
記住我
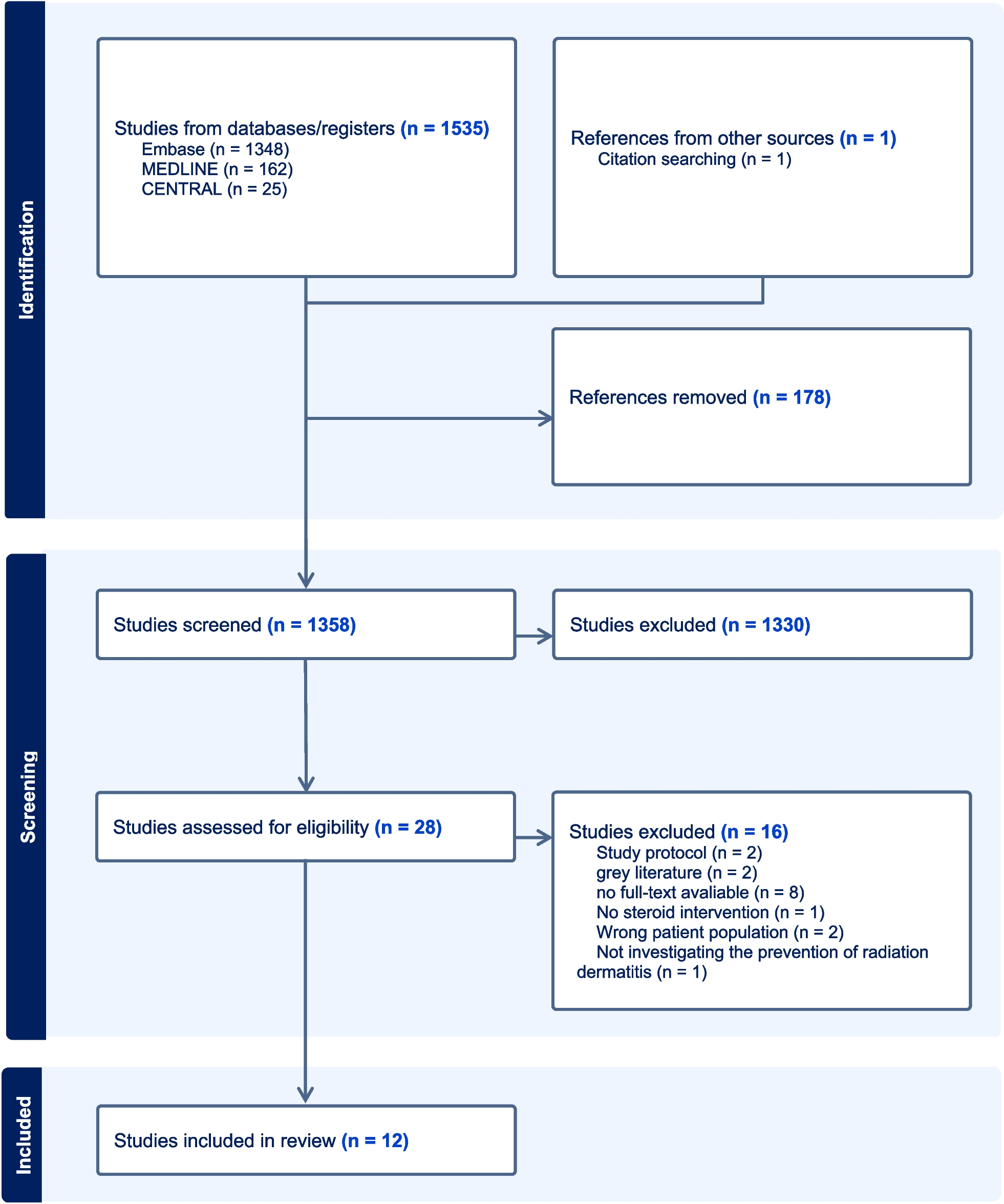

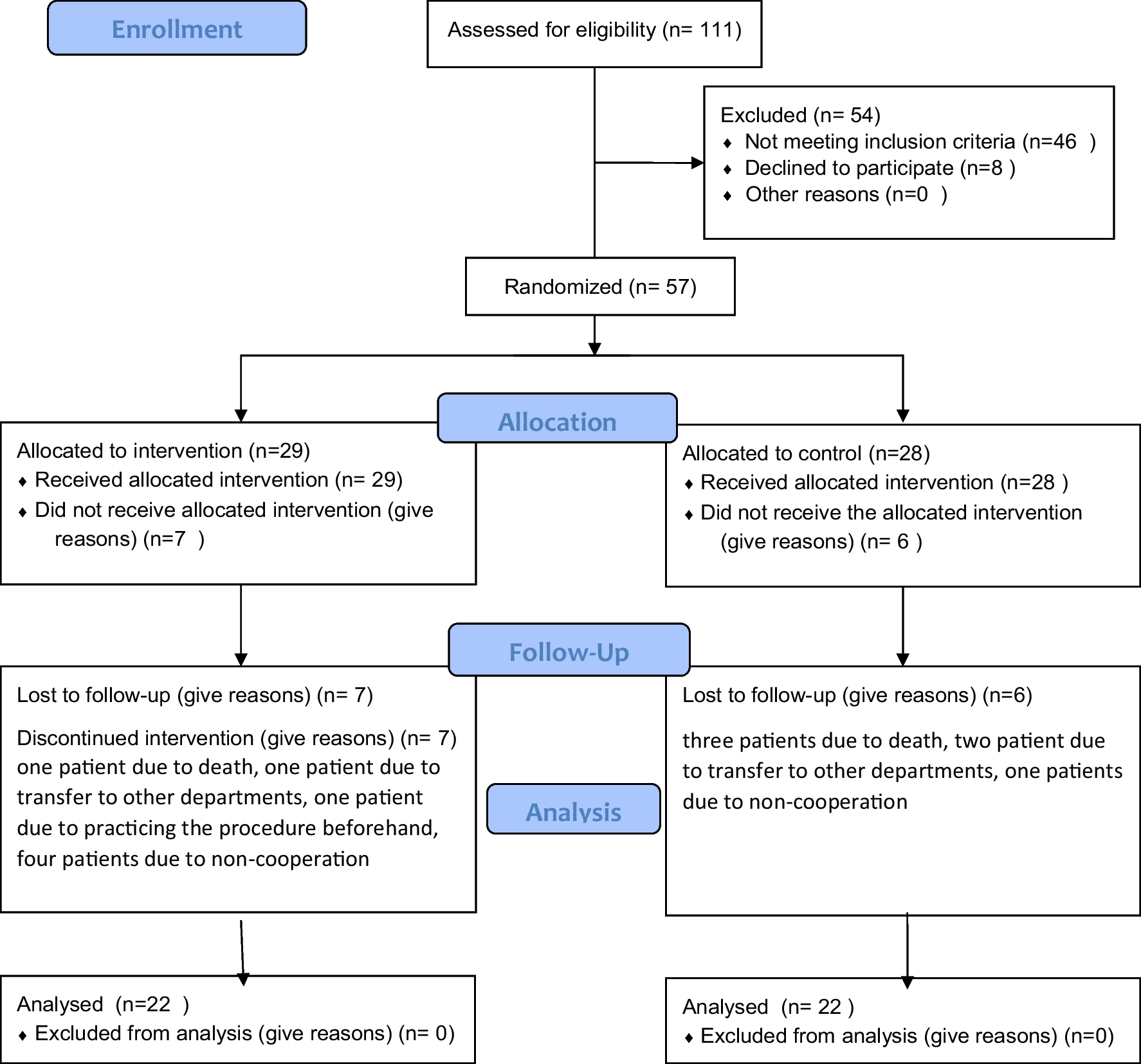
Semi-structured interviews were conducted with 28 patients, 10 family members and 18 healthcare professionals (see Fig. 2). Table 2 provides an overview of participant characteristics. Patients were recruited through Liverpool University Hospitals NHS Foundation Trust (LUHFT) and had a wide range of demographic and clinical characteristics. The majority of patients were living in the North West of England (26, 93%) with deprivation deciles ranging from one (most deprived) to 10 (least deprived). Six family members (60%) were recruited through LUHFT and four (40%) were recruited through snowball sampling. The majority of family members were living in the North West of England (9, 90%), with deprivation deciles ranging from one to 10. Fifteen professionals (83%) were recruited through online advertisements, and three (17%) were recruited through snowball sampling. All professionals were practising in the North West of England and worked across a variety of healthcare settings. Interviews ranged between 16 and 110 minutes.
