Our study revealed that patients with T1D who also had metabolic syndrome experienced greater glycemic variability and higher levels of hyperglycemia in free-living condition, as demonstrated by CGM metrics. Even after adjusting for potential confounding factors, metabolic syndrome remained significantly associated with increased MG, TAR, SD, and IQR.
As the rates of overweight and obesity have increased in the T1D population [8, 9], the prevalence of metabolic syndrome seemed to follow this trend [2, 10,11,12]. Previous research has identified several characteristics associated with metabolic syndrome, including older age, female sex, longer diabetes duration, and higher insulin dosages [5, 8, 13]. Our study also suggested that participants with metabolic syndrome were generally older, predominantly female, had a longer duration of diabetes, and required higher insulin dosages. While previous studies comparing beta-cell function in individuals with and without metabolic syndrome have yielded inconsistent results [14, 15], our study found that beta-cell function, as indicated by fasting C-peptide levels, was similar between the two groups.
The presence of metabolic syndrome in T1D patients was associated with poorer glycemic control and a higher incidence of complications. Previous studies have shown a connection between metabolic syndrome and elevated HbA1c levels [3, 5, 13]. Our research, utilizing CGM data, further confirmed that metabolic syndrome was associated with unsatisfied glycemic control, suggested by higher TAR and increased glucose variability. Metabolic syndrome in T1D patients was associated with a higher risk of both macrovascular and microvascular complications [3, 5, 6, 13, 15,16,17,18,19]. While the role of insulin resistance and metabolic syndrome in the development of cardiovascular diseases was well established in type 2 diabetes [20,21,22], it was also associated with an increased likelihood of macrovascular complications in T1D [8]. Even with good glycemic control, T1D patients with metabolic syndrome showed a higher prevalence of macrovascular complications such as stroke, peripheral arterial disease, and diabetic foot syndrome compared to those without metabolic syndrome [8, 23]. Meanwhile, there was a higher prevalence of diabetic nephropathy and retinopathy in T1D patients with metabolic syndrome [5, 8, 23], which was also observed in our study. This highlighted the importance of considering patients’ overall metabolic health, beyond just glucose control, to mitigate the risk associated with metabolic syndrome and complications in T1D.
Our study demonstrated that metabolic syndrome is associated with an increased risk of diabetic nephropathy in individuals with type 1 diabetes, suggesting that metabolic syndrome may contribute to the progression of diabetic nephropathy. Previous research has indicated that dyslipidemia is linked to diabetic nephropathy [24, 25]. The underlying mechanisms may involve abnormal lipid accumulation, which can damage podocytes, proximal tubular epithelial cells, and renal interstitial tissues through processes such as inflammation, mitochondrial dysfunction, autophagy impairment, endoplasmic reticulum stress, and apoptosis [26,27,28,29]. Therefore, in the long-term management of T1D, it is essential to adopt an integrated approach that emphasizes the comprehensive management of glycemic levels, lipid profiles and blood pressure.
As previously reported, remnant cholesterol in T1D has been linked to reduced TIR, increased TAR, and a higher prevalence of diabetic nephropathy and severe diabetic retinopathy [24, 25]. Our study also observed that metabolic syndrome in T1D was correlated with higher TAR and an increased prevalence of diabetic nephropathy. These results suggest that lipid metabolism abnormalities, including elevated remnant cholesterol, may play a role in the development of diabetic nephropathy in T1D. Further research is needed to validate these associations.
Our study revealed that, consistent with previous research [30,31,32], TAR was associated with metabolic syndrome in free-living conditions. Since increased TAR was linked to both long-term microvascular and acute complications [33,34,35], the observed higher TAR in individuals with metabolic syndrome may partly explain their association with a poorer prognosis. However, another study conducted on Chinese individuals with T1D found no significant difference in TAR between the metabolic syndrome group and the non-metabolic syndrome group after adjusting for age, sex, and duration of diabetes [15]. This discrepancy may be attributable to the fact that the participants in that study were instructed to adhere to a structured lifestyle intervention, which included regular dietary habits and physical exercise, whereas the participants in our study were observed under free-living conditions. In a study with 547 participants with T1D, it was shown that those in the obesity/overweight group were associated with a lower CV [30]. However, in a study conducted in Greece with 73 T1D participants, glucose metrics indicating variability were similar in obese individuals [36]. Another study conducted on Chinese individuals with T1D suggested that CV was higher in T1D patients with metabolic syndrome after adjusting for age, sex, and duration of diabetes using nearest neighbor matching [15]. Moreover, a study involving 895 children and youths with T1D found that obesity was associated with a higher CV [37]. Further research is necessary to elucidate the causal relationship between glycemic variability and metabolic syndrome in T1D patients.
