In this study, we found that the prevalence of significant CAD detected by CCTA was significantly higher among asymptomatic adults with newly detected DM than those without DM. Participants with newly detected DM and coronary artery stenosis also had a higher number of coronary vessels with significant obstruction, indicating a greater extent of CAD. Independent risk factors for CAD included age, gender, elevated low-density lipoprotein levels, and the presence of DM, aligning with established ASCVD risk factors [27].
Type 2 DM significantly increases ASCVD risk through mechanisms including endothelial dysfunction, oxidative stress, and chronic inflammation [28]. Diabetic dyslipidemia, characterized by elevated triglycerides, small dense low-density lipoprotein, and reduced high-density lipoprotein levels, accelerates atherosclerosis. Insulin resistance further impairs lipid metabolism, contributing to plaque buildup in arteries. Endothelial dysfunction, driven by the overproduction of advanced glycation end-products and reactive oxygen species, reduces nitric oxide and increases vascular inflammation. Additionally, a deficiency in protective adipokines exacerbates vascular stiffness and plaque vulnerability. This combination of metabolic and vascular disturbances explains the increased ASCVD risk in DM patients, even though the extent to which DM is considered a ‘major CAD risk factor’ or a ‘CAD risk equivalent’ remains debated [29, 30].
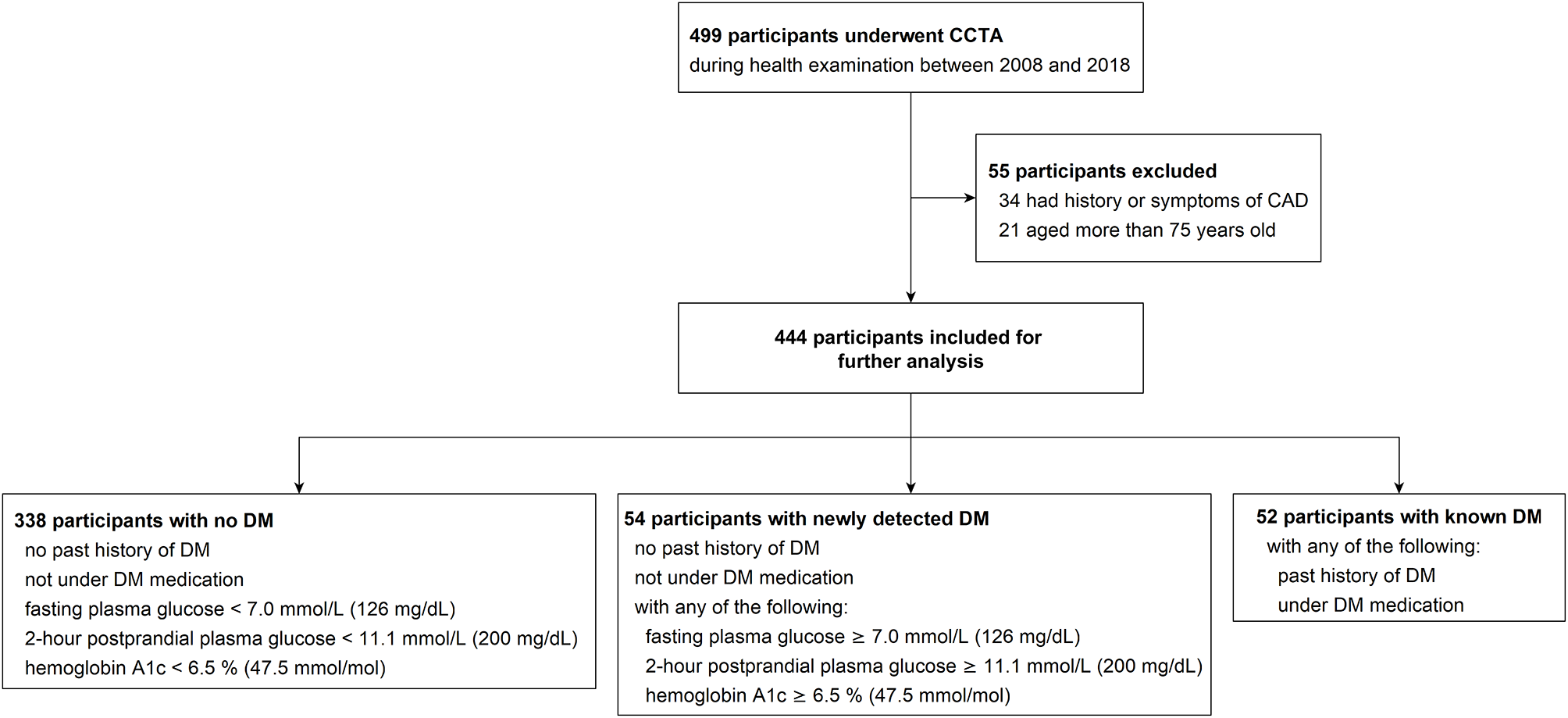
The delay between the onset of hyperglycemia and the diagnosis of DM is common and is estimated to be 4–6 years on average [31]. During this period, both microvascular and macrovascular complications can develop and progress before DM is formally diagnosed. While microvascular complications at DM diagnosis have been well-documented, such as diabetic nephropathy in 18.2% and retinopathy in 25.5%8, the epidemiology of CAD at DM diagnosis is much less frequently described. A prior study with 44 asymptomatic patients diagnosed with DM within 1 year found higher coronary artery calcification rates compared to matched controls (66% vs. 48%, p < 0.05), but no significant difference in the prevalence of coronary obstruction (≥ 70% stenosis) (9.1% vs. 6.8%, p = 0.50) with the use of CCTA [17]. In our study, with a larger sample size, we found a significantly higher prevalence of significant CAD (≥ 50% stenosis) in participants with newly detected DM compared to those without DM (40.7% vs. 20.1%, p < 0.0001), suggesting that CAD, similar to microvascular complications, may develop before DM is detected.
