
記住我
Executive functions are goal-oriented, complex task-solving cognitive processes (Friedman and Robbins, 2022; Funahashi, 2001), and are a multidimensional cognitive structure composed of inhibitory control, working memory, and cognitive flexibility (Baddeley, 1996; Pennington and Ozonoff, 1996). Executive functions play an important role in academic performance and innovative thinking (Guo et al., 2019; Zhang, 2021), the development and maintenance of healthy behaviors (Allan et al., 2016; Yang et al., 2020), as well as mental health and social adaptation (Liu et al., 2021; Xie et al., 2020). The childhood and adolescence period is the golden age for the development of executive functions. Research on strategies to promote executive functions during this stage is of great importance for future real-life decision-making, everyday reasoning, and the establishment of good interpersonal relationships (Shi et al., 2023c).
Physical exercise is a natural means of promoting the development of executive functions in children and adolescents (Verburgh et al., 2014; Xue et al., 2019). Currently, research on the relationship between physical exercise and executive functions mainly focuses on the exploration of dose-effect relationships. A series of studies (De Greeff et al., 2018; Rathore and Lom, 2017; Song et al., 2022; Xie, 2020) have found that long-term regular, moderate frequency and duration, and moderate-intensity exercise have the best intervention effects on the executive functions of children and adolescents. In addition, the type of exercise is an important qualitative element of exercise intervention and is also an important element that researchers (Diamond and Ling, 2016; Tomporowski et al., 2015) call for further exploration in studies. Researchers have conducted meta-analyses on the effects of aerobic (Song et al., 2022) and high-intensity interval training (Hu et al., 2021) interventions on the executive functions of children and adolescents, and both have found positive intervention effects. Furthermore, current meta-analyses on resistance training interventions for executive functions are mostly derived from the middle-aged and elderly population (Coelho-Junior et al., 2022; Landrigan et al., 2020), possibly due to misconceptions about the safety of resistance training for children and adolescents and its adverse effects on bone development.
Motor skills are the carriers of physical exercise, representing the combination of psychological processes and skill operation processes, and there is a shared brain mechanism for skill learning and cognitive tasks (Meijer et al., 2022; Ji et al., 2010). As research progresses, scholars (Gu et al., 2019; Shi and Feng, 2022; Shi et al., 2022) have gradually focused on the relationship between types of motor skills and the executive functions of children and adolescents. Based on the unpredictability of the environmental context, motor skills can be divided into open and closed skills. The former refers to the skills of performing movement tasks in an unpredictable environment, requiring individuals to respond and adjust their movements according to changes in the environment; the latter refers to the skills of performing movement tasks in a stable, predictable environment, where individuals can pre-plan their movement procedures (Zhang, 2012).
The aforementioned studies (Gu et al., 2019; Shi and Feng, 2022; Shi et al., 2022) all found that the effect of open-skill exercise intervention on the executive functions of children and adolescents is better than that of closed skills, mainly due to the rich environmental stimuli of open skills, which can generate more cognitive load on the brain (Shi et al., 2023c). In addition, there is a certain degree of similarity in cognitive demands between open-skill exercise and exercise that involves motor and cognitive dual tasks. The former requires participants to adapt to a constantly changing environment, necessitating greater cognitive load and promoting targeted practice of certain cognitive functions; the latter requires participants to perform cognitive tasks while engaging in physical activities. Both can enhance neuroplasticity, stimulate the formation of new neural connections, improve the integration of sensory and motor processes, and promote cognitive development (Deodato et al., 2024; Shi and Feng, 2022; Wollesen et al., 2022). This provides further evidence to support the positive benefits of open-skill exercise. However, some studies (Becker et al., 2018; Chueh et al., 2017) have reported that there is no difference in the effects of open and closed-skill exercise interventions.
The aforementioned controversy may be due to the differences in various types of open-skill exercises. According to Voss et al. (2010), open skills are further divided into strategic skills and interceptive skills. Strategic skills require individuals to process a large amount of information from the identities, positions, speeds, and trajectories of offensive and defensive players simultaneously, such as in soccer, basketball, hockey, and ice hockey. Interceptive skills require participants to coordinate dynamically with objects in the environment using their body, body parts, or handheld equipment, such as in table tennis, tennis, fencing, and boxing. Krenn et al. (2018) compared the executive function performance of athletes with interceptive, strategic, and closed skills. The results showed that compared to athletes with closed skills, those with strategic skills exhibited unique cognitive advantages in all three sub-functions of inhibitory control, working memory, and cognitive flexibility. In contrast, athletes with interceptive skills only performed well in inhibitory control. However, Voss et al. (2010) showed that athletes with interceptive skills had better cognitive performance than those with strategic skills. Therefore, the relationship between strategic skills and interceptive skills and executive functions is still inconsistent. Research on strategic and interceptive skills is mainly focused on athlete populations, while research on children and adolescents is relatively scarce. Moreover, it is necessary to further explore which type of open-skill exercise intervention is more effective under the premise of maximizing intervention strategies, thus necessitating subsequent studies to further explore based on this classification system.
Based on this, this study systematically searches for literature related to the intervention of open-skill exercises on the executive functions of children and adolescents, and on this basis, uses the method of combining effect sizes to test the effectiveness of the intervention, as well as to further explore the differences in the intervention effects of strategic and interceptive-skill exercises. In addition, this study also further explores the moderating effects of quantitative intervention elements and demographic variables in the intervention. Through this study, it is hoped to provide evidence for open-skill exercise interventions to improve the executive functions of children and adolescents, filling the research gap in strategic and interceptive skill exercises among children and adolescents, and providing a basis for formulating subsequent exercise intervention strategies for the executive functions of children and adolescents.
2 Literature review and research hypotheses 2.1 Effects of open skill-exercise on the executive functions of children and adolescentsOpen-skill exercises contain a rich array of environmental stimuli and interpersonal interaction elements, as well as a variety of problem-solving target tasks, which present children and adolescents with more cognitive challenges and thus offer superior benefits for the promotion of executive functions (Shi et al., 2023c). Although some studies (Becker et al., 2018; Chueh et al., 2017; Jäger et al., 2015) have not highlighted the positive benefits of open-skill exercises in promoting the executive functions of children and adolescents, more studies results have confirmed the more active promoting benefits of open-skill exercises. A series of cross-sectional studies (De Waelle et al., 2021; Holfelder et al., 2020; Möhring et al., 2022) show that children and adolescents participating in open-skill exercises have more cognitive response advantages in executive function task performance, can more readily perceive the trend of cognitive conflicts, and consciously adjust cognitive control strategies to allocate more attentional resources to resolve conflicts (Larson et al., 2014). A series of experimental studies also found that open-skill exercises, which constitute cognitive challenges, have positive intervention effects on the attention inhibition (Gallotta et al., 2015), verbal working memory (O’Brien et al., 2021), spatial working memory (Ottoboni et al., 2021), and executive function (Bai et al., 2022; Crova et al., 2014) task performance of children and adolescents, and the benefits produced by open skills are superior to those of closed skills.
