
記住我
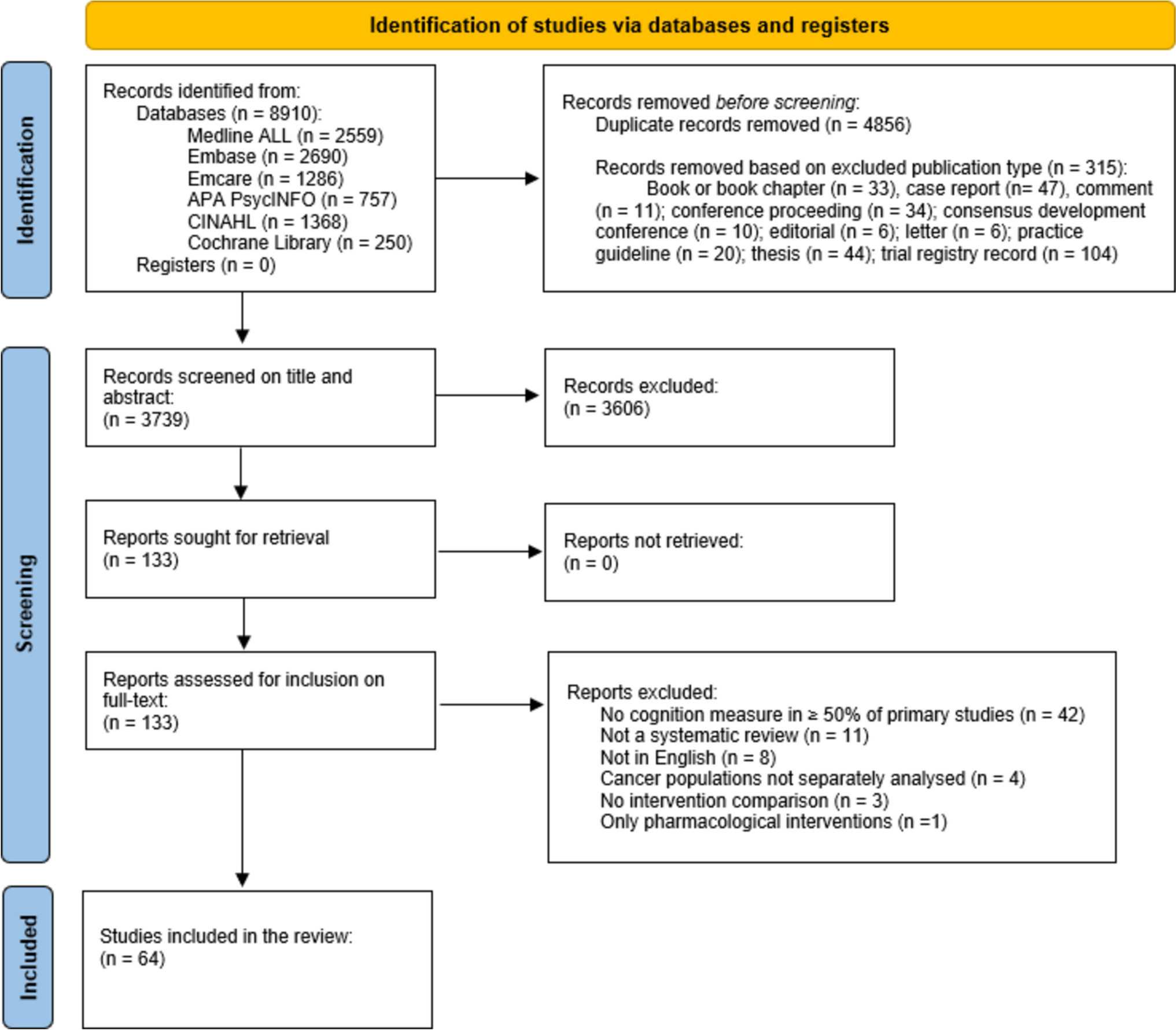

Overall, 8910 records were identified through database searches and 5171 records excluded before screening. After screening, 64 SRs were included in the narrative synthesis (see Fig. 1). The primary reasons for exclusion of full-texts were no cognition measure in ≥ 50% of primary studies (61%), not a SR (16%), and not in English (12%). The 64 SRs captured 318 individual primary studies relevant to our objective, totalling 30,847 participants (see Supplementary Material, Part 2 for primary studies). The number of relevant primary studies in the SRs ranged from 2 to 75. A total of 146 relevant primary studies were included in at least two of the SRs. The CCA determined an overall of 3% of the relevant primary studies, indicating a ‘slight overlap’ [39].
