
記住我








The analysis of practices revealed that only a few physicians, even those with expertise in pediatric hematology, have encountered children or adolescents with MPNs. The primary issue identified was the adaptation of MPN-specific treatments. Since MPNs are rare in children and clinical trials often do not include patients under 18, diagnostic and prognostic criteria have never been validated in the pediatric population, making the management of MPNs in young patients particularly challenging. In this study, the medical management of ET and PV varied significantly between centers and practitioners. A notable heterogeneity in the care provided was observed, particularly in terms of consultation frequency (Fig. 2). Physicians emphasized the need for training, but it is easy to see that shared learning and stronger collaboration between adult hematologists and pediatric experts could help practitioners manage young patients with ET and PV more effectively [6, 7].
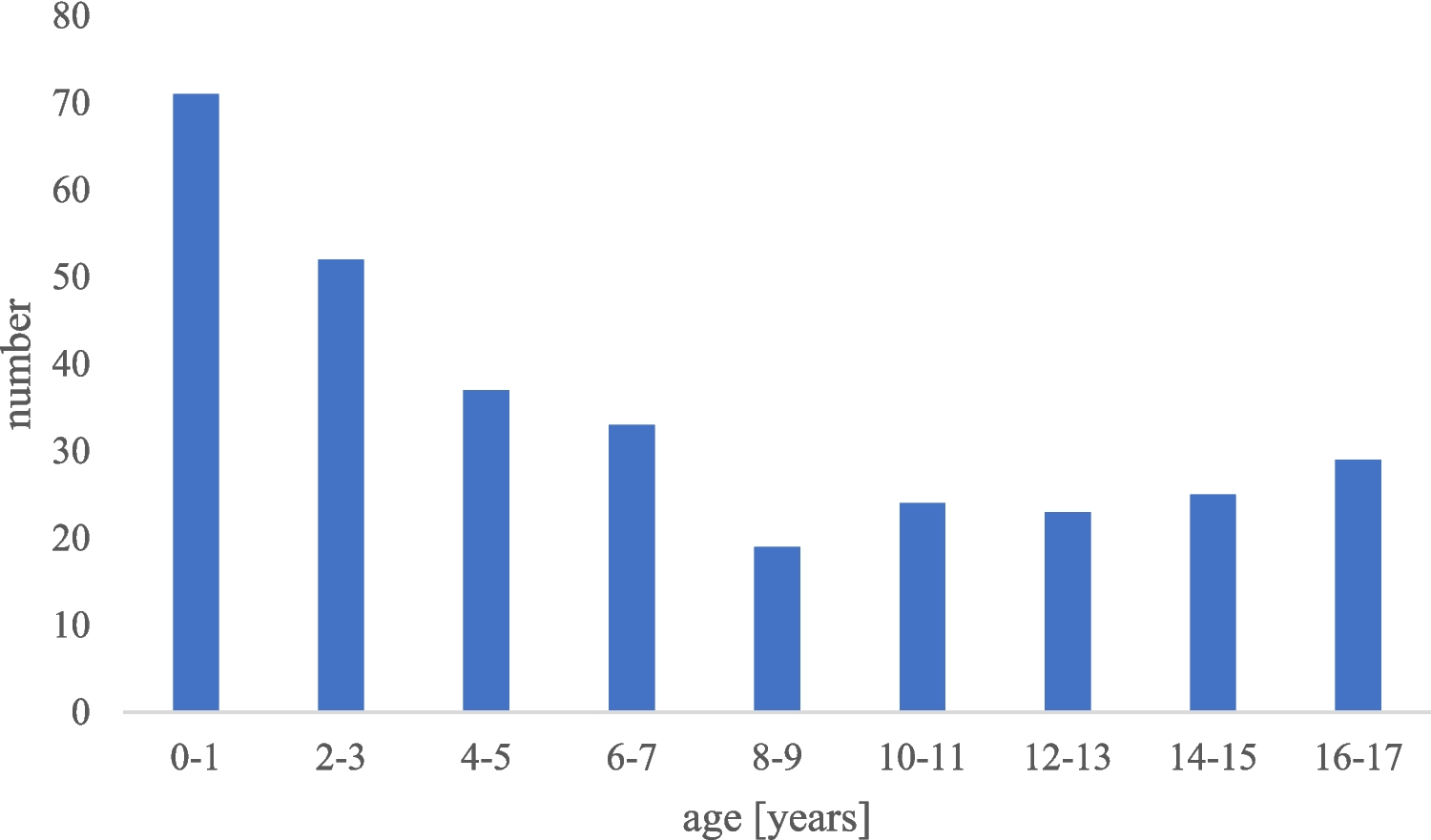
In our multicentric retrospective study, the median age at diagnosis was slightly younger than in previous studies [5, 8]. Almost half of children were asymptomatic at time of diagnosis, and the proportion of so-called triple negative patients was near to 50% as described in the literature [5, 8,9,10]. Without specific clinical symptoms for MPNs, diagnosis was made by chance in almost half of patients, so diagnostic delay was inestimable. Literature indicates that the majority of adult MPNs are associated with somatic mutations that lead to the constitutive activation of the JAK2-STAT5 pathway, with JAK2 V617F being the most common mutation. This mutation is found in ≥ 95% of PV cases and approximately 60% of ET cases [2,3,4, 11]. In line with existing pediatric literature, we observed a lower percentage of JAK2 V617F-positive patients [5, 8, 9], 35% (6/17), with variable allelic frequencies (ranging from 3.44 to 51.4%) in ET and PV, respectively [5, 8, 9]. Distinguishing between PV and JAK2-mutated ET can be challenging in pediatric cases [12]. Although histological analysis remains a key criterion for MPN diagnosis according to the WHO, only 60% of our French cohort underwent a bone marrow biopsy at diagnosis. Putti et al. highlighted the critical role of bone marrow biopsy in accurately diagnosing MPNs and ruling out other causes of thrombocytosis. Clinical and biological characteristics can overlap, and driver mutations are rarely found in this age group. In 2019, Kucine et al. proposed pediatric MPN diagnostic criteria based on the WHO classification, in which bone marrow biopsy remains a crucial element [12]. Based on these findings, we recommend that all patients under 18 with suspected ET or PV undergo bone marrow biopsy and driver mutation analysis. If no driver mutation is identified or if there is a family history of MPN, additional mutations should be explored through next-generation sequencing (NGS). The NGS panel should include all coding exons of the JAK2 and MPL genes, as rare non-canonical driver mutations can be detected in both MPN and constitutional thrombocythemia/polycythemia [13]. A proposed medical approach for pediatric MPNs is illustrated in Fig. 3.