In addition, previous meta-analyses have also confirmed the promoting benefits of open-skill exercises on executive functions. For example, Shi et al. (2022, 2023d) showed that open skills significantly promote the executive functions of both typical and atypical children and adolescents. Zhang et al. (2022) used a web- based meta-analysis to assess the intervention effects of 11 types of motor skills on the working memory of school-age children, and overall presented a pattern of “open skills > closed skills.” Therefore, based on the above research findings, this study proposes Research hypothesis 1: open-skill exercises can significantly improve the executive function of children and adolescents.
2.2 Differences in intervention effects of strategic and interceptive-skill exercisesVoss et al. (2010) further categorized open skills into strategic and interceptive skills in their research on the cognitive advantages of elite athletes and found that athletes with interceptive skills had superior cognitive performance. However, more studies (Krenn et al., 2018; Yu et al., 2019) support that athletes with strategic skills have more active executive function task performance. For example, Yu et al. (2019) used near-infrared brain imaging technology to compare the behavioral and brain activation differences in the attentional executive control network functions of basketball (strategic skill), table tennis (interceptive skill), and track and field (closed skill) athletes. They found that basketball and table tennis athletes showed higher executive control advantages, accompanied by significant activation in the right prefrontal cortex and inferior frontal gyrus, but basketball athletes were accompanied by activation in more brain areas such as the frontal eye field.
In addition, the results of Voss et al. (2010) seem to be inconsistent with research on children and adolescents. Song et al. (2022) integrated randomized controlled trials of strategic game-dominated physical exercise on the executive functions of children aged 4 to 12 through meta-analysis and found that strategic game exercises have positive intervention effects on inhibitory control, working memory, and cognitive flexibility. However, some studies show that the sports environment of interceptive skills and strategic skills is different, and there are specific cognitive requirements, so there is a selective promotion effect on cognitive performance. For example, Wu et al. (2007) compared the intervention effects of football (strategic skill) and table tennis (interceptive skill) on the attention quality of primary school students and found that football exercise was better than table tennis in the intervention effects of attention maintenance and attention transfer; while table tennis exercise was better than football in the intervention effects of attention stability, attention breadth, and attention concentration. Ji (2014) compared the relationship between four types of open skills and the executive function task performance of primary school students and found that the basketball and table tennis groups performed best in the inhibitory control task, while the badminton and taekwondo groups performed best in the cognitive flexibility task.
In addition, Shi et al. (2022) found that the promotion effect of strategic skills on the executive functions of children and adolescents is better than that of interceptive skills. However, this study only compared the proportion of studies with promotional benefits in different types of skill exercises through frequency analysis, and it is not possible to determine the effect size of the intervention, which greatly reduces the accuracy of the research results. Based on previous research on children and adolescents, this study proposes Research hypothesis 2: There is a difference in the effects of strategic and interceptive skill exercises on the executive functions of children and adolescents, and the effect of strategic skill exercise intervention is better than that of interceptive skills.
2.3 Moderating role of quantitative elements in the effectiveness of open-skill exercise interventionsThe quantitative elements of exercise intervention are the focus of dose–response relationship studies and an important factor for researchers to consider when formulating optimal intervention plans. These primarily include the intensity, duration, frequency, and duration of each exercise session.
Intervention intensity refers to the degree of physiological stimulation of the body activity in the exercise plan, which is mainly graded based on maximum heart rate or subjective feeling, and is usually divided into low intensity (<55% HRmax), moderate intensity (55–75% HRmax), and high intensity (>75% HRmax). Dong (2018) and Xie (2020) compared the intervention effects of moderate and high-intensity exercise on the working memory of children and adolescents, and found that moderate-intensity exercise has a positive intervention effect on both children and adolescents, while the intervention effect of high-intensity exercise is not significant, which may be related to the excessive fatigue induced by high-intensity exercise (Zhang, 2008). Shi et al. (2022), based on real exercise situations, also presented similar results, showing that both acute and long-term interventions of moderate exercise help to improve the executive functions of children and adolescents. In addition, research on the executive functions of atypical children and adolescents also shows similar results. For example, Yang (2021) found in a meta-analysis of exercise interventions for children with attention deficit hyperactivity disorder that moderate-intensity exercise has a positive intervention effect on inhibitory control and cognitive flexibility tasks. However, a recent meta-analysis (Feng et al., 2023) showed that both moderate and high-intensity open-skill exercises have a positive promotional benefit for the executive functions of typical children. But there is relatively less literature on high-intensity exercise, and the accuracy of its results needs further verification. Based on this, this study proposes Research Hypothesis 3: Intervention intensity has a moderating effect on the intervention effect of open-skill exercise on the executive functions of children and adolescents, and the intervention effect of moderate intensity is the best.
The intervention period is the total time from the start to the end of the exercise plan, usually measured in weeks. The human body gradually forms a response pattern adapted to the stimulus, suitable for its own survival, after long-term exposure to a specific stimulus (Wang and Su, 2016). Therefore, most current studies on the promotion of executive functions by exercise intervention are conducted with long-term interventions. Li et al. (2020) and Song et al. (2022) compared the promoting effects of different exercise intervention periods on the executive functions of children aged 3–7 and 4–12, respectively. The former showed that interventions below and above 10 weeks are both beneficial to the development of executive functions; while the latter showed that overall, interventions above 10 weeks have a better promoting effect. Shi et al. (2022) compared the promoting effects of real environment exercises below 8 weeks, 9–16 weeks, and above 17 weeks on the executive functions of children and adolescents through systematic review and found that interventions above 17 weeks have a more obvious effect. However, the study has not yet conducted a higher level of evidence combined effect test, so its accuracy is insufficient. Based on this, this study proposes Research hypothesis 4: The intervention period has a moderating effect on the intervention effect of open-skill exercise on the executive functions of children and adolescents, and the effect of longer period exercise is better.
The intervention frequency is the number of times the exercise plan is accepted within a unit of time, usually referring to the number of times of exercise per week. Li et al. (2020) showed that exercises below 3 times/week and above 3 times/week both have a positive intervention effect on the executive function task performance of children. However, Song et al. (2023) showed in their research on children and adolescents with attention deficit hyperactivity disorder that there is a selective promoting effect of exercise frequency on each dimension of executive function, that is, exercise at 2 times/week has a large effect size on the intervention effect of inhibitory control; exercise above 3 times/week has a medium to high effect size on the intervention effect of working memory. In addition, more studies support that the effect of exercise above 3 times/week is more positive, for example, Shi et al. (2022) and Song et al. (2022) showed that exercise above 3 times/week has a more positive promoting effect on the executive functions of children and adolescents. Based on this, this study proposes Research hypothesis 5: The intervention frequency has a moderating effect on the intervention effect of open-skill exercise on the executive functions of children and adolescents, and exercise above 3 times/week has a more positive promoting effect.
There is no unified standard for the classification of each exercise time in related studies, so there is no specific evidence of exercise time. Chen et al. (2015) found that 30 min of moderate-intensity basketball exercise has a better intervention effect on the executive functions of primary school students than 8 min and 15 min. Li et al. (2022) found that 40 min of moderate-intensity “basketball + rope skipping” intervention has a better promoting effect on executive functions than 20 min. In addition, related systematic reviews also show inconsistent results. Li et al. (2020) showed that exercises above and below 35 min both have a positive intervention effect on the executive functions of preschool children; while Song et al. (2022) showed that exercises lasting above 35 min have a higher effect size. Chang et al. (2012) showed that exercises lasting above 20 min have a more positive promoting effect on the cognitive task performance of adolescents; Yang (2021) found in his research on children with attention deficit hyperactivity disorder that exercises lasting 40–60 min overall have a higher effect size. In addition, Shi et al. (2022) also found that there is an inverted U-shaped relationship between each exercise time and executive function task performance, that is, exercises between 30–50 min have a better intervention effect on the executive functions of children and adolescents than those below 30 min and above 50 min. Based on this, this study proposes Research hypothesis 6: Each exercise time has a moderating effect on the intervention effect of open-skill exercise on the executive functions of children and adolescents, and moderate exercise time has a more positive promoting effect.
