
記住我
The COVID-19 pandemic had negative consequences on the mental health of the general population; especially generalized anxiety disorder, whose post-pandemic prevalence increased by 25% (1). Clinically, GAD is expressed through excessive worry (anxious anticipation) about various events or activities. The intensity, duration, or frequency of GAD is often disproportionate to the actual likelihood or impact of an event (2).
Scientific evidence indicates that this disorder is closely linked to intense and difficult-to-manage stress situations. In many cases, worsening anxiety can lead to the onset of depressive symptoms (3); representing a clear indicator of psychological distress (4), with negative effects on both mental and physical health, and a direct impact on daily activities (5).
Additionally, anxiety often coexists with other disorders, such as depression, sleep disorders (6), and suicidal ideation (7, 8), acting as a trigger for multiple diseases (9, 10). This comorbidity not only intensifies anxiety symptoms but also prolongs their duration and reduces the effectiveness of interventions (11). Therefore, early detection is essential to mitigate its impact on mental health and develop prevention and treatment plans that minimize the occurrence of associated pathologies (12), alleviating the burden on the individual and facilitating recovery (3).
An economical, valid, and reliable way to detect GAD is through rapid tests. The Generalized Anxiety Disorder Test (GAD-7) (13), is a self-administered clinical scale used to assess generalized anxiety disorder over the past two weeks, according to DSM-V criteria (2). It is an instrument that is easy to apply, score, and interpret, with widespread use in hospital systems and strong support in the medical literature (14, 15).
The GAD-7 has demonstrated good clinical utility and excellent psychometric properties for quickly assessing GAD symptoms in international studies, showing adequate internal consistency (Cronbach’s Alpha >.70) (16, 17). During the COVID-19 pandemic, its use expanded to numerous studies worldwide (18–20). In Latin America and the Caribbean (LAC), it has also been applied, showing robust validity and reliability indicators (15, 21).
However, to date, no studies have provided evidence of the GAD-7’s invariance based on demographic characteristics in this region. This information is essential as it would strengthen the instrument’s validity for use in diverse populations within LAC. Therefore, the objective of this study was to evaluate the factorial invariance of the Generalized Anxiety Disorder Test considering gender and country of residence in a large sample of adults from the region.
2 Materials and methods2.1 ParticipantsAn e-Health study (22) was conducted using a snowball sampling methodology. Through social networks, personal, and institutional emails, the general population aged 18 and older from 15 countries in the region was invited to complete an online questionnaire. To ensure proper coordination of the project, an international research consortium established interinstitutional agreements with hospitals, civil and governmental organizations, universities, and professional associations.
A logistical framework was developed to form working teams in each country, which were specifically trained for the study. Institutional email databases were compiled, and the online questionnaire was distributed via email, social networks, and WhatsApp, encouraging its dissemination within the communities. Data collection began on May 12, 2022, and concluded on November 27, 2023.
Initially, 14,842 participants were evaluated. However, 2,718 were excluded for not completing the questionnaire, not signing the informed consent, not reporting their gender, or selecting countries where an adequate number of forms could not be collected. As a result, 12,124 forms were processed (54.32% women and 45.68% men) from Argentina (7.3%), Bolivia (6.7%), Colombia (10.3%), Chile (6.9%), Costa Rica (4.9%), El Salvador (5.7%), Ecuador (7.2%), Guatemala (4.7%), Panama (5.1%), Paraguay (5.7%), Peru (8.6%), Puerto Rico (5.8%), Dominican Republic (6.6%), Uruguay (6.3%), and Venezuela (8.2%). The average age of the participants was 31.14 years (SD: 8.78). The final sample included health professionals (12.5%), engineers and exact sciences (9.3%), social sciences (8.2%), legal, accounting, and administrative sciences (10.3%), education sciences (11.4%), university students (14.2%), and community members (34.1%).
The complementary data table provides detailed demographic information about the participants, distributed by countries, age ranges, and the proportion of male and female participants (Table 1). It is worth noting that the representation of other genders was below 0.2%. Due to the lack of statistical power and representativeness of these groups, the analysis focused exclusively on the information provided by male and female participants.