Fig. 1
The characteristics and quality assessment of the 64 included SRs are summarised in Table 2.
Table 2 Characteristics of included SRsIn total, 44% of SRs included only randomised control trials (RCTs; n = 28), with two of the 64 reviews (3.3%) not including RCTs, resulting in relevant RCTs being included in 97% of SRs (n = 62). Most SRs included multiple cancer types (n = 36; 56%), with the most common cancers being breast (n = 39 reviews; 61%), followed by brain (n = 21; 33%), prostate (n = 10; 16%), colorectal (n = 6; 9%), and lung (n = 5; 8%). Haematological cancers were included in 10 of the 64 reviews (16%). Fourteen SRs reported the inclusion of studies whereby participants had pre-intervention cognitive impairment (22%), with 9 only including primary studies that had participants who showed pre-intervention cognitive impairment (14.06%).
The number of participants included within each SR ranged from 41 to 7895. Of the SRs that reported mean participant age ranges across their primary studies (n = 22; 34.4%), mean ages ranged from 5 to 75 years. Of the reviews that reported sex or gender (n = 29; 45.3%), most included multiple sexes or genders (n = 21; 32.8%) with only females being included in 11 of the 64 reviews (17.3%). Most reviews included both subjective and objective cognitive assessments (n = 48; 75%), with 9 of 64 reviews only including objective cognitive assessments (14.1%), and seven only including subjective cognitive assessments (11%). The specific cognitive measures included within each review can be found in the Supplementary Materials, Part 3.
Quality appraisal of systematic reviewsThe AMSTART quality ratings found the majority of reviews were of ‘low quality’ (n = 39; 60.94%), followed by ‘moderate quality’ (n = 15; 23.4%), ‘critically low quality’ (n = 8; 12.5%), and ‘high quality’ (n = 2; 3.1%). The mean AMSTAR quality rating across all reviews was 1.17 (SD = 0.68) reflecting an overall ‘low-to-moderate’ quality. A variety of quality appraisal tools were used in the included reviews, most commonly the AMSTAR and the Risk of Bias in Systematic Reviews (ROBIS) tool.
Intervention characteristics and effectivenessThe characteristics of interventions and outcomes from the SRs are summarised in Table 3 across intervention domains. Most SRs included mixed intervention types (n = 24; 37.5%), followed by Physical activity/exercise (n = 15; 23.4%), cognitive training/rehabilitation (n = 15; 23.4%), mind–body and psychological/behavioural interventions (n = 5; 7.8%), and multi-modal/complex interventions (n = 4; 64.5%). See Supplementary Material Part 3 for additional details of the included reviews (i.e. countries, intervention descriptions, cognitive measures.
Table 3 SRs characteristics of interventions and outcomesCognitive training/rehabilitationIn total, 15 (23%) SRs primarily assessed cognitive training/rehabilitation interventions, with a further 21 (33%) including some cognitive training/rehabilitation interventions. All SRs primarily assessing cognitive training/rehabilitation included RCTs (n = 15) with 27% of these only including RCTs. Interventions reported included computerised cognitive training (13%), multi-component cognitive rehabilitation (13%), strategy training (7%), and a combination of these interventions subjective measures, such as the Functional Assessment of Cognitive Therapy-Cognitive Function (FACT-COG) and the Patient Reported Outcomes Measurement Information System Cognitive Function (PROMIS-COG), and objective measures such as the Wisconsin Card Sorting Task, Trail Making Test, and the Auditory Verbal Learning Test (see Supplementary Materials, Part 3 for a full list of measures in each SR).
