B.2 Differences in stress exposure between NICUs
The unit of admission and the unit type (open bay or single bed unit) were separately added as predictor variables to the final model in Models 3 and 4, respectively. This enabled us to compare the differences in NeO-stress scores, taking into account the possible differences between units with respect to the infant characteristics included in the model.
A p-value < 0.05 was considered statistically significant in all analyses. Data were analysed using IBM SPSS Statistics for Windows, version 27.0. Armonk, NY and R version 4.2.1 with the nlme package (version 3.1–157) to estimate linear mixed models.







留言 (0)