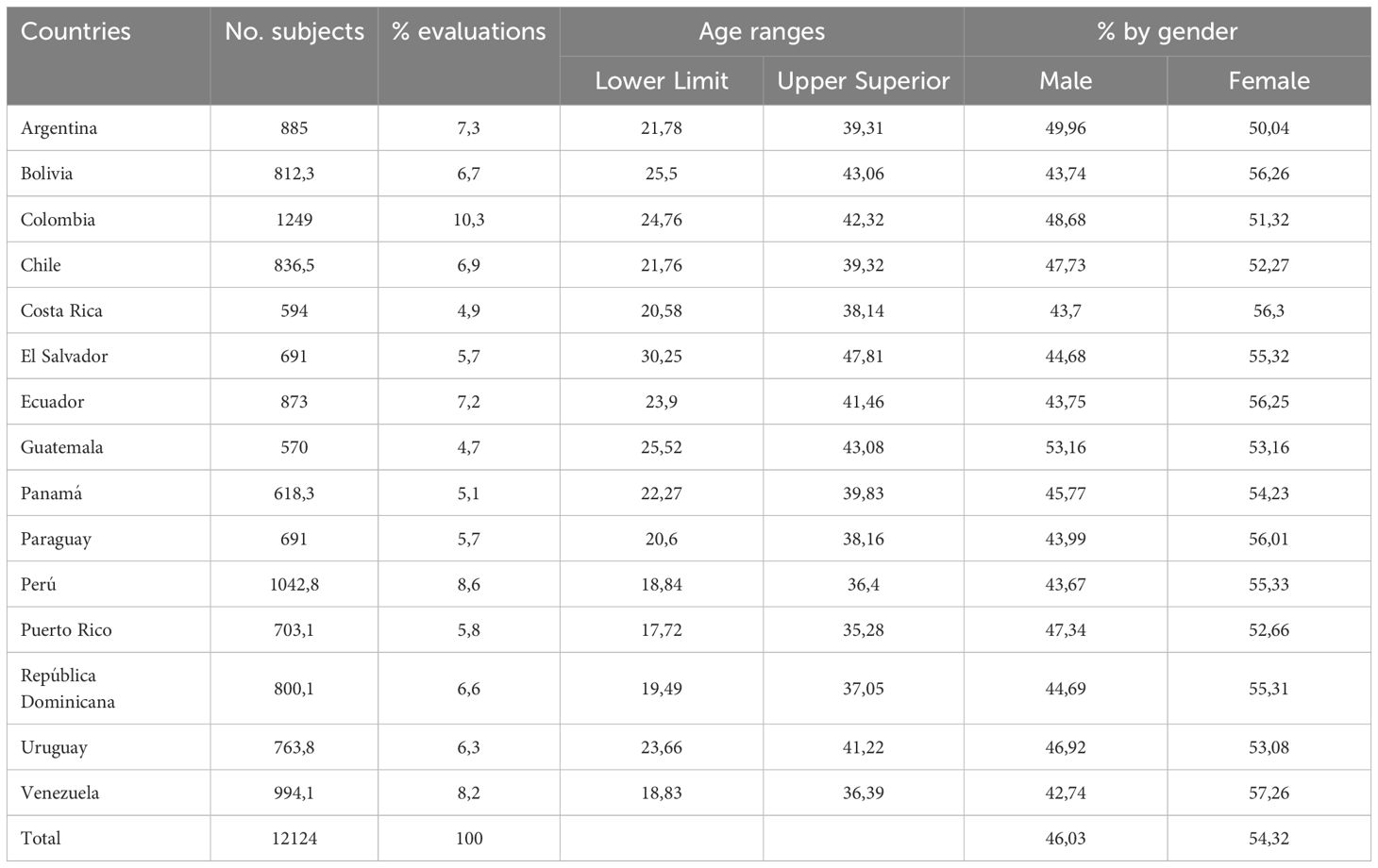
Table 1. Complementary data table: demographic information of the participants.
2.2 InstrumentsAn automated Google form was used, which provided information about the study’s objective, informed consent, along with demographic questions. Additionally, the GAD-7 was applied, which, through seven questions, allows for a quick assessment of the presence and severity of generalized anxiety disorder over the past two weeks (2, 13). The score ranges from 0 to 3 for each item, with response options being “Not at all,” “Several days,” “More than half the days,” and “Nearly every day.” The total GAD-7 score can range from 0 to 21, with a score of ≥10 indicating generalized anxiety disorder. It also allows for grading the severity of the disorder.