Interventions typically resulted in improvements in cognition in cancer survivors. Included meta-analyses primarily assessing cognitive training/rehabilitation found efficacy in improving subjective cognition (n = 2; SMD range = 0.30–0.52), and objective cognition (Memory (n = 3); SMD range = 0.18–0.42, median = 0.40. Attention (n = 2) SMD range = 0.09–0.81. Executive Functioning; SMD range = 0.15–0.81), with primarily medium effects. Overall, 87% of the SRs primarily assessing cognitive training/rehabilitation reported general efficacy (> 50% primary studies showing efficacy) in improving > 50% of measured domains of subjective and/or objective cognitive functioning. For example, Von Ah et al. [89] found cognitive training and rehabilitation resulted in pre- to post-intervention improvements in memory, self-reported cognitive functions, attention, verbal fluency, processing speed, letter fluency, cognitive flexibility, executive function, and global cognition for adult cancer survivors of various tumour types. Yan et al. [94] found cognitive training significantly improved processing speed, verbal memory, working memory, episodic memory, and overall subjective cognition in mid-to-older adults across various cancer types and stages. However, there was some variability in results with SRs finding some cognitive training/rehabilitation interventions to be ineffective in improving particular domains of cognition in cancer survivors. All (n = 34) SRs that assessed cognitive training/rehabilitation interventions found some interventions to be ineffective for one or more cognitive processes. For example, while Von Ah et al. [89] typically found improvements in cognition, other studies reported no improvements in memory, subjective cognitive function, executive function, processing speed, psychomotor speed, attention, verbal fluency, subjective cognitive function, cognitive flexibility, daily function, or global cognition. Similarly, Yan et al. [94], while finding general effectiveness in their meta-analysis, found no significant improvements from cognitive training on the domains of attention, short-term memory, or executive functioning.
While many of the reviews discussed or attempted to identify differentiating interventional, methodological, or participant characteristics explaining the variability in effectiveness observed, no clear and consistent components, factors, or characteristics could explain intervention effectiveness variation across the SRs. Overall, cognitive training/rehabilitation interventions were found to be effective for improving cognition in cancer survivors across various tumour types, stages, and participant ages, however, there was variability in effectiveness across a range of cognitive processes with no clear differentiating components, factors, or characteristics.
Physical activity/exerciseOverall, 15 (23%) SRs primarily assessed physical activity/exercise interventions, with a further 20 (31.3%) including physical activity/exercise interventions. Fifteen SRs included some RCTs on physical activity/exercise, and ten focused exclusively on RCTs. The majority of SRs (n = 12; 80%) included a mix of aerobic, resistance, and combined aerobic/resistance interventions. A further three SRs (20%) included only aerobic interventions (e.g. walking, cycling, jogging). Resistance training included weighted exercise programs (see Supplementary Materials, Part 3 for additional details of interventions). Cognitive measures included both subjective measures, such as the European Organisation for Research and Treatment of Cancer-Cognitive Functioning Scale (EORTC-CFS), PROMIS-COG, and the Cognitive Failures Questionnaire, and objective measures such as CogState, Montreal Cognitive Assessment (MOCA), and Trail Making Test (see Supplementary Materials, Part 3 for a full list of measures in each SR).
The interventions typically resulted in improvements in cognition in cancer survivors, although mixed results were common. Included meta-analyses primarily assessing physical activity/exercise interventions found slight efficacy in improving subjective cognition (n = 7, SMD range = 0.01–0.51, median = 0.18); objective cognition (memory (n = 1, SMD = 0.03); executive functioning (n = 1, SMD = 0.19); processing speed (n = 1, SMD = 0.08 and overall (N = 1; paediatric/adolescence, SMD = 0.40) with primarily small to medium effects. Overall, 60% of the SRs primarily assessing physical activity/exercise interventions found general efficacy (> 50% primary studies showing efficacy) in improving > 50% of measured domains of subjective and/or objective cognitive functioning. For example, Bernal et al. [44] found a small-to-medium effect of an exercise intervention on childhood cancer survivors (various types) in objective (5 RCTs) and subjective (13 RCTs) cognitive functioning. Furthermore, Hiensch et al. [62] found resistance, aerobic, and mixed exercise interventions to have a small statistically significant effect on self-reported cognitive functioning in mid-to-older adult survivors of various cancers. There was notable variability in results with some SRs finding some physical activity/exercise interventions to be ineffective in improving cognition in cancer survivors across general cognition or within specific cognitive domains. For example, Brunet et al. [46] found that, across a wide range of physical activity and exercise interventions, the effects were inconclusive in 71% (n = 50) of the included primary studies, and null effects were reported for subjective cognition.
Across the SRs, there was no clear pattern between physical activity and exercise intervention types and dose, participant characteristics, and efficacy of the interventions on particular or general subjective or objective cognitive performance. However, Bernal et al. [44] found studies that involved participants with a longer time since cancer diagnosis, or end of cancer treatment, more female participants, and lower levels of supervision were significantly associated with smaller improvements in cognitive function. Additionally, primary study quality may be related to efficacy. For example, Baydoun et al.’s [42] SR on the effects of yoga on cognition, found studies rated as ‘high quality’ reported positive effects while those rated as lower quality found null effects.
Overall, the slight majority of physical activity/exercise interventions were found to be effective in improving cognition in cancer survivors across cancer types and stages, and across physical activity/exercise types. However, there was a significant variability in the findings and the majority of positive effects were small to medium.
