Patient cohort
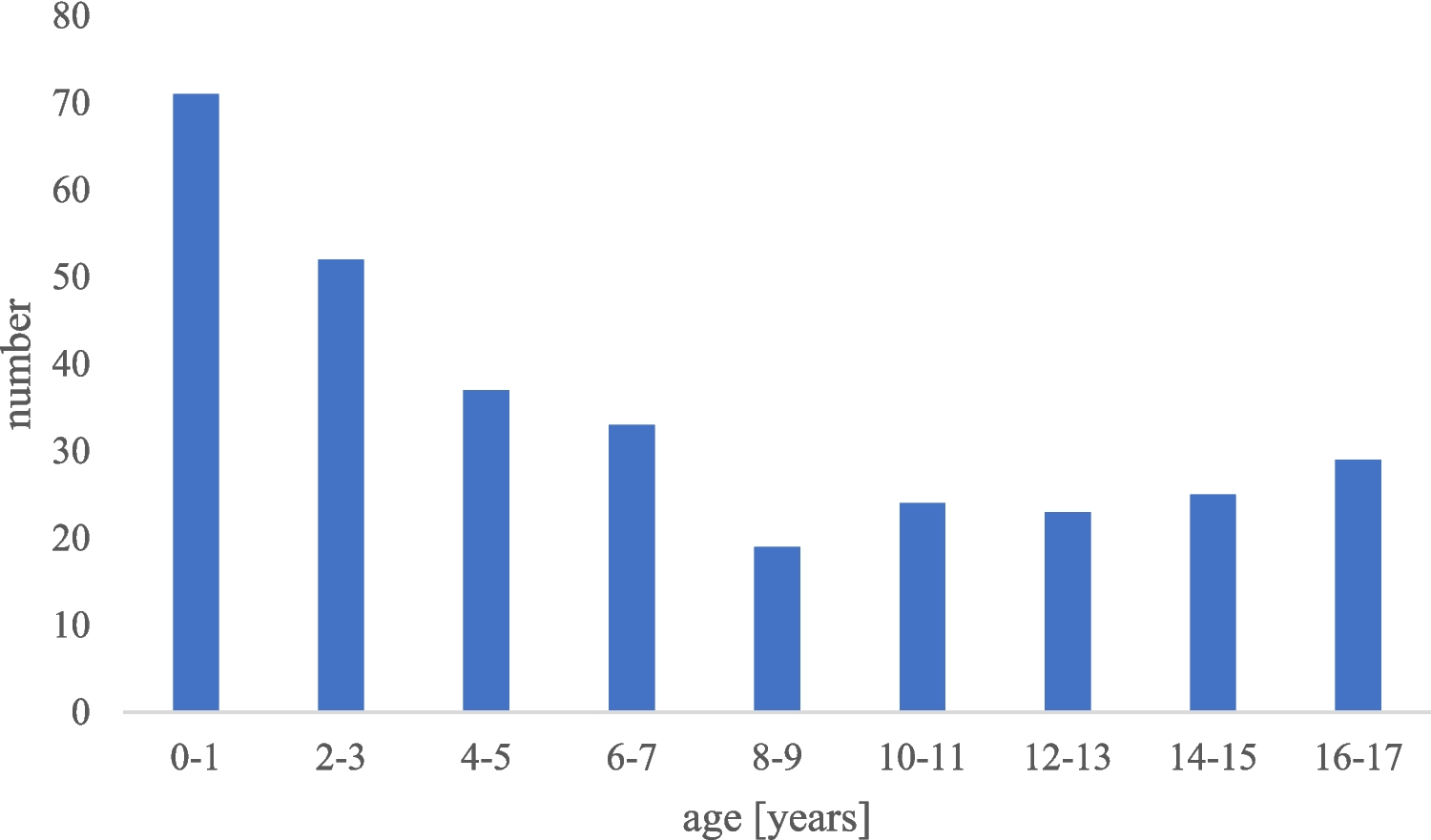
Patients below 18 years of age undergoing CVAD implantation for various reasons were eligible for inclusion.