2.3 Data analysisThe data were digitized using Google Forms in a Google Spreadsheet. The database was downloaded as an xlsx file and imported into R software version 4.02 in its RStudio programming environment version 1.3.595 (23). The openxlsx (24) package was used for data import, and the tidyverse (25) and psych (26) packages were used for data preparation and analysis. The lavaan (27), semPlot (28), and semTools (29) packages were used for confirmatory factor analysis (CFA) and measurement invariance. The MBESS (30) packages were used for confirmatory factor analysis (CFA) and measurement invariance. The MBESS (31) package was used to calculate the winsorized correlation coefficient (tr. = 0.10). For the CFA, the Robust Weighted Least Squares Mean and Variance adjusted (WLSMV) estimator was used, and unidimensional structure was evaluated. For the evaluation of fit indices, the following criteria were considered: values ≥.90 and ≥.95 for CFI and TLI, as adequate and good fit, respectively; values ≤.08 and ≤.05 for RMSEA, as adequate and good fit, respectively; and for SRMR, values ≤.08 and ≤.06 were considered good and ideal fit, respectively. The decision to apply measurement invariance analysis instead of Differential Item Functioning (DIF) was based on the study’s objective to compare latent structures across different groups. While DIF analysis focuses on detecting item-level biases, measurement invariance evaluates whether the overall factorial structure of a scale is comparable across groups, ensuring that observed differences reflect true variations in the latent construct rather than measurement biases. This approach was deemed more suitable for evaluating the invariance of the psychometric model across gender and country groups, following the procedures proposed by Wu & Estabrook (31), and using established cutoff criteria (ΔCFI <.010, ΔTLI <.010, ΔSRMR <.030, and ΔRMSEA <.015) to determine invariance levels (32–34).
2.4 Ethical considerationsThe study adhered to the ethical standards of the relevant national and institutional committees and the Declaration of Helsinki of 1975, as revised in 2008. Informed consent was obtained online from all participants, who, upon completing the assessment, received a report of their results and a document containing psychological and clinical guidance. The protocol was approved by the Ethics Committee of Universidad de La Costa (Record No. 173 of May 27, 2024, research project code INV. 140-03-001-18).
3 ResultsIn Table 2, the descriptive statistics for the seven items of GAD are shown. It can be observed that item 5 has the lowest mean value, while item 3 has the highest mean value. Regarding Skewness and Kurtosis, these are close to zero, indicating that the data distribution is unlikely to affect subsequent analyses.
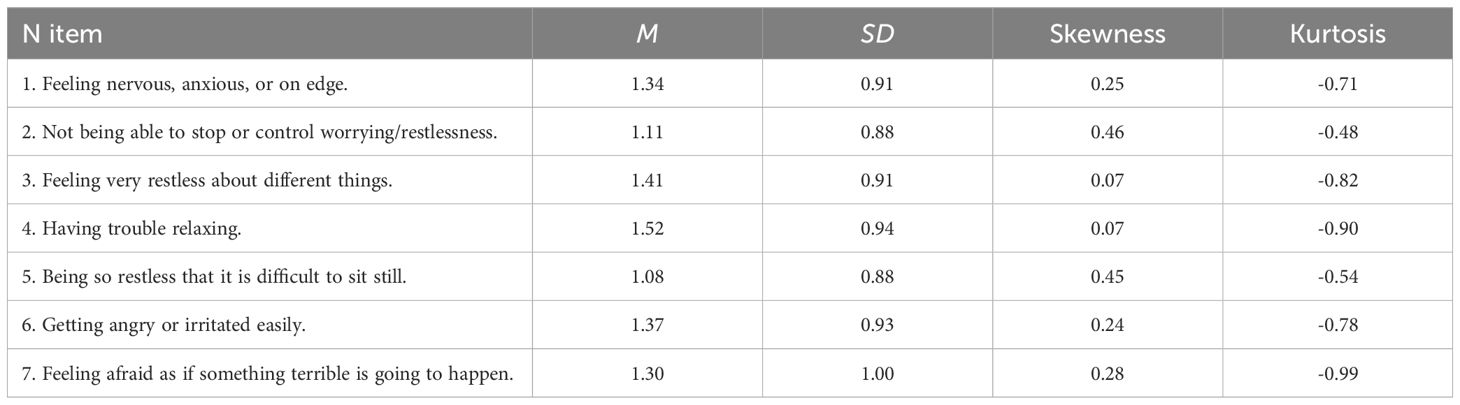
Table 2. Descriptive statistics for the GAD-7 Items.
