The current prospective nationwide cohort study shows that obesity prior to 10 years of age more than doubles the risk of MS regardless of MS heredity, compared to general population comparators. This study also confirms that obesity in adolescence increases the risk for MS. Additionally, this study suggests a dose-response relationship between degree of obesity and the risk for MS.
In the present study, the estimated risk of obesity on MS was more than double, which is in line with previous studies in adults [6, 15, 17] and studies with retrospective design with self-reported or estimated weight data from pediatric years [10,11,12]. The proportion of males and females that were diagnosed with MS were similar, which was mirrored in the hazard ratio estimates, indicating that obesity affects MS equally in males and females.
This study found that, compared to the general population, class I obesity did not significantly increase the risk for MS, while class II obesity showed a pronounced risk, indicating a dose-response relationship. The underlying mechanism may be attributed to obesity’s role in inducing a persistent, low-grade inflammatory state characterized by elevated levels of proinflammatory cytokines [2]. Type of diet and microbiota may also contribute both to obesity and MS [7]. A study in mice suggest that high-fat diet induced obesity causes a pro-inflammatory micro-environment which promotes CNS inflammation through proliferation and activation of encephalitogenic T cells into the CNS [24]. A cross-sectional study in humans suggest that leptin, typically high in individuals with obesity, promotes autoreactive T-cell proliferation and proinflammatory cytokine secretion [10]. Further, obesity-induced gut microbiota dysregulation has been shown to shift the balance between proinflammatory and anti-inflammatory responses, suggesting that it might act as a link between obesity and MS [22, 25]. Consequently, the proinflammatory condition in obesity most likely amplifies the immune response and thereby increases the risk of developing autoimmune inflammatory disorders, such as MS.
Some case reports have identified individuals developing symptoms of MS shortly after immense weight loss following bariatric surgery [26,27,28]. Conversely, anti-obesity medications based on glucagon-like peptide-1 receptor agonists appear to have a protective effect against the development of MS [29]. This suggests that weigh loss itself may not be a direct contributor to MS. In the present study, modest weigh loss after lifestyle behavioral treatment was not associated with increased risk of MS several year later. Over half of those who developed MS in the present study had class II obesity at their last recorded treatment visit, making direct comparisons to previously published reports challenging. Nevertheless, since obesity itself remains a significant factor contributing to MS risk, as demonstrated in this study, and is associated with MS progression and relapse [30, 31], prevention of high degree of obesity in childhood and adolescence is warranted.
Previous epidemiological research suggest that the association between early life high BMI and MS only is present for adolescent obesity and not childhood obesity [15,16,17]. However, studies using Mendelian randomization with estimated childhood BMI have suggested an effect of childhood BMI on subsequent MS risk [13, 14]. The current study extends these findings by using clinically obtained anthropometric measured in childhood. Consequently, the association between obesity and elevated risk of MS is shown to not be limited to adolescence but extends to childhood. Since treatment for pediatric obesity rarely results in obesity remission [19], it is plausible that early exposure to obesity leads to longer obesity duration. This may lead to a long-term pro-inflammatory response which could act as a catalyst, activating genes that are associated with the development of MS.
Parental MS was more common in the pediatric obesity cohort, which might give rise to a hypothesis of shared predisposition for MS and early obesity onset in the offspring. However, our study design prevents us from drawing any conclusions about causality. A genetic study, using Mendelian randomization, found little evidence of genetic pleiotropy between genes associated with high BMI in childhood and MS later in life [13], which contradicts a shared genetic predisposition. Another plausible explanation for this observation could be the strong hereditary nature of obesity. Consequently, parental BMI may be higher in the obesity cohort, potentially elevating the prevalence of parental MS. Future research should explore the potential synergistic relationship between MS heredity and childhood obesity in increasing MS risk. This research is vital for unraveling the intricate genetic and environmental interactions contributing to MS and obesity.
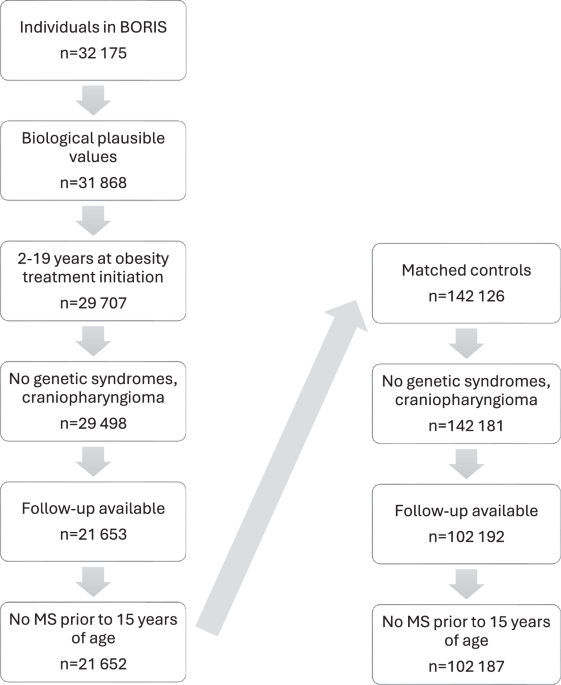
Despite the large-scale longitudinal study with individual-level data, some limitations should be acknowledged. Firstly, there are several risk factors known to be associated with MS that were not possible to control for, such as smoking, Epstein-Barr viral infection, and low vitamin D levels [16]. Secondly, no genetic data was available, but we were able to adjust for parental MS. Thirdly, as BORIS only includes anthropometric data from clinical visits, obesity duration prior to treatment cannot be determined. Fourthly, obesity status in the control group was unknown, which could cause an underestimation of obesity as a risk factor for MS. Fifthly, the median age at follow-up was 20.8 years of age, which should be kept in mind since MS typically develops between 20 and 40 years of age. Yet, we could observe an effect of pediatric obesity on MS.

留言 (0)