Fig. 2
Recruitment flow diagram (N = 56)
Table 2 Participant characteristics (N = 56)GSE and IPAQ-SF dataPatients self-reported a range of GSE scores, which ranged between 22 and 40 (median = 32, Interquartile range (IQR) = 9). Twelve patients (43%) self-reported moderate levels of PA (Category two, IPAQ-SF); nine patients (32%) self-reported high levels of PA (Category three, IPAQ-SF) and seven patients (25%) self-reported low levels of PA (Category one, IPAQ-SF). The majority of patients (22, 79%) met the CMOs’ PA guidelines for adults or for older adults, relating to the amount of aerobic PA conducted per week.
The majority of healthcare professionals (11, 61%) self-reported high levels of PA (Category three, IPAQ-SF), five professionals (28%) self-reported moderate levels of PA (Category two, IPAQ-SF), and one professional (6%) self-reported low levels of PA (Category one, IPAQ-SF). All professionals who reported IPAQ-SF data (17, 94%), met the CMOs’ PA guidelines for adults, relating to the amount of aerobic PA conducted per week.
Patient self-reported GSE data alongside self-reported IPAQ-SF data for both patients and healthcare professionals are presented in Table 3.
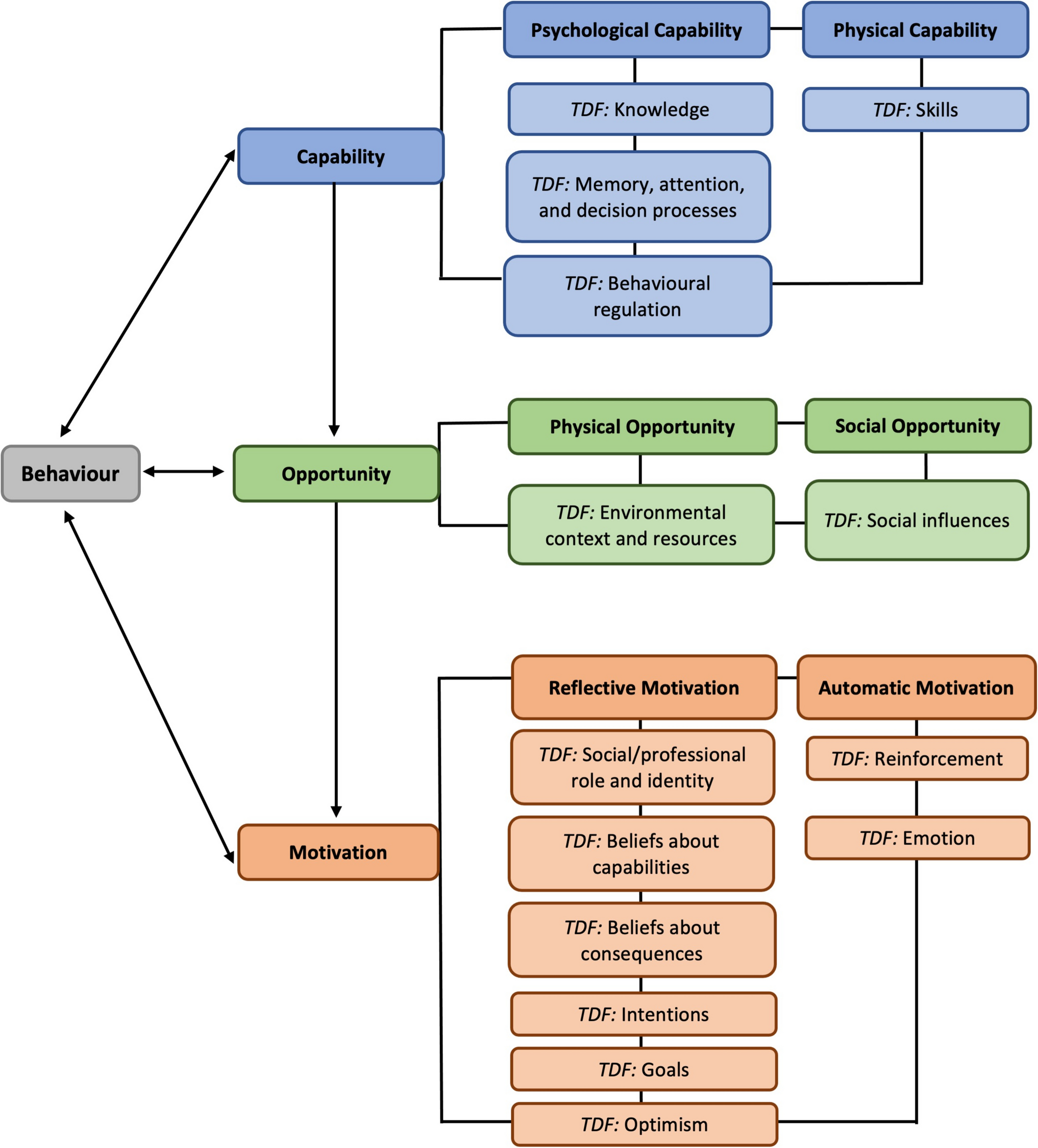
Table 3 Patients’ General Self-Efficacy (GSE) and International PA Questionnaire – Short Form (IPAQ-SF) Data (N = 28) and Professionals’ IPAQ-SF Data (N = 18)ThemesReflexive thematic analysis led to the identification of six themes. Capability-related themes included ‘lack of physical capability due to treatment-related side effects’ and ‘lack of knowledge about the benefits and importance of PA’. An opportunity-related theme was related to ‘HaNC as a disadvantaged patient cohort’ and motivation-related themes included ‘fear of causing harm by being physically active’ and ‘perceptions of who is responsible for PA promotion’. An additional theme related to the implications of the COVID-19 pandemic.
Lack of physical capability due to treatment-related side effects (COM-B: physical capability; TDF: skills)Many participants described how treatment-related side effects can create a barrier to daily functioning and PA. Professionals discussed that HaNC patients can experience treatment-related side effects that are more challenging, compared with other cancer types.
“… If you look at the treatment effects globally on a patient between head and neck radiotherapy, pelvic radiotherapy for maybe prostate or cervical cancer, and maybe breast radiotherapy… head and neck is- I think it is an accepted fact, it is way harder to get through.” (HCP4; Surgery).