2.4 Moderating role of demographic variables in the intervention effects of open-skill exercisesAge, gender, and ethnicity are important demographic factors that affect the executive functions of children and adolescents (Peng et al., 2023). Firstly, executive functions have been regulating human activities since infancy, and some researchers (Anderson et al., 2018) have found that the fastest development stages of human executive functions are between 0 to 2 years, 7 to 9 years, and 16 to 19 years. Zhao et al. (2015) have shown that younger children have a more significant advantage in cognitive improvements caused by exercise. In addition, a meta-analysis (Wang et al., 2019) further confirmed this result, indicating that exercise has a positive effect on children, adolescents, and the elderly, but the effect size in the child group is much higher than in other groups. Secondly, girls generally exhibit higher executive functions and usually take longer than boys (Zhao et al., 2015). Moreover, boys are more inclined to participate in open-skill exercises with intense physical confrontation and rapid transitions of offense and defense, which is more conducive to the development of their executive functions. However, this study has not yet found comparative studies on the effects of exercise intervention on the executive functions of different gender groups. Lastly, Rea-Sandin et al. (2021) shows that the absolute difference in executive functions between white people and ethnic minorities is much larger than the absolute differences between ethnic minorities and within ethnic minorities, suggesting that ethnicity is a factor affecting executive functions. But this study has also not yet found comparative studies on the effects of exercise intervention on the executive functions of different ethnic groups.
Based on the above, this study proposes Research hypothesis 7: Age has a moderating effect on the intervention effect of open-skill exercises on the executive functions of children and adolescents, and exercise has a higher promoting effect on younger children than on older children and adolescents; and Research hypothesis H8: Gender has a moderating effect on the intervention effect of open-skill exercises on the executive functions of children and adolescents, and exercise has a more positive promoting effect on boys. In addition, for research on ethnicity, this study only conducts exploratory research and does not propose a research hypothesis.
3 MethodsThis study was conducted in compliance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 and was registered at International Prospective Register of Systematic Reviews (PROSPERO), under number CRD42025636714.
3.1 Search strategiesA single researcher conducted a literature search using Chinese and English search terms. Search terms included: (1) motor skill, sports skill, sports items, exercise, physical activity, fitness, exercise; (2) executive function, working memory, inhibition control, cognitive flexibility, self-control, self-regulation; (3) children, child, adolescents, pupils, teenagers, young, students. Boolean logic operators AND were used to connect the three sets of search terms, and OR was used to connect similar search terms. Searches were conducted in the CNKI, Web of Science (WOS), PubMed, ScienceDirect, and SPORTDiscus databases, with the search period extending from the establishment of the database to December 2023.
3.2 Inclusion and exclusion criteriaInclusion and exclusion criteria were designed according to the PICOS principle (Costantino et al., 2015). Inclusion criteria: (1) Participants were typically developing child adolescents; (2) Intervention measures are long-term interventions based on open skills; (3) Control measures include traditional physical education courses, basic academic courses, free activities, etc.; (4) Outcome variables include inhibition control, working memory, cognitive flexibility; (5) Study design includes randomized controlled trials (RCTs) and quasi-experimental designs (QEDs). Exclusion criteria: (1) Atypically developing children and adolescents with cognitive or intellectual disabilities, physical disabilities, etc.; (2) Unreported or uncertain types of motor skills; (3) Combination of open and closed skill interventions; (4) Screen-based motion games, such as Xbox, Kinect, and Nintendo, etc.; (5) Combined interventions of sports activities and cognitive therapy; (6) Cross-sectional, case–control, historical data, and other descriptive studies; (7) Reviews, abstracts, letters, comments, etc.; (8) Literature that cannot obtain original data (means and standard deviations); (9) Repeated publications for the same research subjects, only higher-quality literature is included. Two researchers independently conducted literature screening, and two other researchers conducted a second assessment of the screened literature. If there is controversial literature, the group discusses and decides together.
3.3 Data codingThis study is coded according to the following four parts: (1) Basic information of the literature, including the author, publication date, and research design; (2) Characteristics of the participants, including sample size, age, female proportion, and race; (3) Intervention and control measures, including intervention measures (intervention carrier, intervention intensity, intervention period, intervention frequency, and duration per session) and control measures; (4) Outcome variables, including measurement tools and main findings. In addition, the study classifies the intervention carrier into strategic skills and interceptive skills based on the classification standards of open skills. Included studies use reaction time, accuracy, and scores as three types of evaluation indicators to reflect the performance of executive function tasks. The faster the reaction time, the higher the accuracy and score, the better the executive function is indicated to be. To ensure the consistency of the direction of the index evaluation, the accuracy and score are extracted and coded in the opposite direction according to the study by Feng et al. (2023). The effect size is coded as an independent sample, that is, one independent sample codes one effect size. If there are multiple independent samples, they are coded separately (Cao et al., 2022).
Subgroup analysis helps to further clarify the effects of open skill exercise interventions on children and adolescents. Coding of moderating variables: (1) Open skill types are divided into strategic and interceptive skills; (2) Intervention intensity is divided into low, medium, and high; (3) Intervention period is divided into 6–10 weeks and 16–36 weeks; (4) Intervention frequency is divided into 1–2 times/week and 3–5 times/week; (5) Intervention time is divided into 30 min/session, 30-60 min/session, and 75-120 min/session; (6) Age is divided into 5–9 years old and 10–16 years old; (7) Race is divided into Eastern (including China and South Korea) and Western (including Italy, the United States, Switzerland, and Spain). Two researchers independently extract literature data, and two other researchers conduct a second assessment of the extracted content. If there are controversial issues, the group discusses and decides together.
3.4 Quality assessmentThis study uses the bias risk assessment tool recommended by the Cochrane Collaboration Network (Cumpston et al., 2019) to assess the quality of RCTs. The tool assesses from six aspects: randomization methods, blinding, allocation concealment, completeness of outcome data, selective reporting of study results, and other biases. Additionally, the Methodological Index for Non-Randomized Studies (MINORS) scale (Slim et al., 2003) is used to assess the quality of QEDs. This tool includes 12 items, with 9 to 12 items used for additional criteria in evaluating studies with a control group, each item is worth 2 points, with a total score of 24 points. A score of 0 indicates not reported; 1 indicates reported but insufficient information; 2 indicates reported and provides adequate information. Two researchers independently make judgments based on the evaluation tools, and if there are serious disagreements on items, they will discuss with a third researcher.