Fig. 3
Proposal for an approach to manage pediatric MPNs
With a median follow-up of 45 months, no patient presented thrombotic complication (not taking into account patients with complications before diagnosis) and only one patient presented with recurrent epistaxis. On top of predominance for thrombotic venous events, Ianotto et al. [5] reported that the incidence of thrombosis during the follow-up was 9.3% for patients with PV, and 3.8% for those with ET. In the context of these chronic diseases occurring in young patients, only very prolonged follow-up (several decades) could enable the risks of complications to be established more precisely.
The treatment goals in pediatric MPN are to avoid thrombosis and bleeding, treat MPN-related symptoms, and minimize risk of malignant transformation. A relatively high frequency of initial prescription of “antithrombotic” drugs was observed despite the low number of high-risk patients, as defined on history of thrombosis and platelet count (over 1000 G/L) [4, 11, 14] and more than 50% of patients have been treated with a cytoreductive drug or related therapy (10/17, 58.8%). The reasons for prescribing these treatments were not explained. The hypotheses explaining these data could be: the unacceptable nature of persistent symptoms, even moderate in young patients, the apprehension of professionals regarding the risk of transformation, parent’s opinion… This study aims to better characterize the therapeutic indications in the future. Thrombocytosis > 1500 G/L or high elevation of hematocrit (teenage boy > 54%, teenage girl > 47%) [4] are proposed as an indication for treatment by European LeukemiaNet (ELN) but there is no data on a specific threshold for children and AYA. On top of literature, this study highlights that specific treatment such as antithrombotic and cytoreductive drugs (pegylated interferon) should be introduced only if the patient reports specific disabling symptoms, or suffers from complications (thrombosis or hemorrhage). Therefore, extreme thrombocytosis by itself, must not be seen as a formal therapeutic indication in young patients. Initiating a treatment has to be associated with specific precautions such as psychological evaluation before pegylated interferon, or fertility preservation before hydroxyurea. Because ET and PV are very rare conditions in the pediatric population, all newly diagnosed young patients should benefit from a multi-disciplinary meeting, gathering adult hematologists with expertise in looking after MPN and pediatricians to decide the best management and therapy. Our study is in line with relative literature and shows that complications in young patients are rare, and transformation is exceptional. In this case, it is essential to reassess therapeutic indications and discuss therapeutic de-escalations regularly.