As hyperglycemia and glucose fluctuation were the primary challenges in the glucose profiles of T1D individuals with metabolic syndrome, treatment strategies focusing on these two factors should be prioritized. Despite advancements in technology, such as artificial pancreas systems, insulin dosage guidance systems, and novel insulin formulations [38,39,40,41], there remain significant unmet clinical needs in the management of patients with T1D. Our findings demonstrated that TAR was strongly correlated with diabetic complications and was associated with metabolic syndrome in T1D. These results underscored the critical importance of comprehensive long-term management strategies, including medical nutrition therapy, individualized meal planning strategy, and appropriate physical activity, to achieve favorable outcomes in T1D care. Furthermore, proper lifestyle management remained crucial and fundamental for T1D management. This included regular physical activity and personalized medical nutrition therapy. For individuals with metabolic syndrome, higher glucose variability often reflected inadequate meal planning and insufficient physical activity [8, 9, 42,43,44,45,46,47], which were key contributors to the development of metabolic syndrome. Therefore, for T1D patients with metabolic syndrome, comprehensive diabetes education should be emphasized. This education should focus on empowering patients with the knowledge and skills necessary to effectively manage their condition through lifestyle modifications.
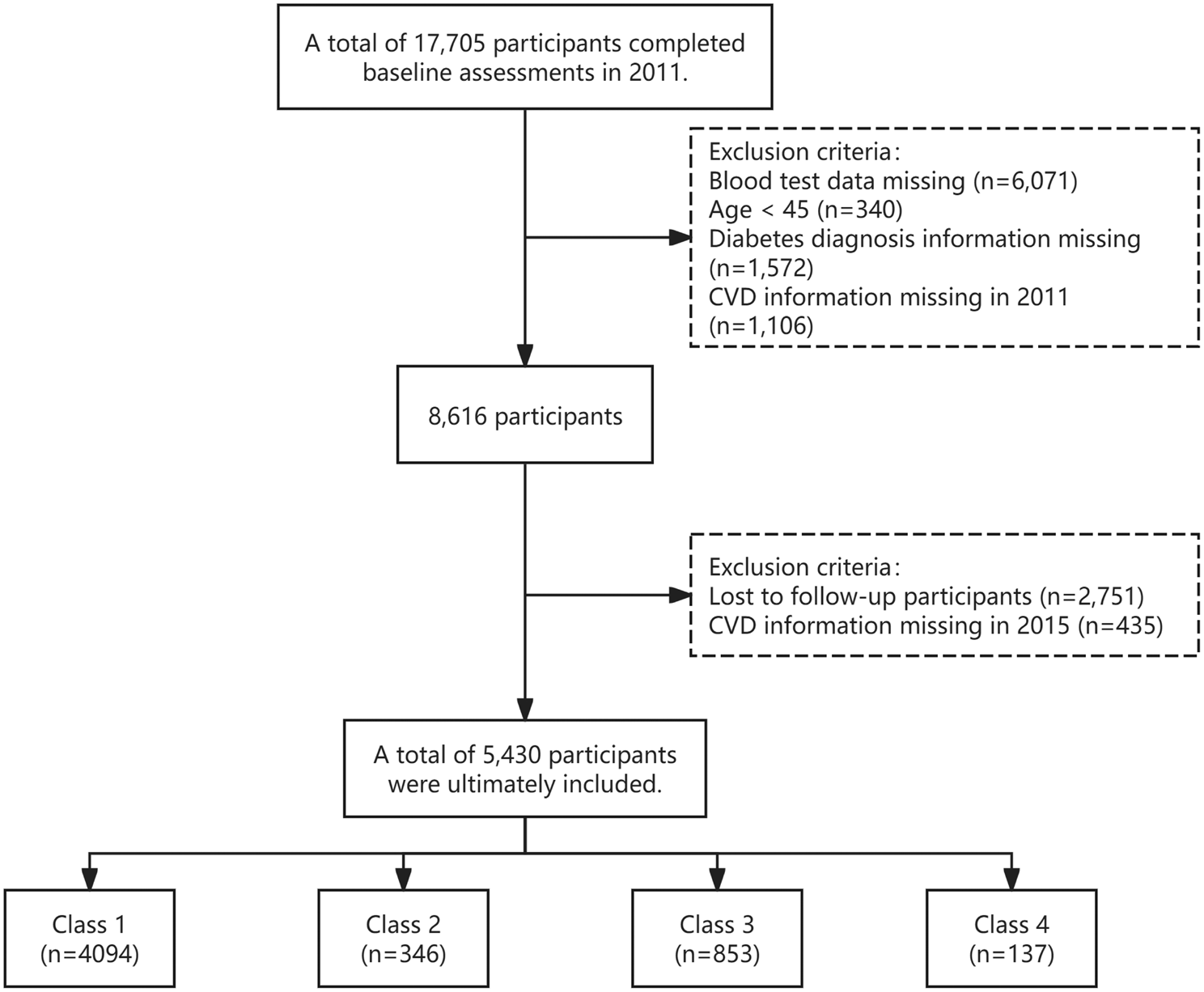
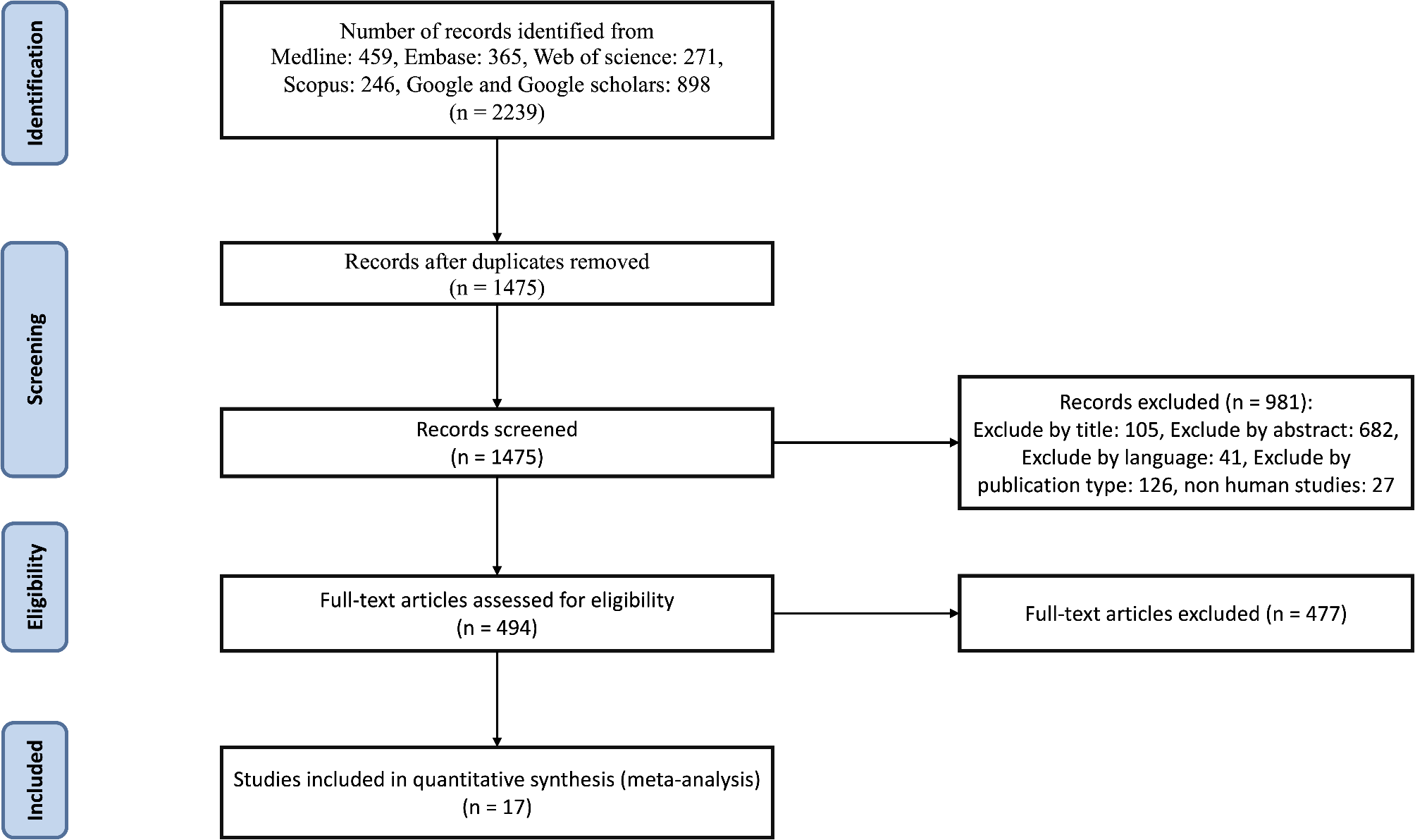
Our study had several limitations. First, as a cross-sectional study, it could not establish causality between CGM metrics and metabolic syndrome. Further prospective studies are needed to clarify the relationship. Second, this was a single-center study with a relatively small sample size, highlighting the need for multi-center studies in diverse settings to validate our conclusions. Third, over five hundred participants were excluded due to insufficient CGM data or missing information necessary for assessing metabolic syndrome, which might introduce selection bias.

留言 (0)