3.5 Statistical analysisData processing and statistical analysis are conducted using Stata16.0. Firstly, a meta-analysis is used to explore the effects of open skill exercise interventions on the executive functions of children and adolescents. The meta-analysis uses the standardized mean difference (SMD) to represent the effect size and the 95% CI to represent the estimated interval of the overall parameters constructed by the sample statistics. The Q test and I2 statistic are used to test the heterogeneity between studies. If I2 < 50%, p > 0.1, it is considered that there is little heterogeneity between studies, and a fixed effect model is selected for analysis; if I2 ≥ 50%, p ≤ 0.1, it is considered that there is significant heterogeneity between studies, and a random effect model is selected for analysis (Sun and Shi, 2021). Secondly, subgroup analysis and meta-regression analysis are used to explore the moderating effects of exercise intervention elements and demographic variables. Finally, the Egger linear regression model is used for literature publication bias test, and the one-by-one exclusion method is used for literature sensitivity analysis. The heterogeneity test level is set to α = 0.1, and the other test levels are set to α = 0.05.
4 Results 4.1 Screening resultsThis study retrieved a total of 7,883 articles through the search. After deduplication using EndNote X9 software and excluding articles that were completely unrelated to the topic of this study (for example, those that did not include the search keywords in the title at all), 865 articles were obtained. In addition, based on the inclusion and exclusion criteria, several rounds of screening were conducted, and ultimately 16 articles were included. The search process is shown in Figure 1.
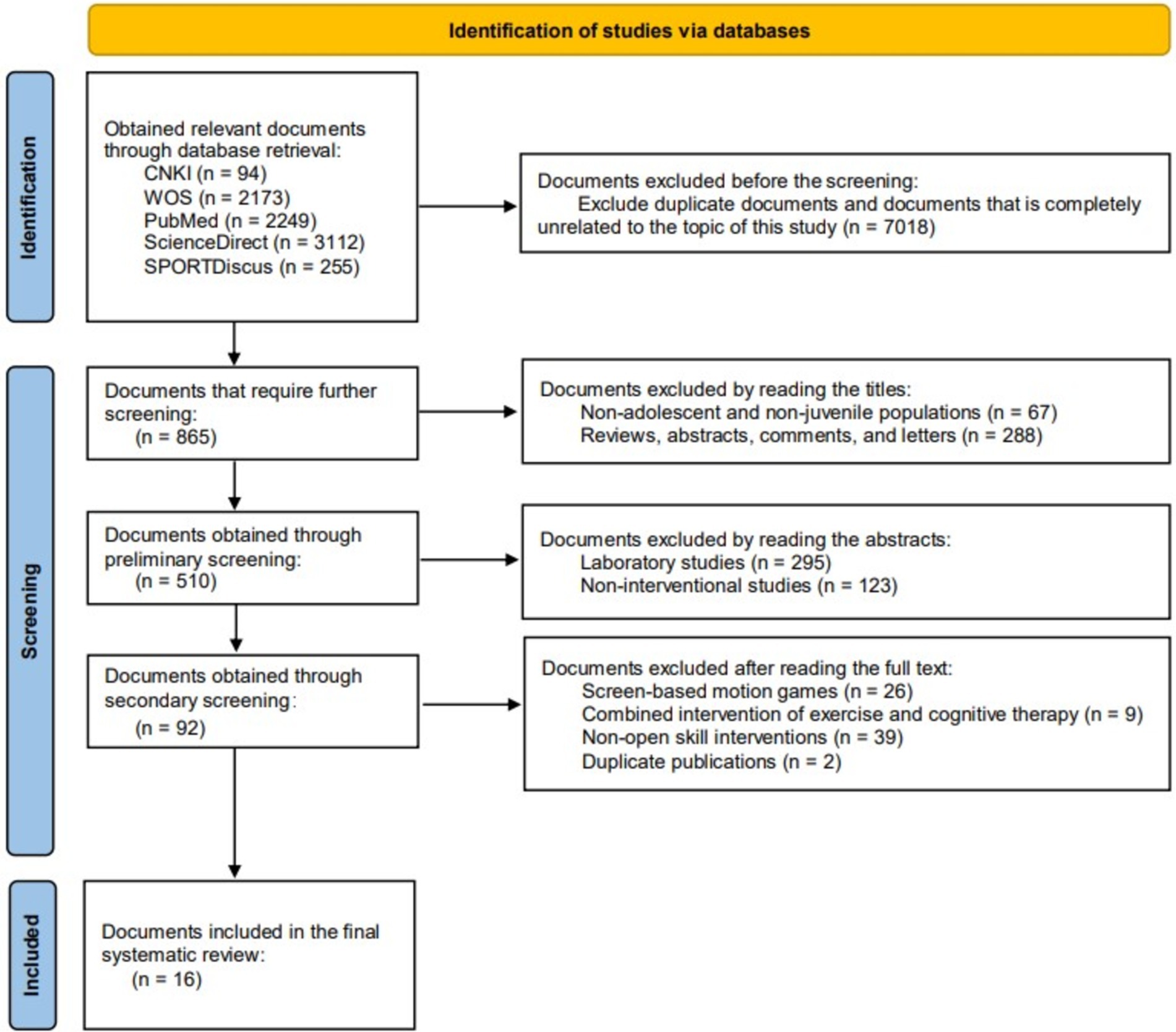
Figure 1. Flowchart of the screening process.
4.2 Basic characteristics of the included studies 4.2.1 Bibliographic information and study designChang et al. (2013) explored the effects of low and moderate intensity exercise interventions. To estimate the effect size, this study extracted data from different intensity interventions in that literature, meaning the literature includes two sub- studies, thus a total of 17 studies were included. The publication dates of the included studies ranged from 2013 to 2022, including 11 randomized controlled trials (RCTs) and 6 quasi-experimental designs (QEDs).
4.2.2 Characteristics of the participantsIncluded studies comprised a total of 1,298 participants, with the smallest sample size being 13 (Chang et al., 2013) and the largest being 460 (Pesce et al., 2016), averaging a sample size of 76. Participant ages ranged from 5 to 16 years old, with 9 studies involving participants aged 5 to 9 years (Chang et al., 2013; Crova et al., 2014; Jiang and Zeng, 2015; Alesi et al., 2016; Pesce et al., 2016; Chen et al., 2017; Lai et al., 2020; Ma et al., 2022), and 8 studies involving participants aged 10 to 16 years (Lakes et al., 2013; Schmidt et al., 2015; Martín-Martínez et al., 2015; Cho et al., 2017; Dai, 2020; Pan et al., 2016; Yin et al., 2017; Chou et al., 2020). The proportion of female participants in the included studies varied from 0.0 to 62.3%, with 5 studies (Jiang and Zeng, 2015; Dai, 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017) not reporting the proportion of female participants. Participant nationalities included China (Chang et al., 2013; Jiang and Zeng, 2015; Chen et al., 2017; Dai, 2020; Lai et al., 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017; Chou et al., 2020), Italy (Crova et al., 2014; Alesi et al., 2016; Pesce et al., 2016), the United States (Lakes et al., 2013), Switzerland (Schmidt et al., 2015), Spain (Martín-Martínez et al., 2015), and South Korea (Cho et al., 2017). There were 11 studies (Chang et al., 2013; Jiang and Zeng, 2015; Chen et al., 2017; Dai, 2020; Lai et al., 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017; Chou et al., 2020; Cho et al., 2017) involving Eastern populations and 6 studies (Crova et al., 2014; Alesi et al., 2016; Pesce et al., 2016; Lakes et al., 2013; Schmidt et al., 2015; Martín-Martínez et al., 2015) involving Western populations.
