
記住我





Case 1: A 42-year-old woman was observed with thrombocytopenia in a medical examination, which progressed to pancytopenia in 6 months. The bone marrow aspiration (BMA) yielded a marked hypocellular bone marrow, and flow cytometry (FCM) analysis performed on peripheral blood demonstrated CD55(−) CD59(−) granulocytes (approximately 2.3%) and red blood cells (approximately 0.6%). She was diagnosed with aplastic anemia stage 3 and received immunosuppressive therapy consisting of antithymocyte globulin (ATG), cyclosporine (CyA), and methylprednisolone (mPSL). Since then, she has been managed as an outpatient and received treatment with CyA and PSL. Her peripheral blood neutrophil and platelet count remain low (neutrophil: 0.5 × 109–0.8 × 109/L, hemoglobin: 60–80 g/L, platelet: 1.0–2 × 109/L). Two years later, she was admitted to our hospital due to poorly controlled anemia. Her reticulocyte counts, unconjugated bilirubin levels, and lactate dehydrogenase (LDH) activity had increased and haptoglobin levels had decreased (hemoglobin: 56 g/L, reticulocyte: 163,500/μL, unconjugated bilirubin: 1.8 mg/dL, LDH: 1674 U/L). FCM analysis performed on peripheral blood revealed CD55(−) CD59(−) granulocytes (approximately 28.5%) and red blood cells (approximately 21.8%, Fig. 1A). She was remitted from hemolysis immediately with a dose escalation of PSL. However, her pancytopenia prolonged, and a BMA performed 2 months later revealed approximately 4.3% myeloblasts of nucleated cells, multinucleated erythroblasts, and megakaryocytes of multiple, widely separated nucleated cells. Cytogenetics studies showed monosomy 7 in 20 metaphases analyzed, and she was diagnosed with MDS-refractory cytopenia with multilineage dysplasia (RCMD). Notably, the proportion of CD55(−) CD59(−) granulocytes and red blood cells decreased when she was diagnosed with MDS (Fig. 1A). The patient underwent unrelated bone marrow transplant. After engraftment, she has been managed as an outpatient. Two months post-transplant, she was admitted to our hospital due to severe diarrhea. Colonoscopy revealed mucosal sloughing and diffuse mucosal defect in the whole small intestine. She was diagnosed with Stage 3 gastrointestinal graft versus host disease (GVHD). No significant skin rash or liver involvement was observed, and she was diagnosed with Grade III acute GVHD. She received immunosuppressive therapy consisting of mPSL and beclomethasone. A bone marrow biopsy did not show relapse of MDS. 295 days after transplantation, she died from acute GVHD as well as a bacterial infection which arose during immunosuppressive therapy.
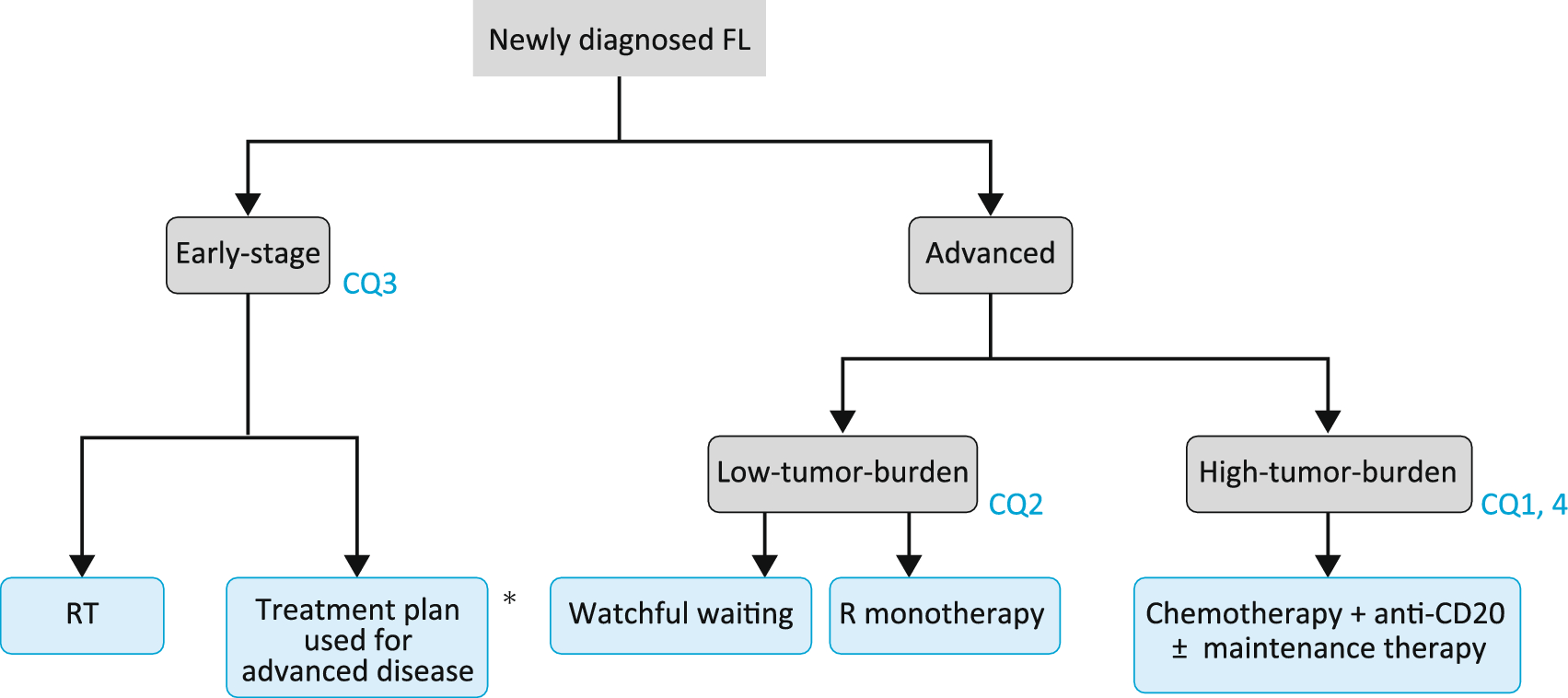
