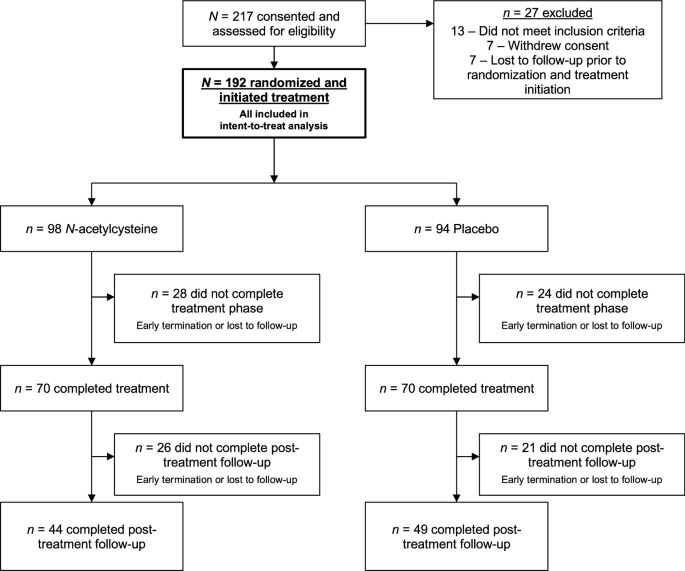
Study design and participants
This randomized, double-blind, placebo-controlled, parallel-group study included a screening period of up to 4 weeks, a 12-week treatment course, and follow-up through week 26 from randomization, with post-treatment visits at approximately weeks 16 and 26. The study received Medical University of South Carolina Institutional Review Board approval and was conducted in accordance with the Declaration of Helsinki and the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use and Good Clinical Practice guidelines. Study outcomes were pre-registered on clinicaltrials.gov (NCT 03055377). The 2400 mg/day dosage of oral N-acetylcysteine, administered as 1200 mg twice daily, was selected based on prior positive findings with this dosage combined with contingency management [11]. Participants ages ≥18 provided written informed consent. Written parental consent and participant assent were obtained for those <18 years old. Eligible participants were ages 14–21, met DSM-5 criteria for cannabis use disorder within the last 30 days, expressed interest in cannabis use disorder treatment, and submitted a urine sample positive for cannabinoids (> 50 ng/mL). Individuals currently enrolled in cannabis use disorder treatment, with moderate or severe substance use disorders aside from cannabis or nicotine/tobacco, with current (past 30 days) or planned synthetic cannabinoid use, pregnant or lactating, currently prescribed carbamazepine or nitroglycerin, with seizure disorder or uncontrolled severe asthma, or with acutely unstable medical or psychiatric disorders were excluded.
Participants self-reported baseline motivation, readiness, and confidence to quit using cannabis (all on a 1–10 scale, with 1 = “not” and 10 = “extremely”) and were randomized in 1:1 ratio to N-acetylcysteine or placebo, stratified by age (≤18 versus ≥19) and by nicotine use status (assessed via Clinical Laboratory Improvement Amendments of 1988 [CLIA]-waived point-of-care urine cotinine test, with cutoff of <50 ng/mL signifying a cotinine-negative sample and thus categorizing into the non-nicotine-use group). A stratified random block design was utilized with random block sizes of 4 and 6. The randomization schedule was developed by the study statistician prior to initiation of enrollment, using a blinded allocation (A/B), and the investigational pharmacy randomly assigned active NAC and placebo treatment to A/B assignments. Participants, clinicians, and study personnel were blind to treatment allocation throughout the study.
Procedures
United States Pharmacopeia (USP) grade N-acetylcysteine powder was encapsulated in 600 mg quantities (two 600 mg capsules per dose). Matched placebo capsules were also prepared. All capsules were packaged and dispensed in blister packs, with individual labels for time/date of each dose. Participants were instructed to take two capsules (1200 mg) twice daily (total of 2400 mg per day), in approximately 12-h intervals; in the event of issues with tolerability, dose adjustments in increments of 600 mg were permitted at the discretion of the study medical clinician. Text messages prompted participants at the scheduled time for each dose, including a secure link for participants to upload a video recording of their medication-taking; study personnel reviewed participants’ uploaded videos to confirm adherence [14].
All participants received brief (typically <10 min) weekly medical clinician-delivered medical management and non-manualized skills-based cannabis cessation counseling (designed to match the intervention provided in the prior youth N-acetylcysteine trial, and to mimic what may be feasibly conducted in a busy clinical practice setting). The study, which included a hybrid of in-person and virtual visits, was conducted via a dedicated research clinic at the Medical University of South Carolina in Charleston, South Carolina.
