Study design and participants
We conducted a multicenter cohort study of children whose mothers were enrolled in the FEPED cohort. The FEPED cohort is an observational prospective cohort of 3129 French and Belgian women with a singleton pregnancy that was assembled between April 2012 and July 2014 and designed to study the association between vitamin D status during pregnancy and pre-eclampsia. Maternal plasma vitamin D concentrations during the T1 and T3, as well as in cord blood, were available for approximately 1400 women. The FEPED study design has been fully described previously [24,25,26].
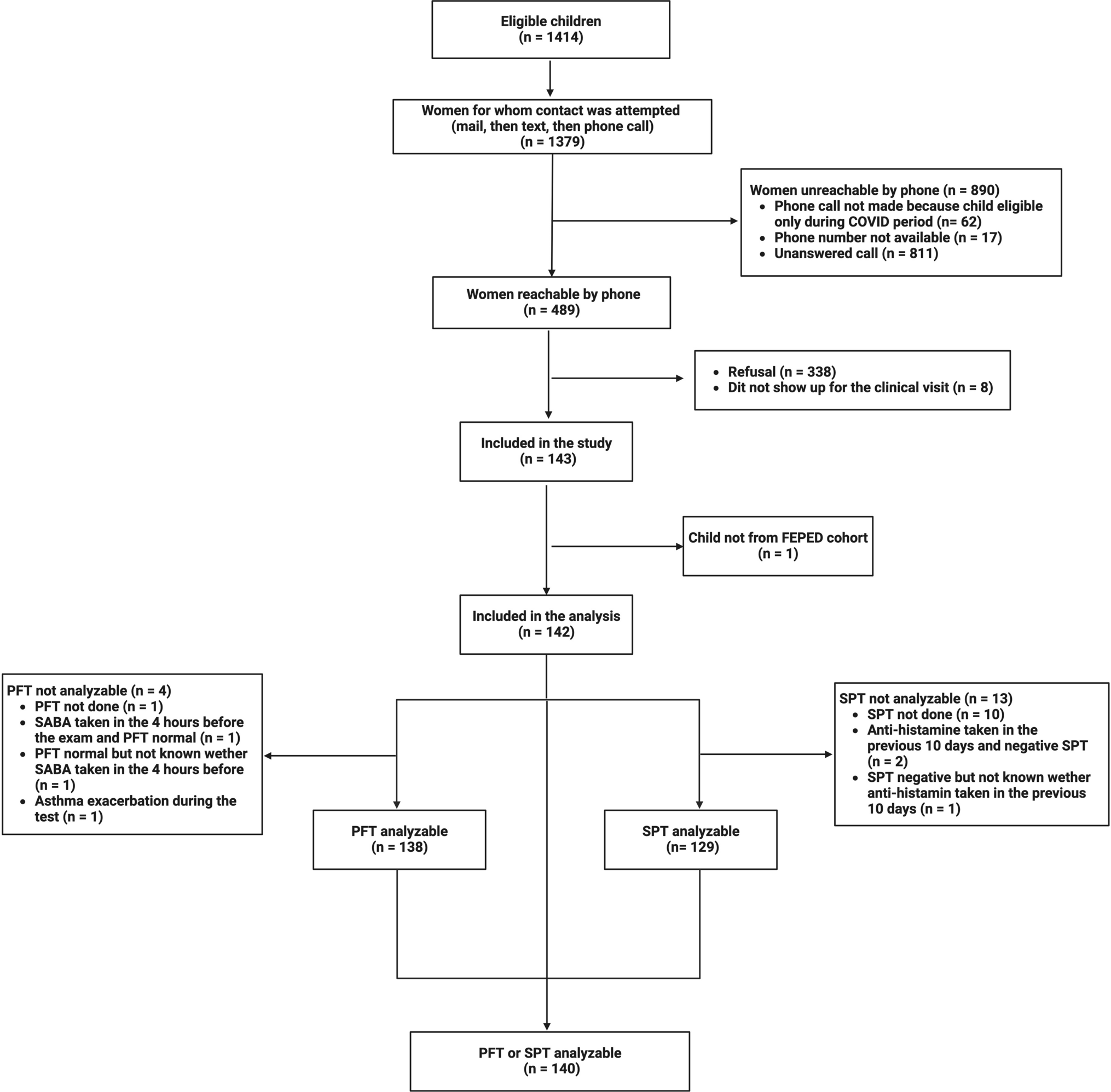
Children were enrolled between August 2018 and September 2021. Inclusion criteria were birth at term (≥ 37 weeks of post-menstrual age), availability of vitamin D plasma concentrations during T1 and T3 and in cord blood, and age of 5 to 6 years at the time of participation. The exclusion criterion was an underlying disease that prohibited the performance of lung function tests. The women included in FEPED whose children were eligible to participate in the RESPIFEPED study were contacted. If they agreed to their child’s participation, a visit was scheduled at the investigating center of their choice. Three centers participated in the study: Necker Enfants Malades Hospital, Robert Debré Hospital, and Armand Trousseau Hospital, all located in Paris, France.