Next, confirmatory factor analysis was conducted to study the internal structure of the GAD-7. The models analyzed and their fit indices are presented in Table 3. For the instrument, the unidimensional structure without correlated errors showed a good fit in the CFI, TLI, and SRMR indices. However, the RMSEA index indicated an inadequate fit; therefore, the model was re-specified by adding the covariance between item 1 and item 2, which reduced the RMSEA value, indicating an adequate fit (<.08) to the model. Moreover, a theoretical explanation is that GAD-7 items 1 and 2 measure closely related constructs within the domain of generalized anxiety. Item 1 (“Feeling nervous, anxious, or on edge”) and item 2 (“Not being able to stop or control worrying/disquiet”) reflect a common core of anxiety-related emotional arousal and intrusive thoughts (32). Both items target the core of generalized anxiety disorder, which is characterized primarily by excessive worry and difficulties in controlling those thoughts (33). Therefore, it is expected that they share a considerable portion of common variance, which explains the need to model this covariance.

Table 3. Analyzed models and fit indices.
Figure 1 presents the factor loadings of the model that showed the best fit for the GAD. In this case, the factor loadings were greater than.71, and the correlated error between item 1 and item 2 had a value of.31.
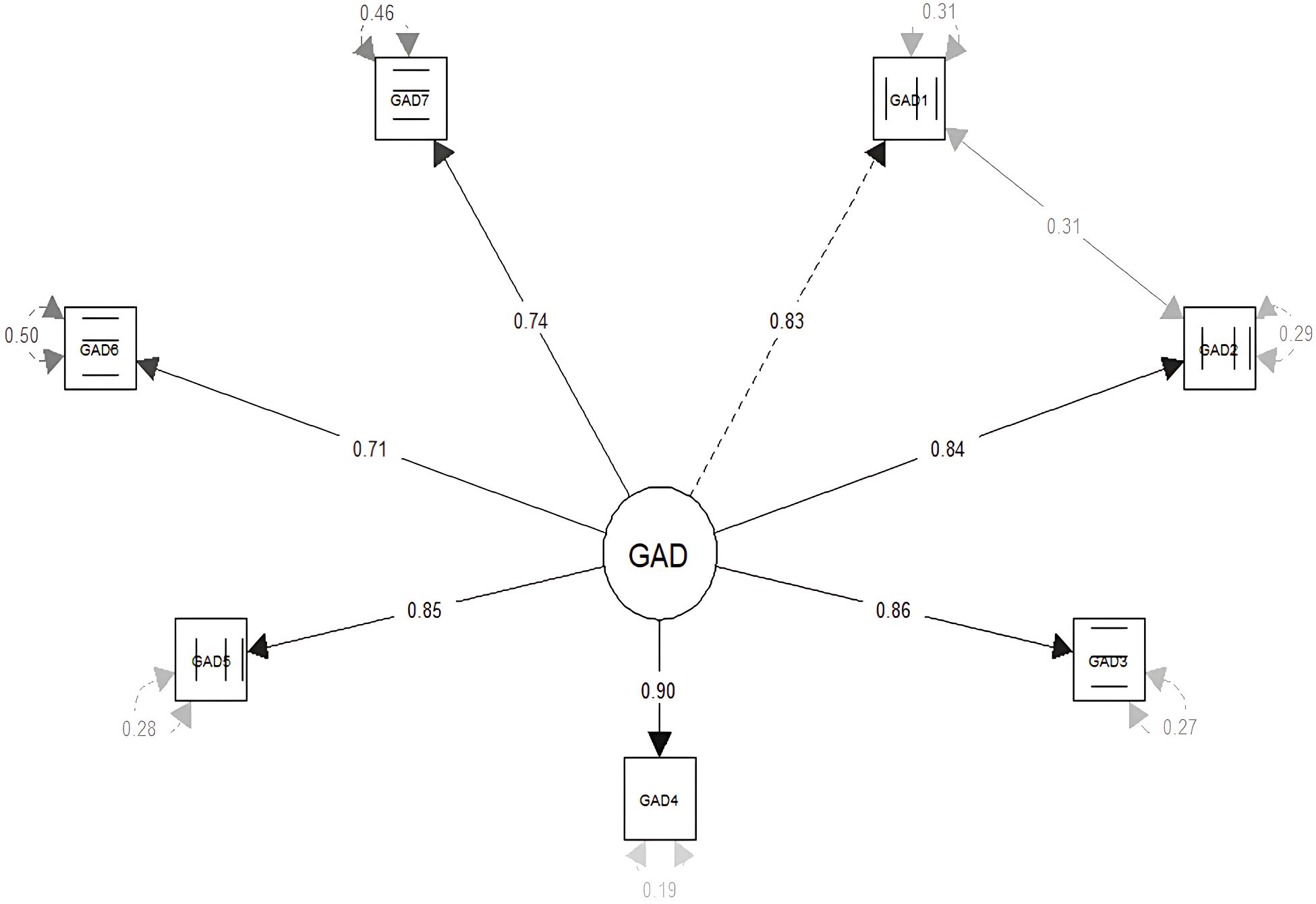
Figure 1. Factor loadings and correlated errors of the GAD-7.
Subsequently, the invariance of the GAD-7 measures was evaluated according to gender and country. As shown in Table 4, the invariance analysis reveals that the factor structure of the GAD-7 by gender showed fit indices ranging from adequate to good at the configural, threshold, metric, scalar, and strict levels. Additionally, the differences between the fit indices were smaller than the value established in the data analysis section, indicating that the factor structure of the instrument presents measurement invariance and is equivalent for both groups (men and women). The same results were observed when using the country as the comparison variable. It was found that the structure (configural), thresholds, factor loadings (metric), intercepts (scalar), and residuals (strict) were equivalent between the group.
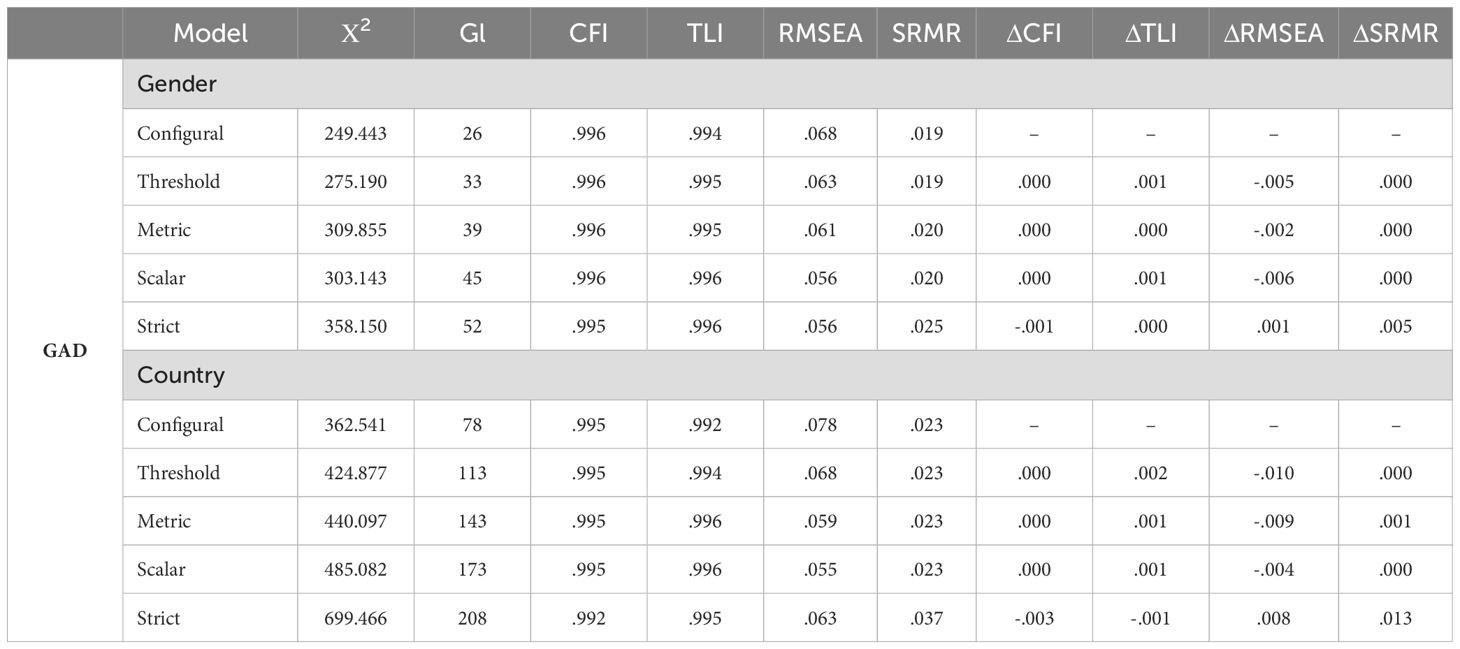
Table 4. Measurement invariance by gender and country.