Fig. 1
The populations of CD55(−) CD59(−) PNH clones changes in phases between the types of the development. Flow cytometry dot plot analyses of peripheral blood samples from patients. A, C PNH clone size was determined by measuring CD55(−) CD59(−) CD235a(+) erythroid cells and CD55(-) CD59(−) CD11b(+) neutrophil cells. PNH clone size had diminished over the development to MDS in case1. MDS cells were thought to be derived from non-PNH clone cells as shown in the scheme. B, D 16.3% of CD235a(+) erythroid cells and 85.4% of the CD34(+) blast cells consisted of CD55(−) CD59(−) PNH clones. Acute erythroid leukemia was concomitant with PNH and leukemic blast cells were thought to be derived from PNH clone cells. FITC, fluorescein isothiocyanate; PE, phycoerythrin
Case 2: An 81-year-old man was observed with slight pancytopenia through an examination before surgery for lumbar spinal canal stenosis. His hemoglobin level was 129 g/L, white blood cell (WBC) count was 4.9 × 109/L, and platelet count was 12.9 × 109/L. General malaise and palpitations appeared from the next month, and he was referred to our hospital for further examination. His hemoglobin level was 81 g/L, WBC count was 2.1 × 109/L with 12.0% blasts, and platelet count was 6.2 × 109/L. BMA yielded a marked hypercellular bone marrow and erythroid dominance, representing approximately 47% myeloblasts of non-erythroid cells (NECs). Cytogenetic studies showed a complicated chromosome aberration: 45,X,-Y,−2,add(3)(p12),add(5)(q31),add(7)(q11.2),−9,add(15)(p11.2),+2mar in 12 of 20 metaphases analyzed. Furthermore, reticulocyte counts, unconjugated bilirubin levels, and LDH activity had increased and haptoglobin levels had decreased, suggesting intravascular hemolysis (reticulocyte: 89,800/μL, unconjugated bilirubin: 1.7 mg/dL, LDH: 1881 U/L). FCM analysis performed on peripheral blood demonstrated CD55(−) CD59(−) granulocytes (approximately 42%) and red blood cells (approximately 16%), consistent with paroxysmal nocturnal hemoglobinuria (PNH). Furthermore, 85.4% of the CD34-positive blast cells consisted of CD55- and CD59-negative PNH clones (Fig. 1B). The patient was diagnosed with concomitant PNH and acute erythroid leukemia. The patient received induction therapy with idarubicine (IDR) 12 mg/m2 1 day and cytarabine (AraC) 100 mg/m2 daily for five consecutive days. At 4 weeks after induction therapy, blasts in both peripheral blood and bone marrow had increased and determined non-remission status. The patient died from leukemic progression to cerebral infarction as well as a bacterial pneumonia infection which arose during induction therapy.
留言 (0)