4.2.3 Intervention and control measuresThis study mainly adopts interventions through single sports such as soccer (Chang et al., 2013; Jiang and Zeng, 2015; Alesi et al., 2016; Chen et al., 2017; Dai, 2020; Ma et al., 2022), basketball (Pan et al., 2016; Yin et al., 2017), tennis (Crova et al., 2014; Lai et al., 2020), and taekwondo (Lakes et al., 2013; Cho et al., 2017). There are also studies (Schmidt et al., 2015; Martín-Martínez et al., 2015; Pesce et al., 2016; Chou et al., 2020) that use a variety of game-like sports to develop dynamic coordination and cognitive functions. According to the classification of open skills, there are 13 studies (Chang et al., 2013; Jiang and Zeng, 2015; Alesi et al., 2016; Chen et al., 2017; Dai, 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017; Schmidt et al., 2015; Martín-Martínez et al., 2015; Pesce et al., 2016; Chou et al., 2020) that use strategic skills for intervention; there are 4 studies (Crova et al., 2014; Lai et al., 2020; Lakes et al., 2013; Cho et al., 2017) that use interceptive skills for intervention.
In the included studies, 14 studies (82.35%) reported the intensity of the exercise intervention, among which one study (Chang et al., 2013) used low-intensity intervention; 12 studies (Chang et al., 2013; Crova et al., 2014; Jiang and Zeng, 2015; Martín-Martínez et al., 2015; Pesce et al., 2016; Chen et al., 2017; Cho et al., 2017; Dai, 2020; Lai et al., 2020; Pan et al., 2016; Yin et al., 2017; Chou et al., 2020) used moderate-intensity intervention; one study (Schmidt et al., 2015) used high-intensity intervention. The intervention period ranged from 6 weeks (Schmidt et al., 2015) to 36 weeks (Lakes et al., 2013), with 9 studies (Chang et al., 2013; Jiang and Zeng, 2015; Schmidt et al., 2015; Martín-Martínez et al., 2015; Chen et al., 2017; Lai et al., 2020; Pan et al., 2016; Chou et al., 2020) between 6 to 10 weeks; and 8 studies (Lakes et al., 2013; Crova et al., 2014; Alesi et al., 2016; Pesce et al., 2016; Cho et al., 2017; Dai, 2020; Ma et al., 2022; Yin et al., 2017) between 16 to 36 weeks.
The intervention frequency ranged from once a week (Crova et al., 2014; Pesce et al., 2016) to five times a week (Cho et al., 2017; Dai, 2020). Among them, there were 11 studies with a frequency of 1 to 2 times per week (Chang et al., 2013; Lakes et al., 2013; Crova et al., 2014; Jiang and Zeng, 2015; Schmidt et al., 2015; Martín-Martínez et al., 2015; Alesi et al., 2016; Pesce et al., 2016; Chen et al., 2017; Lai et al., 2020); and 6 studies with a frequency of 3 to 5 times per week (Cho et al., 2017; Dai, 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017; Chou et al., 2020). The duration of each session ranged from 30 min per session (Pan et al., 2016; Yin et al., 2017) to 120 min per session (Crova et al., 2014; Dai, 2020). Specifically, there were 2 studies with a duration of 30 min per session (Pan et al., 2016; Yin et al., 2017); 12 studies with a duration of 30 to 60 min per session (Chang et al., 2013; Lakes et al., 2013; Jiang and Zeng, 2015; Schmidt et al., 2015; Martín-Martínez et al., 2015; Pesce et al., 2016; Chen et al., 2017; Cho et al., 2017; Lai et al., 2020; Ma et al., 2022; Chou et al., 2020); and 3 studies with a duration of 75 to 120 min per session (Crova et al., 2014; Alesi et al., 2016; Dai, 2020).
The control measures included traditional physical education classes (Lakes et al., 2013; Crova et al., 2014; Schmidt et al., 2015; Alesi et al., 2016; Pesce et al., 2016; Chen et al., 2017; Pan et al., 2016; Chou et al., 2020), basic academic courses (Lai et al., 2020), aerobic exercises (Martín-Martínez et al., 2015), and a no-treatment control group (Jiang and Zeng, 2015; Cho et al., 2017; Dai, 2020; Ma et al., 2022; Yin et al., 2017).
4.2.4 Outcome variables15 studies have explored the effects of open-skill exercise interventions on inhibitory control. Among them, 10 studies used reaction time to assess task performance, including the Flanker task (Chang et al., 2013; Schmidt et al., 2015; Chen et al., 2017; Dai, 2020; Pan et al., 2016; Yin et al., 2017), Hearts-and-Flowers task (Lakes et al., 2013), GO/NOGO (Ma et al., 2022), and Stroop (Chou et al., 2020); 5 studies used accuracy to assess task performance, including the Flanker (Chang et al., 2013), Hearts-and-Flowers task (Lakes et al., 2013), Stroop (Martín-Martínez et al., 2015), and GO/NO GO (Ma et al., 2022); 4 studies used scores to assess task performance, including RNG (Crova et al., 2014; Pesce et al., 2016) and Stroop (Jiang and Zeng, 2015; Cho et al., 2017). 12 studies have investigated the effects of open-skill exercise interventions on working memory. Among them, 6 studies used reaction time to assess task performance, including 1-back (Chen et al., 2017; Lai et al., 2020; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017) and 2-back (Dai, 2020; Ma et al., 2022); 2 studies used accuracy to assess task performance, including 1-back (Schmidt et al., 2015; Ma et al., 2022) and 2-back (Ma et al., 2022); 5 studies used scores to assess task performance, including RNG (Crova et al., 2014; Pesce et al., 2016), Corsi blocks test (Jiang and Zeng, 2015; Alesi et al., 2016), Digital and letter span (Martín-Martínez et al., 2015), Forward Digit Span (Alesi et al., 2016), and Backward Digit Span (Alesi et al., 2016). 9 studies have explored the effects of open-skill exercise interventions on cognitive flexibility. Among them, 8 studies used reaction time to assess task performance, including the Hearts-and-Flowers task (Lakes et al., 2013), More-odd shifting (Schmidt et al., 2015; Chen et al., 2017; Ma et al., 2022; Pan et al., 2016; Yin et al., 2017), Trail Making Test (Martín-Martínez et al., 2015), and Salthouse (Dai, 2020); 2 studies used accuracy to assess task performance, including the Hearts-and-Flowers task (Lakes et al., 2013) and More-odd shifting (Ma et al., 2022); 1 study used scores to assess task performance, including the flexible item selection task (Jiang and Zeng, 2015).
The basic information of the included studies is detailed in Table 1.