In our population, the use of pegylated interferon seemed to be uncommon, compared to the first-line prescription of hydroxyurea. Hydroxyurea is effective in preventing thrombosis for high-risk patients with essential thrombocythemia [15] but could be associated with specific toxicities such as gonadotoxicity, acute leukemia, and myelofibrosis, with particular concern in young patients [12, 16, 17]. Interferon is known as a safe option in young patients and improves myelofibrosis-free survival [17]. Moreover, pegylated interferon has been reported to achieve a better molecular response compared to hydroxyurea. Pegylated interferon would therefore appear to be more appropriate as a first-line treatment for children and adolescents. Ruxolitinib is a JAK2 inhibitor approved for the treatment of PV in adult patients with intolerance or resistance to hydroxyurea treatment, regardless of JAK2 V617F mutational status, with well-known efficacy for splenomegaly, potentially reduction of vascular events, and complete molecular remission [18]. The use of ruxolitinib is well tolerated in the adult population, although side effects such as myelosuppression, hyperlipidemia, and risk of viral infections require surveillance and proactive preventive measures [19, 20]. In our cohort, only one patient with PV has been treated by JAK2 inhibitors after a decision in a multi-disciplinary staff meeting. No complication linked to PV or to the treatment was observed. Studies assessing ruxolitinib as treatment for intolerant or resistant children to interferon are needed.
Data concerning follow-up in our study revealed a great heterogeneity. Regular check-ups are required for young patients with ET or PV. Patients must also be warned about lifestyle risks, for example thrombohemorrhagic risks associated with smoking or hormonal contraception. Women with a child desire should be referred to a specialist and benefit from a specific follow-up. Resolution of symptoms, blood count normalization, toxicity, and complications should be followed for treated patients. Mutated allele burden has been validated as a prognosis factor in MPNs. Monitoring of JAK2, CALR, or MPL allele burden has been validated in several protocols following interferon, ruxolitinib, or stem cell transplant [18, 21]. In adult populations, a reduction in the mutated allele burden has been observed in response to various therapies, including interferon, JAK inhibitors, and stem cell transplantation. Although hydroxyurea fails to significantly reduce the JAK2 V617F allele burden, interferon has demonstrated the ability to achieve a sustained molecular response in patients with PV and ET [22]. Minimal residual disease or measurable residual disease (MRD) uses sensitive laboratory methods to find remaining abnormal cells among millions of normal cells after treatment. Initial studies on MRD assessment following JAK inhibitor therapy have reported modest reductions in mutational burden, despite significant improvements in patient survival in myelofibrosis [23]. However, growing evidence suggests that long-term therapy may lead to slow but complete molecular responses in some patients, underscoring the importance of extended MRD monitoring [24]. Thus, MRD evaluation could also be considered and linked to clinical evolution in pediatric cases of JAK2-mutated myeloproliferative neoplasms. Whereas the use of MRD in treatment adaptation needs to be further investigated, we propose monitoring variant allele frequency (VAF) in JAK2 V617F-mutated patients with sensitive techniques such as real-time quantitative PCR or digital PCR, when feasible. Controls of bone marrow smear or biopsy during follow-up should only be carried out in case of further disturbance of blood counts or new clinical symptoms (Fig. 3).
A diagnosis of a chronic disease at the age of 65 years carries a different significance than one made under the age of 18 years or younger, which is why care for young patients must be tailored to their unique needs. Attention must be given to the psychological well-being of both the patient and their family, medication adherence, as well as educational and career guidance in the context of living with a chronic disease. To improve care and follow-up for young patients, studies evaluating quality of life are essential and will be a key part of the ongoing research in this field. The development of specialized AYA units has significantly improved care for this age group in the context of other chronic diseases. Unfortunately, pediatric patients with MPNs do not currently have access to such specialized structures. Therefore, ongoing collaboration between pediatricians and adult hematologists is crucial for optimizing care and management.
留言 (0)