Mind–body and psychological/behaviouralFour (6%) SRs primarily assessed mind–body and psychological/behavioural therapy interventions, with a further 18 (28%) including some mind–body and psychological/behavioural therapy interventions. Four SRs primarily assessing mind–body and psychological/behavioural therapy interventions included non-RCTs and 25% (n = 1) included exclusively RCTs. These SRs included the interventions of mindfulness/stress reduction-based interventions (n = 2; 50%), and cognitive behavioural therapy (n = 1; 25%) (see Supplementary Materials, Part 3 for additional detail of interventions). Cognitive measures included both subjective measures, such as the Multiple Ability Self-Report Questionnaire, and the EORTC-CFS, and objective measures such as the California Learning Verbal Learning Test, and Stroop Task (see Supplementary Materials, Part 3 for a full list of measures).
The interventions typically resulted in improvements in cognition in cancer survivors. The included meta-analysis primarily mind–body and psychological/behavioural therapy found efficacy in improving subjective cognition (n = 1; SMD = 0.26), and objective cognition (Overall (n = 1); SMD = 0.11) with a small to medium effect. Overall, 80% of the SRs specifically assessing mind–body and psychological/behavioural therapy found general efficacy (> 50% primary studies showing efficacy) in improving > 50% of measured domains of subjective and/or objective cognitive functioning in cancer survivors. For example, Cifu et al. [53] found mindfulness-based interventions were typically effective at improving objectively and subjectively measured cognition in mid-to-older age adults with breast cancer from pre-intervention to the final 6-month follow-up measures. Furthermore, Hines et al. [63] in their SR on the effectiveness of CBT in improving cognition in cancer, found CBT to be typically effective for improving objective and subjectively measured cognition in cancer survivors who have had chemotherapy in the short-term post-intervention assessments. However, there was some variability in results, with all these SRs reporting some null findings. For example, while Hines et al. [63] found general efficacy of CBT intervention for improving short-term objective and subjective cognition, the majority of included primary studies did not demonstrate longer-lasting effects, finding no significant positive impacts of the interventions from 6 to 32 weeks. Furthermore, Zhang et al. [98] in their SR assessing mindfulness/relaxation-based interventions in adult cancer survivors found significant effects on subjective, but not objective measures of cognition.
Overall, mind–body and psychological/behavioural therapy interventions were found to be largely effective in improving cognition in cancer survivors. However, there was significant variability in the improvement of subjective or objective cognition across the SRs with no clear methodological or participant characteristics to explain this variability. Furthermore, the efficacy of mind–body and psychological/behavioural therapy interventions in improving cognition is primarily in the short-to-midterm (i.e. up to 6 months), with questionable efficacy longer-term.
Multi-modal/complex interventionsFour (6.3%) SRs assessed multi-modal/complex interventions. Two SRs only included RCTs (n = 2; 50%). Multi-modal/complex interventions included model of care approaches (n = 3; 75%), and health education (n = 1; 25%) (see Supplementary Materials, Part 3 for additional detail of interventions). Cognitive measures included both subjective measures, such as EORTC-CFS, and objective measures such as the Cognitive Functional Independence Measure) (see Supplementary Materials, Part 3 for a full list of measures in each SR).
Overall, the interventions typically resulted in improvements in cognition in cancer survivors. Most (75%) of the SRs assessing multi-modal/complex interventions found general efficacy (> 50% primary studies showing efficacy) in improving > 50% of measured domains of subjective and/or objective cognitive functioning in cancer survivors. For example, Zhao et al. [99] in their SR of health education RCTs in gastrointestinal cancer survivors found health interventions were effective in improving subjective cognition (no objective assessments were included) with a modest effect. Similarly, Wang et al. [92] in their SR of comprehensive nursing care interventions for lung cancer survivors found the interventions improved self-reported cognition with a medium effect. However, given the broad inclusion criteria of these multi-modal/complex intervention SRs, the specific efficacious mechanisms of effect are unknown. This also leads to challenges in understanding the factors that may result in an efficacious model of care intervention versus an intervention with null effects. For example, Cheng et al. [51] in their SR assessing multiple types of nurse-led interventions across cancer types found no effect of nurse-led interventions on subjective cognition. However, the characteristics of the interventions which may have led to a null effect are unclear.
Most (75%) multi-modal/complex interventions were found to be effective in improving cognition in cancer survivors. However, given the broad inclusion criteria of these SRs, it is challenging to understand the mechanisms of effect.
留言 (0)