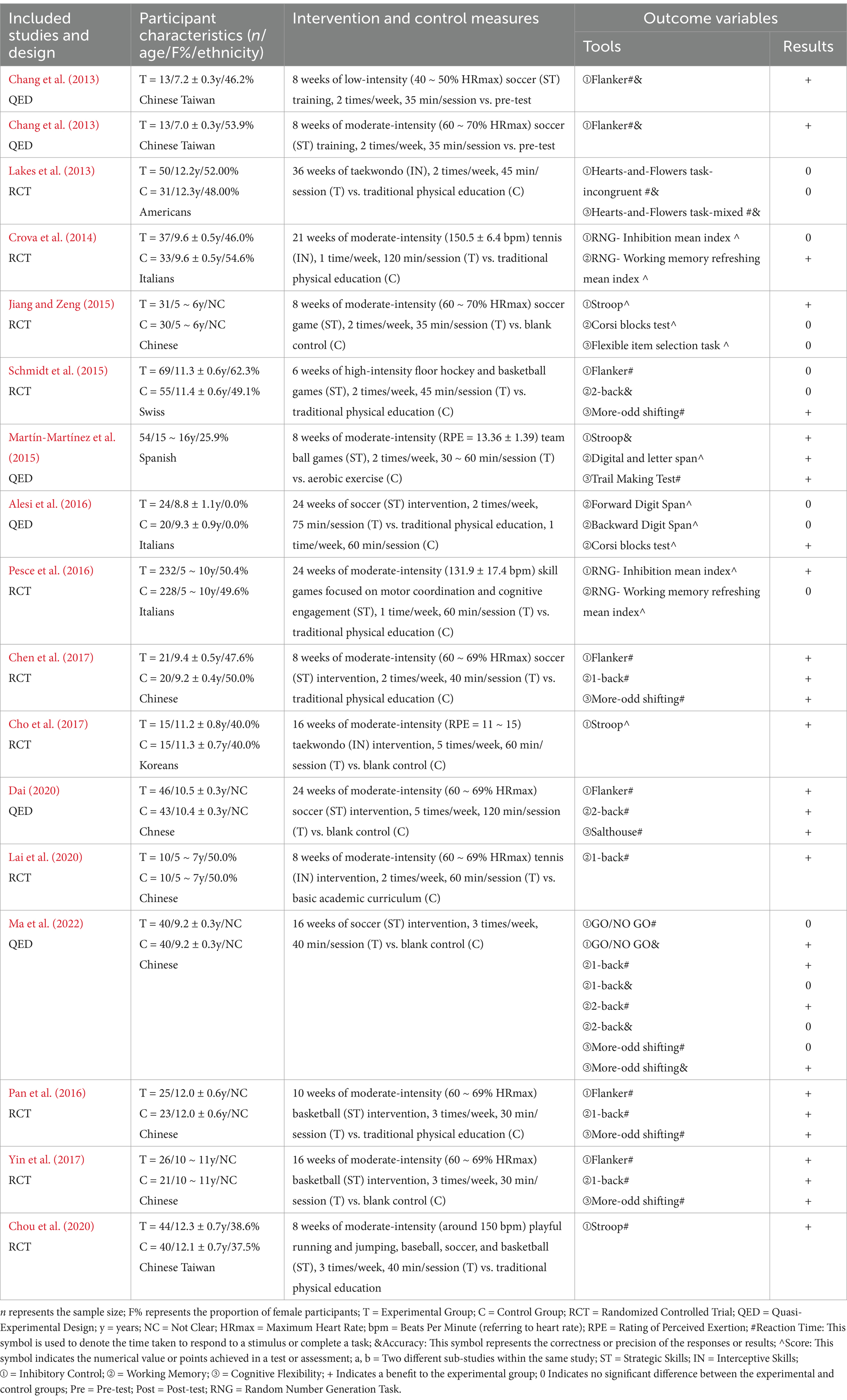
Table 1. Summary of original data information included in the meta-analysis.
4.3 Quality assessment resultsIn the 11 RCTs, 4 studies reported on randomization methods, mainly including whole group randomization (Crova et al., 2014; Pan et al., 2016; Pesce et al., 2016) and lottery method (Chen et al., 2017). Five studies reported on the implementation strategies of blinding, mainly including blinding of assessors (Lakes et al., 2013; Schmidt et al., 2015) and double blind (Chen et al., 2017; Lai et al., 2020; Chou et al., 2020). Six studies reported on the completeness of outcome data, indicating no participant dropouts or missing participants. Five studies reported participant dropouts, with the dropout sample ranging from 7 to 17 cases. Additionally, no study detailed the strategy of allocation concealment, and there was no instance of selective reporting of study results, and it is unclear whether other biases exist. The quality assessment results of the RCTs are detailed in Table 2. The quality scores of the six QEDs ranged from 17 to 19, and the quality of the included literature was relatively high (Table 3). The main reasons for the lower quality scores were that the endpoint indicator evaluation was not implemented using a blinded method, sample size was not estimated, the proportion of dropouts/missed visits was >5% and the reasons for presentation/missed visits were not stated.
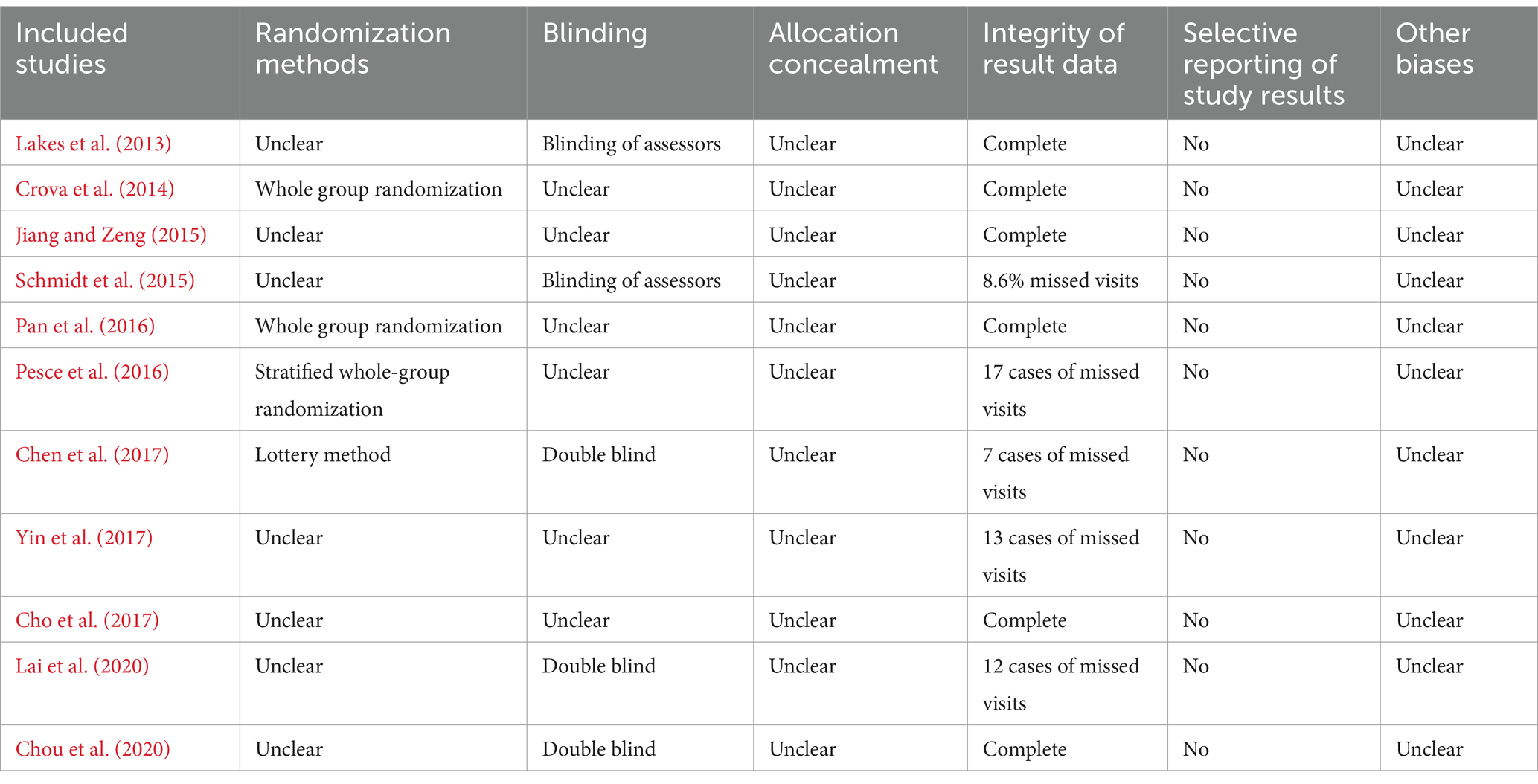
Table 2. Results of risk of bias assessment for RCT studies.