Written and oral informed consent was obtained from at least one parent at enrolment. This study was approved by the Comité de Protection des Personnes CPP Ile de France VI on (CPP/32–17), registered with the ClinicalTrials.gov identifier NCT03229317, and conducted in accordance with the Declaration of Helsinki.
Clinical data collection
Clinical data were obtained by interviewing the parents during the visit and the child’s physical examination. The following data were collected concerning the child: vitamin D supplementation since birth, the occurrence of one or more episodes of bronchiolitis and the age at the first episode, preschool asthma diagnosis defined by at least three wheezing episodes before 36 months of age, asthma at the age of 5 to 6 years (school-age asthma) using the international ISAAC questionnaire [27], history of anti-asthmatic and antihistamine treatment since birth, presence of allergic rhinitis or atopic dermatitis symptoms using the international ISAAC questionnaire [27], intrauterine and postnatal tobacco exposure, weight, height, and child’s skin color (Fitzpatrick classification) [28].
Skin prick test
Seven standard solutions (cat, dog, Alternaria alternata, birch, orchard-grass, Dermatophagoides pteronyssinus, Dermatophagoides farinae), one positive control (10 mg/ml histamine dihydrochloride), and one negative control (50% glycerol saline solution) were used for skin prick tests (SPT) as previously described [29]. No request was made to stop antihistamine treatment(s) before the test, but the results were considered uninterpretable if negative and an antihistamine had been taken within 10 days.
Pulmonary function test (PFT)
sReff was obtained using the same method for all participating centers with identical plethysmography cabins (MasterScope Body; Erich Jaeger, Würtzburg, Germany): three sets of 10 breaths at 30–45 breaths/min were examined and the results from the median breath from the median trial reported. Reference equations were those of Kirkby et al. [30]. We chose sReff as the primary endpoint for several reasons. First, plethysmographic-specific airway resistance (sRaw) is a measure suitable for most 5- to 6-year-olds [31,32,33,34], with reliable reference equations and a standardized method [30]. Second, it is an index of both airway caliber and alveolar growth, as it is equal to the airway resistance (Raw) multiplied by the functional residual capacity (FRC) [30, 35]. Third, it is an earlier measure of obstruction than the forced expiratory volume in 1 s (FEV1) [36]. Finally, sReff calculates specific Raw from multiple points throughout the breathing cycle and is, therefore, the recommended sRaw measurement in children [30].
Resistance was also measured during expiration using the interrupter technique (Rint). This method was chosen as a complement to increase the chance of having at least one resistance measurement per participant. Reference equations were those of Merkus et al. [37]. FRC was measured by the helium dilution method, and the reference equations were those of Zapletal et al. [38]. All results are expressed as a percentage (%) of their predicted value.
No request was made to stop asthma treatment(s) before the test, but results were considered uninterpretable if normal, and a short-acting beta agonist had been taken within 4 h.
Vitamin D measurement and status definition
Maternal plasma vitamin D concentration was measured during the T1 and T3 of pregnancy and that of the newborn in the cord blood at birth. Vitamin D concentrations refer to the measurement of total 25-hydroxyvitamin D (25(OH)D), which was obtained according to the FEPED protocol [26]. Vitamin D status was defined, according to the literature, as follows: < 20 ng/ml: deficient, ≥ 20 mg/ml: sufficient [39].
Statistical analysis
The required sample size to detect a difference in sReff of 10% (standard deviation = 20%) with 80% power and a two-sided 5% alpha risk was calculated to be 180 subjects. We estimated that 10% of the tests (SPT and PFT) might not be analyzable and aimed to include 200 children.
Baseline characteristics of included and eligible non-included children were compared using the chi-square test for categorical and Student’s t-test for continuous variables. Subjects were separated into two groups for analysis of the primary endpoint: those with a vitamin D concentration during T1 < 20 ng/ml (exposed) and those with a concentration ≥ 20 ng/ml (unexposed). Baseline characteristics of exposed and non-exposed children were compared using the chi-square test for categorical and the Wilcoxon rank-sum test for continuous variables. The primary endpoint (sReff) was compared between exposed and non-exposed subjects using Student’s t-test, as were the other respiratory functional parameters (FRC and Rint). The same analyses were conducted using maternal vitamin D concentration during T3 and in cord blood. Correlation between vitamin D plasma concentration at T1, T3, cord-blood and sReff, Rint, and FRC was assessed by the Spearman coefficient. Associations between potential confounders (intrauterine and postnatal tobacco exposure, bronchiolitis before 6 months of age, skin color) and lung function indices were assessed using Student’s or Welch’s t-tests. Associations between secondary endpoints (asthma before 36 months of age, asthma at age 5–6, occurrence of at least one episode of bronchiolitis, presence of allergic sensitization, skin color) and vitamin D concentration during T1 were assessed using the chi-square test. Quantitative variables are expressed as means (standard deviations) or medians [ranges] and qualitative variables as n (%). All statistical analyses were performed using R statistical software 4.0.3 (http://cran.rproject.org).









留言 (0)