Finally, McDonald’s Omega coefficient was applied to evaluate the internal consistency of the instrument. The value obtained for the GAD-7 test was ω = .91.
4 DiscussionWe analyzed the factor structure, and the reliability level of the GAD-7 test to detect GAD symptoms, considering the concepts of gender and country invariance, in a large sample of the surveyed population from LAC.
Factor analysis revealed that the GAD-7 has a unidimensional structure, explaining 70% of the variance and demonstrating adequate fit indices (RMSEA = 0.062, CFI = 0.997, TLI = 0.995, SRMR = 0.017). This confirms that the items of the instrument reflect a single factor of generalized anxiety. This finding aligns with international literature, which has consistently shown in various national contexts that the GAD-7 reliably measures a single factor associated with disorder symptoms (13, 34). Furthermore, multiple global studies have validated its reliability, establishing it as a key tool for both clinical practice and research (17, 20, 35, 36).
These results indicate that the GAD-7 can identify symptoms of generalized anxiety without the need to divide the items into subscales. The consistency of its factorial structure across different countries supports the instrument’s validity and reinforces its applicability at an international level, offering a standardized approach to detecting the disorder. This is particularly relevant in Latin America and the Caribbean, where reliable, accurate, and affordable tools are needed for the consistent detection of generalized anxiety.
Secondly, we demonstrated the factorial invariance of the GAD-7 considering participants’ gender and country of residence. The results indicate that the GAD-7 maintains equivalence at all levels (configural, metric, scalar, and strict), both between men and women and across the different countries evaluated. These findings are particularly significant, given that studies analyzing the stability of the instrument by gender and country remain limited (36); although the invariance of the instrument has been confirmed in other contexts (37–39).
In this context, the available evidence has demonstrated the usefulness of the GAD-7 in various settings across Latin America. The instrument has been used to identify symptoms of generalized anxiety in populations receiving healthcare services (14, 40, 41), university students (42–44), and the general population (36, 45, 46).
Finally, our study confirmed the high reliability of the GAD-7, as evidenced by an Omega coefficient of 0.91, which ensures the instrument’s ability to consistently detect GAD symptoms. Specifically, a value greater than 0.90 reflects a high degree of homogeneity among the test items, ensuring that each item contributes equally to measuring the construct’s structure. These findings align with previous studies conducted in various countries, which have also reported high internal consistency indices for the GAD-7 (16, 47–50).
These findings are particularly relevant in the Latin American context, where access to mental health services is limited. In this scenario, the GAD-7 stands out for its reliability and stability in measurement, exceeding the recommended threshold for evaluations in clinical practice. This makes it a fast and accurate tool that facilitates early diagnosis and timely interventions for the detection of GAD.