The most common treatment-related side effects included fatigue and difficulties in eating and drinking.
“Just tiredness… he’d only have to sit on the bed for five minutes and he’d fall asleep.” (F3).
“I was out of action for a couple of weeks. When I say action, I mean, I could not eat, I could not swallow...” (P2).
Lack of knowledge about the benefits and importance of PA (COM-B: psychological capability; TDF: knowledge)Some patients described not understating how being physically active could help them prepare for treatment, help them day-to-day or to manage treatment-related side effects.
“If somebody said to me, “Go and walk for two miles a day” I would say, “Why? It is my neck that is bad. Walking is not going to affect my neck…” (P2).
Patients and family members described how receiving advice from healthcare professionals on the benefits and importance of PA would have been useful.
“I think just giving them a bit of advice to, it sounds a bit corny, getting a bit more active. It’s only going to benefit you later on...” (P18).
Notably, a patient described thinking their healthcare professionals did not perceive they would benefit from being physically active.
“I think maybe they perhaps don't simply register the fact that people would benefit from trying to be active.” (P17).
Professionals’ own perceptions and interest in PA influenced their discussions with patients. Those who were physically active discussed being unable to “leave that at the door when I go into my clinic” (HCP4; Surgery). While another described that if professionals are not physically active or interested in PA themselves, it is “very hard for them to encourage others to do it when it’s not what they actually do themselves…” (HCP12; Physiotherapy).
Professionals described that receiving training on the benefits of PA for HaNC would be useful. This training could include a “small module on mandatory training” (HCP17; Radiotherapy), and “more education around where to signpost” (HCP13; Nursing).
HaNC as a disadvantaged patient cohort (COM-B: physical and social opportunity; TDF: environmental context and resources and social influences)One patient described how she had been diagnosed with breast cancer and was offered a Macmillan-led PA class for people with breast cancer, which was “one of the best things” she had done as it helped her “physically and mentally”. She described how she did not understand “why they can't do that sort of thing for HaNC” (P25).