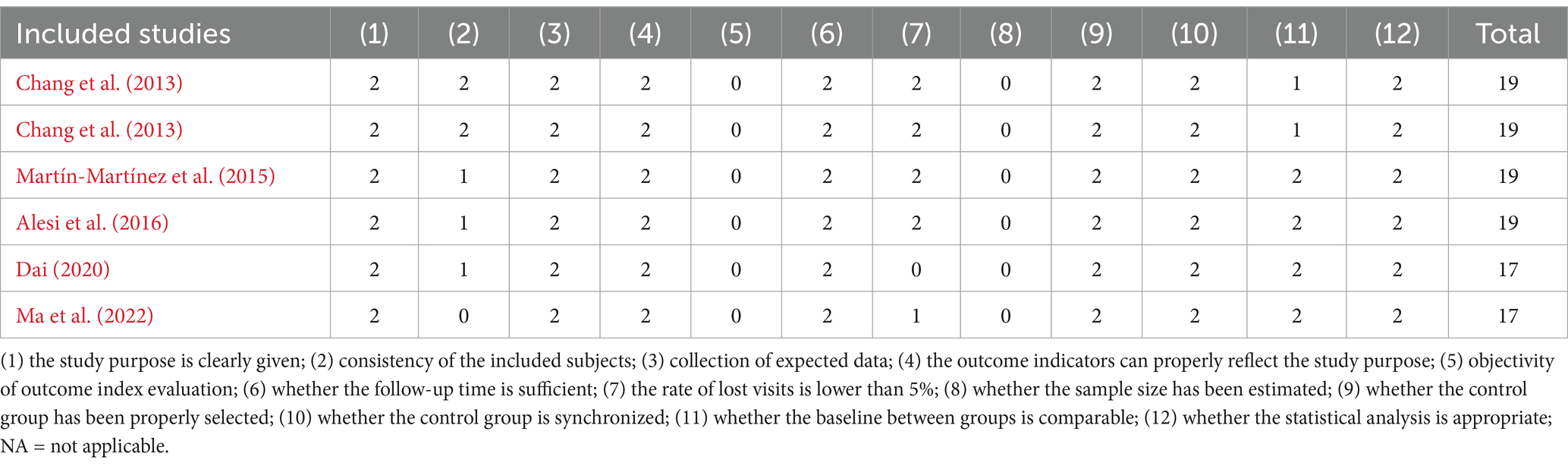
Table 3. Results of risk of bias assessment for QED studies.
4.4 Main effect testsThe studies on the effects of open-skill exercise interventions on inhibitory control, working memory, and cognitive flexibility all exhibit high heterogeneity (I2 > 80%, p < 0.01), hence a random-effects model was used for the main effect test. The results (Table 4) show that open-skill exercise interventions have positive effects (p < 0.01) on inhibitory control (SMD = −0.627, 95%CI = −0.890 to −0.363), working memory (SMD = −0.517, 95%CI = −0.768 to −0.266), and cognitive flexibility (SMD = −0.652, 95%CI = −1.085 to −0.219).

Table 4. The effects of open-skill exercise intervention on the executive functions of children and adolescents.
4.5 The moderating effect of open-skill typesThe examination of the moderating effect of open-skill types (Table 5) shows that there is a moderating effect of open-skill types on the effect of exercise intervention in inhibitory control (Q = 15.86, p < 0.01). Specifically, strategic skill exercise intervention has a positive effect on inhibitory control (SMD = −0.707, 95%CI = −0.819 to −0.594), while the effect of interceptive skill exercise intervention is not significant (p > 0.05). There is no moderating effect of open-skill types on the effects of exercise intervention on working memory and cognitive flexibility (p > 0.05), but both strategic and interceptive skill exercise interventions have positive effects (p < 0.05).
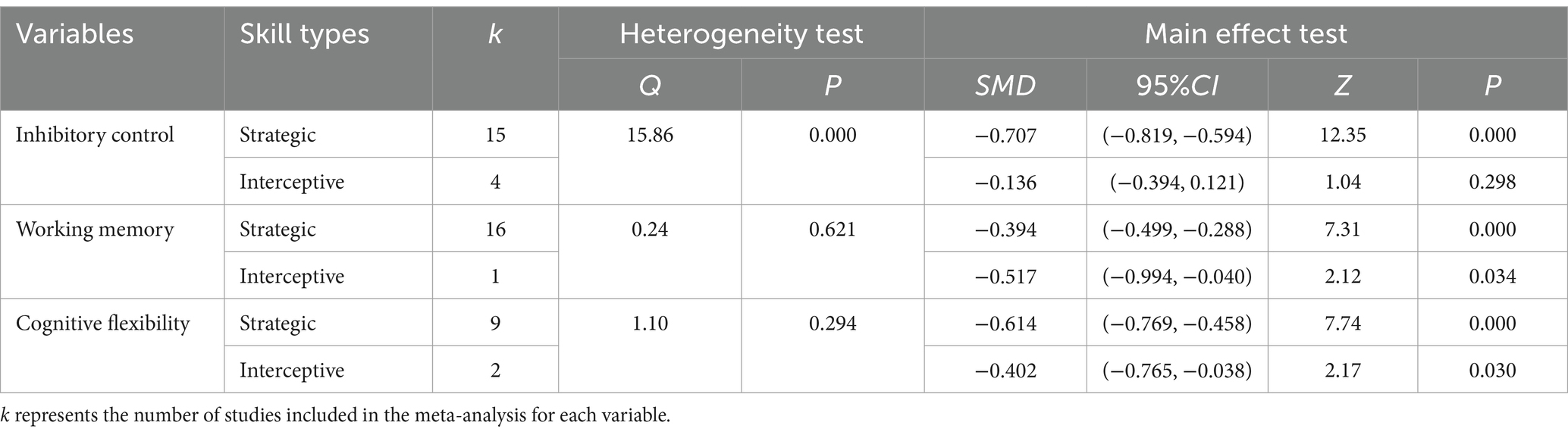
Table 5. Examination of the moderating effect of open-skill types.