For patients with established DM, studies have shown a correlation between the duration of hyperglycemia and increased risks of CAD. Gurudevan et al. found a higher prevalence of obstructive CAD (≥ 60% stenosis) in participants with impaired fasting glucose compared to those with normal fasting glucose (29.5% vs. 13.3%, p = 0.02) [32]. Kim et al. demonstrated that a longer duration of DM was associated with a greater risk of significant CAD (≥ 50% stenosis) (49.1%, 29.6%, and 28.3% in patients with DM duration ≥ 10 years, 5–10 years, and < 5 years, respectively, p < 0.001) [33]. These findings imply that, beyond the initial elevated CAD risk at DM diagnosis, the risk continues to increase with time.
The scarcity of epidemiology data on CAD at the time of DM diagnosis may be due to the lack of observed benefit in previous clinical trials and the current guidelines that do not recommend routine screening for CAD in asymptomatic DM patients [4, 19]. CCTA provides detailed information on plague distribution and vascular stenosis and has been shown to improve risk stratification for CAD [14, 15], even in asymptomatic patients with DM [34, 35]. However, its routine use for screening CAD in asymptomatic patients is not supported by current evidence [19]. Furthermore, the risks associated with CCTA, including radiation exposure and the use of contrast medium [36], make it less favorable as a universal screening tool. Alternatively, other methods, such as common carotid artery intima-media thickness (CIMT), have been found to be increased in patients with newly diagnosed type 2 DM [37], correlating with the presence and severity of CAD in asymptomatic DM patients [38]. Similarly, the reactive hyperemia index (RHI) [39] and ankle-brachial index (ABI) [40] have demonstrated predictive value for CAD in patients with type 2 DM, offering more affordable and accessible options for assessing cardiovascular risk in primary care settings. Additionally, risk stratification tools including the ASCVD risk score [27], which rely on readily available clinical data, remain valuable for guiding prevention strategies at the population level.
As ASCVD remains the leading cause of morbidity and mortality in DM [12, 13], its importance cannot be emphasized enough by both patients and clinicians. The finding of a 40.7% prevalence of significant CAD in participants with newly detected DM highlights the need for continued research into screening and managing CAD in this population, especially as the detection techniques and management strategies continue to evolve. Also, this study is the first to report data on CAD prevalence in newly detected DM in the Asian population, providing a foundation of future population-based guideline development.
Several limitations should be noted. First, data were collected from a single medical center, and CCTA was performed based on participants’ preferences, which may have introduced selection bias related to self-concern and socioeconomic status. However, the age and gender distribution of newly detected DM participants aligns with nationwide data in Taiwan [41]. Second, information on plaque composition and burden was missing in some of the CCTA reports, limiting further analysis of plaque characteristics. Nevertheless, the data on coronary stenosis were complete, allowing significant findings to be derived. Similarly, information about chronic medication was incomplete, while the biological effect of some of the medication was analyzed, such as lipid profiles for lipid-lowering medications. Other potential confounders, including lifestyle and diet, were not assessed. Third, although participants labeled as newly detected DM met at least one diagnostic criterion, more information is needed to confirm the diagnosis. As a cross-sectional study, follow-up data was unavailable. Finally, this study focused on CCTA for its ability to directly visualize coronary artery stenosis. However, it is important to note that alternative methods, including CIMT, RHI, ABI, and cardiovascular risk scores, may be more practical for large-scale screening due to their cost-effectiveness and ease of implementation. Future studies should compare these methods directly to assess their relative strengths in detecting CAD in newly diagnosed DM patients. Further investigation is also needed to elucidate the progression of CAD in patients with DM.






留言 (0)