Professionals discussed that PA promotion needed to be prioritised across health services and recognised as a core factor in the treatment and recovery for HaNC.
“For me, it’s absolutely out there, exercise is medicine. It’s just not seen like that at all. But it sits in that same category. It’s all treatment on the same scale.” (HCP12; Physiotherapy)
However, a challenge to PA promotion was to “look at what are you prioritising it over” (HCP5; Speech and Language Therapy).
Fear of causing harm by being physically active (COM-B: automatic motivation and reflective motivation; TDF: emotion and beliefs about consequences)Many participants expressed fear of overexertion, and lacked confidence in what they were able to do and were fearful of weight loss. One family member described that she thought if her father lost weight, it meant he was at risk of having a recurrence.
“He had had an appointment and (a doctor) had said that he had never had a patient where they had gained weight and they had a recurrence. So, it is sort of like…in my head, I just thought, “Well, if he loses weight, what does that mean?” … he is more at risk of having a recurrence.” (F4).
One patient described being advised to do less PA by their healthcare professional and feeling worse as a result.
“When I found out what it was, she was wanting me to do compared to what I had been doing, I thought “Oh God, I’m going to rot in my chair.”… I gave it a go anyway and I must admit I didn’t feel as good as what I had done.” (P26)
Several professionals discussed that if patients burnt too many calories and lost weight, this could have had a detrimental impact on their treatment.
“… We don’t want them to lose weight, and then we explain the reason, because we don’t want the mask to be gappy. So, the consequence if the immobilisation doesn’t fit to the patient, is that they have to go through the re-scan and re-plan stage, which makes their treatment longer.” (HCP7; Radiotherapy)
Perceptions of who is responsible for PA promotion (COM-B: reflective motivation and physical opportunity; TDF: social/professional role and identity and environmental context and resources)Many professionals described they did not see it as part of their role to discuss PA with their patients.
“I have not had a great deal of discussions about PA with patients, because I do not have to.” (HCP6; Nursing)
The majority of professionals discussed how PA promotion needed to be a multidisciplinary approach to ensure that a consistent message was being conveyed to patients. However, one professional identified that a consultant’s input was imperative when encouraging and facilitating behaviour change.
“There’s so much anecdotal evidence out there that the patients do everything that their consultant says, so if it’s coming from them, it’s more embedded...” (HCP1; Physiotherapy)
One professional described how other health promoting behaviours were discussed in consultations, as these factors are involved in the “aetiology of the disease and the response to treatment” (HCP4; Surgery).
“We have got as far as smoking, alcohol, generally a healthier lifestyle, diet [advice]… and there are a couple of good reasons for that… It’s more medicalised anyway, it’s part of your medical history, more typically… and it can be just a straight limitation about how you manage the patients pre-operatively.” (HCP4; Surgery)
Implications of the COVID-19 pandemic (COM-B: physical capability and physical opportunity; TDF: skills and environmental context and resources)Some patients discussed being less physically active during the pandemic and some professionals discussed that as a result of lower PA levels, patients presented with reduced physical capability prior to treatment.
“After COVID and everything, that has just thrown everything out the window because we've stopped for a year and a half…” (P4)
“A lot of people now, not so much at the start of the pandemic but now, are saying, “I’ve not done anything for the past 18 months because of COVID…” So, a lot of patients are coming through to have their surgery saying, “I’m deconditioned anyway.” (HCP1; Physiotherapy)
One professional discussed that as patients with cancer were advised to self-isolate during the COVID-19 pandemic, when this advice was lifted, they forgot to promote PA again with their patients.
“I wasn’t really discussing it with patients so much… when patients could actually start going out and things again, I had forgotten to mention it…” (HCP11; Radiotherapy)
Notably, one professional discussed the results of a surgical research trial conducted during the COVID-19 pandemic, which found that self-isolation was detrimental to patients.
“It said, ‘isolation before elective surgery might be associated with a small but clinically important increased risk of post-operative pulmonary complications.’… It just suggested that we might be doing a harmful thing for our patients by telling them to go and hide away in the cupboard because COVID is out there.” (HCP2; Surgery)
留言 (0)