CVAD systems and technique for vessel access
Single- or multiple lumen-tunneled central venous access devices (TCVADs), such as Broviac or Hickman catheters, Permcath, and completely implanted CVADs (Ports), were surgically implanted. Detailed analysis of CVADs included their material composition, presence or absence of antimicrobial coatings, and rationale for selection. In this study, only tunneled, surgically implanted CVADs such as Ports or Broviac catheters were included. Non-tunneled and peripherally inserted devices were excluded from the analysis. The procedures were performed under sterile conditions in aseptic operating rooms using mainly the following five venous access sites either through venous cutdown or percutaneous puncture following the Seldinger technique: internal jugular vein (via cutdown or puncture), external jugular vein (via cutdown), subclavian vein (via puncture), cephalic vein (via cutdown), or the anonymous vein (via puncture). Typically, a standard antibiotic, usually a first-generation cephalosporin, was administered within 30 minutes before the surgery.
Catheter tip position
A chest X-ray was performed immediately following every implantation of a CVAD. The catheter tip position was defined as previously described [1]. Briefly, two conventional methods were used to categorize the location of the catheter tip, namely either a categorical division based on the position of the catheter tip relative to the right main bronchus or a metrical division based on the position of the catheter tip relative to the carina. Both methods are described elsewhere in detail [1].
Data acquisition
This retrospective, single-center cohort study involved manual extraction of data from electronic medical records of pediatric patients with CVADs between 2021 and 2022. Demographic data, diagnosis specifics, implantation details (including CVAD type, caliber, and number of lumina), implantation techniques, venous sites, and catheter tip positions relative to anatomical landmarks were systematically collected.
The primary objective was to evaluate the impact of prior CVAD placements on complication rates. Other variables, such as catheter type, insertion technique, and patient demographics, were included as secondary analyses to control for potential confounders and provide a comprehensive risk assessment. Key data points included patient demographics (case number, birthdate, name, sex), clinical details (diagnosis date, weight at implantation), and procedural specifics (date of implantation, material composition). Additionally, prophylactic measures, complications (type, date), removal details (date, reason), and prior CVAD history were meticulously documented. Previous CVADs were defined as any tunneled CVAD implanted within the patient’s lifetime, with a recorded range of 1–5 prior placements.
Complications tracked encompassed bloodstream infections, site infections, dislodgements, occlusions, thromboses, arrhythmias, mechanical issues, and bleeding events.
Definition of complications
Complications were categorized as follows: catheter-related bloodstream infections (BSI), catheter dislodgement, occlusion, thrombosis, arrhythmia, insertion site infections, mechanical issues, and others. Immediate minor issues such as brief local bleeding at the implantation site that had no subsequent consequences in medical care were not considered.
Catheter-related BSI was diagnosed based on clinical signs of systemic infection and at least one positive blood culture obtained via the CVAD. Removal of the contaminated catheter depended on factors such as infection severity, pathogen type, and response to antibiotic treatment and was always discussed together with the primary team (e.g., the pediatric oncologists). Dislodgement referred to any shift in the catheter tip position away from the central part of the venous system, rendering it unusable as a CVAD. CVAD occlusion was identified by partial or complete blockage of the catheter lumen, requiring surgical intervention for resolution. Thrombosis involved the formation of a clot extending to the nearby vessel area, including potential pulmonary embolism. Mechanical complications encompassed any dysfunction of the CVAD and included rupture or other damages to the CVAD.
In cases where two complications occurred at the same time, one complication was defined as the main complication leading to the other one (mechanical complication leading to dislodgement and thrombosis, thrombosis leading to occlusion).
Statistics
Continuous variables were expressed as median or mean ± standard deviation and categorical variables as frequency (%). Cox proportional regression was used to investigate the relationship of complication rates and other parameters of interest. Patients who did not experience the outcome event were censored at the time of the last follow-up. We rigorously tested the assumptions of the Cox proportional hazards model, including checks for proportionality, to ensure the validity of our findings. Additionally, sensitivity analyses were conducted to assess the robustness of the results, particularly in subgroups with repeated CVAD placements. These measures strengthen the reliability of our conclusions despite the retrospective nature of the study. Hazard ratios were estimated with 95% CIs and a multivariable model was constructed. Results were considered statistically significant at p < 0.05. Data in this study was analyzed using IBM SPSS Statistics 29.0.02(20).
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University Hospital Essen (Approval number: 22–10,967-BO). The Ethics Committee emphasized that, due to the absence of consent, only retrospective data from existing medical records obtained through routine clinical care may be used for this research. In compliance with data protection regulations, personal data will be anonymized as soon as the research purpose allows.
Consent to participate
As this is a retrospective study, no informed consent was required.









留言 (0)