4.6 The moderating effect of quantitative intervention elementsFirstly, the intensity level plays a moderating role in the effect of open-skill exercise interventions on inhibitory control (Q = 15.10, p < 0.01), with moderate intensity showing a positive intervention effect (SMD = −0.762, 95%CI = −0.886 to −0.638), while low and high intensities do not show significant intervention effects (p > 0.05). Additionally, moderate intensity has positive intervention effects (p < 0.01) on working memory (SMD = −0.504, 95%CI = −0.635 to −0.372) and cognitive flexibility (SMD = −0.750, 95%CI = −0.956 to −0.543), while high intensity does not significantly affect working memory (p > 0.05). Secondly, the period of the intervention has a moderating effect on the efficacy of open-skill exercise interventions for working memory (Q = 7.72, p < 0.01), with both 6 to 10 weeks and 16 to 36 weeks showing positive intervention effects (p < 0.01), but the 6 to 10 weeks period having a higher effect size (SMD = −0.653, 95%CI = −0.860 to −0.447). Furthermore, both periods significantly affect inhibitory control and cognitive flexibility (p < 0.01).
Thirdly, The frequency of exercise has a moderating effect on the efficacy of open-skill exercise interventions for inhibitory control (Q = 4.08, p < 0.05), with both 1 to 2 times per week and 3 to 5 times per week showing positive intervention effects (p < 0.01), but 3 to 5 times per week having a higher effect size (SMD = -0.782, 95%CI = -0.973 to −0.590). Both frequencies significantly affect working memory and cognitive flexibility (p < 0.01). Finally, the duration of each exercise session has a moderating effect on the efficacy of open-skill exercise interventions for working memory (Q = 24.03, p < 0.01) and cognitive flexibility (Q = 16.84, p < 0.01), with all durations from 30 min, 30 to 60 min, and 75 to 120 min showing positive intervention effects, but 30 min showing a higher effect size for working memory (SMD = −1.461, 95%CI = −1.918 to −1.005), and 75 to 120 min for cognitive flexibility (SMD = −1.474, 95%CI = −1.944 to −1.004); moreover, all durations significantly affect inhibitory control (p < 0.01). The test for the moderating effect of quantitative intervention elements is detailed in Table 6.
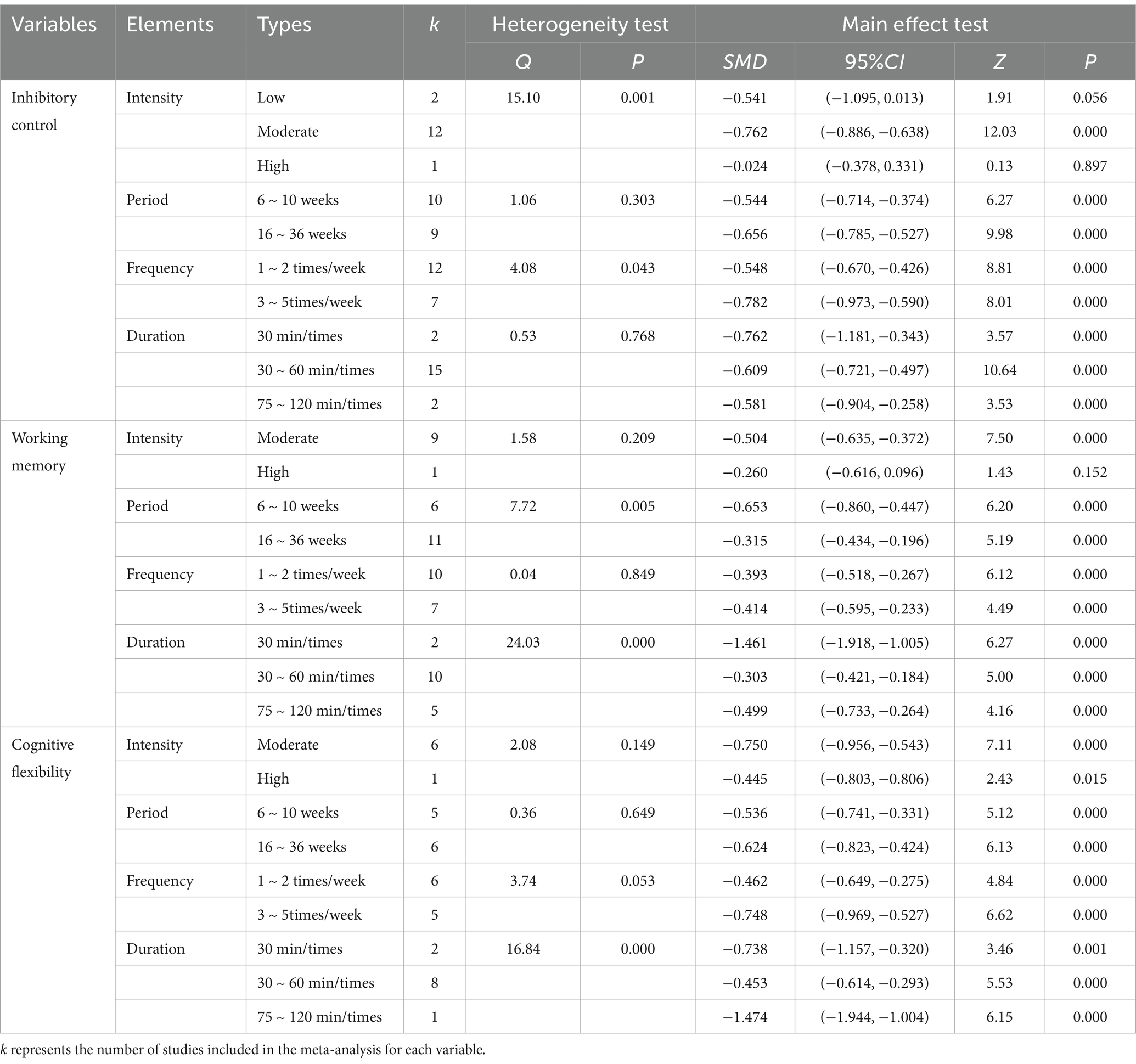
Table 6. Examination of the moderating effect of quantitative intervention elements.
4.7 The moderating effect of demographic variablesFirstly, age has a moderating effect on the efficacy of open-skill exercise interventions on inhibitory control and working memory (p < 0.01). Although open-skill exercises have positive intervention effects on both inhibitory control and working memory for the 5 to 9 and 10 to 16 age groups (p < 0.01), the promotion effect on inhibitory control is more pronounced for the 5 to 9 age group (SMD = −0.764, 95%CI = −0.901 to −0.627), and the promotion effect on working memory is more pronounced for the 10 to 16 age group (SMD = −0.758, 95%CI = −0.960 to −0.555). Additionally, open-skill exercises have positive intervention effects on cognitive flexibility for both the 5 to 9 and 10 to 16 age groups (p < 0.01). Secondly, ethnicity has a moderating effect on the efficacy of open-skill exercise interventions on inhibitory control (p < 0.01). Although open-skill exercises have positive intervention effects on inhibitory control for both Eastern and Western groups (p < 0.01), the promotion effect on inhibitory control is more pronounced for the Eastern group (SMD = −0.831, 95%CI = −0.991 to −0.671). Furthermore, open-skill exercises have positive intervention effects on working memory and cognitive flexibility for both Eastern and Western groups (p < 0.01). The moderating effects of age and ethnicity
留言 (0)