Outcome measures
Urine cannabinoid testing at baseline, during weekly visits, and at post-treatment follow-up visits, was conducted as the primary biological measure of cannabis use. Participants self-reported cannabis use throughout the study via mobile technology-delivered daily surveys, including quantification of daily cannabis and other substance use [14]. Missing daily substance use data were filled via Timeline Follow-Back-like procedures at study visits [15].
Weekly urine samples were tested qualitatively with CLIA-waived point-of-care cannabinoid tests (cutoff of <50 ng/mL signifying a cannabinoid-negative urine sample) and sent to the laboratory for quantitative cannabinoid and creatinine testing to allow for evaluation of creatinine-normalized cannabinoid levels [16, 17]. For virtual visits, necessitated as an option due to COVID-19 related restrictions to in-person visits, qualitative urine cannabinoid tests were conducted remotely but laboratory quantification was not performed.
Primary efficacy was assessed as self-reported abstinence from cannabis use confirmed by urine cannabinoid testing (<50 ng/mL) during the 12 weeks of treatment, measured at weekly study visits. In addition to abstinence, weekly proportion of days using cannabis (frequency) and grams of cannabis used per using day (amount) were compared between study treatment groups [18].
Adverse events were assessed for severity and relatedness to study treatment by the medical clinician at all visits and coded in Medical Dictionary for Regulatory Activities (MedDRA) terminology by body system.
Study personnel reviewed participants’ uploaded medication-taking videos to confirm adherence; as part of medical management, the medical clinician addressed medication adherence during weekly visits throughout treatment. Adherence was assessed as the percentage of video-verified doses compared with the expected number of doses taken, summarized at each weekly visit (range 0–100%). A participant was considered medication compliant when taking at least 80% of prescribed doses.
Statistical analysis
A sample size of 67 participants per treatment group would provide 80% power with two-sided α = 0.05 to detect a group difference on the primary endpoint (proportion of negative urine cannabinoid tests); accounting for an anticipated 30% attrition rate, a sample size of 96 per group was deemed adequate for statistical power.
Participant baseline characteristics found to be significantly associated with cannabis use outcomes were included as covariates in adjusted model development. Self-reported 7-day point prevalence abstinence, cannabis use days, and cannabis use amounts were summarized at each weekly study visit as well as follow up visits. The main effect of N-acetylcysteine on negative weekly urine cannabinoid tests was assessed with a repeated measure log-linear regression using a general estimating equations framework (GEE). Models were computed using design covariates, including study treatment assignment, visit week, baseline cannabis use rates, and characteristics utilized in the stratification at randomization (age, urine cotinine resulting indicating nicotine use status). Working correlation structures were independently compared using the quasi-likelihood under the independence model criterion statistic [19]. All randomized participants were included in the primary analysis and assessed (1) using all available data and (2) with participants deemed non-abstinent at any missed visit (drop-out/loss-to-follow up included). Model based means were used to construct the pairwise comparisons of treatment groups. In addition to the longitudinal analysis of negative urine cannabinoid tests and 7-day point prevalence abstinence rates during treatment, rates were compared between treatment groups at each post-treatment follow-up visit using logistic regression models. Summary results are presented as means and standard deviations, while model-based results are presented as risk ratios (RR) and associated 95% confidence intervals. Secondary cannabis use outcomes were (1) percentage of days using cannabis (frequency) and (2) grams of cannabis per using day (amount) between study visits during treatment, and were compared between study groups using linear mixed effects regression models. Assumptions of residual normality were assessed using QQ plots, and when deviations from normality were determined, data transformations were made (e.g. natural logarithm, square root). In addition to the primary analysis, modifying effects of sex assigned at birth on treatment efficacy were examined. When significant, stratified treatment efficacy estimates were estimated.
Penetration of the medication blind was assessed at the end of study treatment. Between groups assessment of blinding efficacy was conducted using Pearson’s Chi-Square test statistic, and data are reported as proportions correctly identifying their actual treatment assignment.
Treatment emergent adverse events are reported as the total number of events and frequencies for the whole cohort, as well as stratified by treatment assignment for all events that occur during study treatment.
Adherence (proportion of participants taking ≥80% of medication doses) was compared between randomized treatment groups using generalized linear mixed effects models with outcome specific distributions (logistic). Overall group differences, as well as differential adherence over time, were assessed through inclusion of a treatment group factor, a linear time factor, and the appropriate interaction.
All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA).




留言 (0)