5 LimitationsAlthough this study presents adequate results, it has some limitations. First, construct validity was not assessed; however, the analyses showed that the GAD-7 has adequate internal consistency and a factorial structure invariant across gender and country. Second, the cross-sectional design limits the evaluation of changes in generalized anxiety levels over time. Future longitudinal studies would be valuable, particularly in a post-pandemic context. Third, no information was collected on premorbid state or prior mental health conditions, making it difficult to conduct more detailed causal analyses, such as case-control studies. Fourth, although the sample included several countries from Latin America and the Caribbean (LAC), it lacked representation of minority subgroups, such as Indigenous communities, rural areas, and economically vulnerable populations. This limits the understanding of the cultural applicability of the GAD-7 and its cultural equivalence, which could be improved by expanding the sample (44, 45). Fifth, factorial invariance by age was not analyzed, a relevant aspect since anxiety symptoms may vary across age groups. Finally, the use of self-reported data poses risks of response bias and limits the generalization of results. The absence of clinical variables and diagnostic interviews restricts clinical validation. Advanced methodologies, such as Differential Item Functioning (DIF) analysis, would be necessary to address potential cultural biases and improve accuracy in diverse populations.
Currently, the scale validation is based on self-reported data, which is a widely used approach in psychological and social sciences research. However, future studies should incorporate clinical validation using criterion-related measures (51), such as structured interviews or comparisons with established diagnostic tools. The inclusion of external validation criteria would ensure that the scores obtained through the scale are aligned with clinically recognized constructs (52), thereby increasing the scale’s applicability in both research and clinical settings.
Future research should aim to validate the scale using clinical criteria, such as structured interviews and comparisons with diagnostic tools, to strengthen the interpretative validity of the results. The inclusion of clinical background information, such as medication use and comorbidity, would provide a more comprehensive understanding of the population. Additionally, employing Item Response Theory (IRT) models, such as the Rasch model (53, 54), and conducting cross-group comparisons by gender and country would enhance the generalizability and cultural sensitivity of the scale. Finally, addressing self-selection bias through random or stratified sampling techniques would reduce ambiguity concerning the population represented in the study and improve the inferential validity of the findings.
Considering these limitations, we can conclude that the GAD-7 maintains a stable factorial structure across both men and women, as well as among different countries in LAC. This provides a solid empirical foundation for the use of the GAD-7 in clinical and epidemiological research within the region and across diverse contexts. Additionally, it facilitates the early detection of anxiety and supports the implementation of mental health policies that address the specific needs of the region.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statementThe studies involving humans were approved by Ethics Committee of Universidad de La Costa, record No. 173 of May 27, 2024. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributionsNL: Writing – original draft, Writing – review & editing, Data curation, Conceptualization, Methodology, Supervision, Resources, Validation. JC: Writing – review & editing, Funding acquisition, Investigation, Methodology. DR: Investigation, Software, Writing – original draft. NC: Data curation, Formal analysis, Writing – review & editing. CQ: Data curation, Methodology, Writing – review & editing. BM: Investigation, Methodology, Writing – original draft. RQ: Data curation, Investigation, Writing – original draft. CC: Funding acquisition, Project administration, Writing – review & editing. JM: Funding acquisition, Project administration, Writing – original draft. JC: Investigation, Resources, Writing – review & editing. LC: Investigation, Validation, Writing – original draft. DS: Software, Visualization, Writing – review & editing. IF: Data curation, Formal analysis, Writing – original draft. JH: Formal analysis, Resources, Writing – review & editing. WB: Formal analysis, Methodology, Writing – original draft. YF: Resources, Validation, Writing – review & editing. KA: Software, Visualization, Writing – original draft. BZ: Data curation, Formal analysis, Writing – review & editing. EM: Data curation, Formal analysis, Writing – original draft. CR: Formal analysis, Funding acquisition, Writing – review & editing. RA: Data curation, Formal analysis, Writing – original draft. CA: Project administration, Software, Writing – review & editing. PG: Data curation, Formal analysis, Writing – original draft.
FundingThe author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was approved and funded by the Universidad de la Costa. Project reference: INV. 140-03-001-18.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Organización Mundial de la Salud. Salud mental y COVID-19: datos iniciales sobre las repercusiones de la pandemia. Ginebra, Suiza: Organización Mundial de la Salud, (2022). pp. 1–13.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. In: Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed, vol. 947. American Psychiatric Association, Arlington, VA, US (2013). p. xliv, 947–xliv p. doi: 10.1176/appi.books.9780890425596
Crossref Full Text | Google Scholar
3. Fernández Sánchez A, Estrada Salvarrey MN, Jaime ERA. Relación de estrés-ansiedad y depresión laboral en profesionales de enfermería. Rev Enfermería Neurológica. (2019) 18:29–40. http://www.revenferneurolenlinea.org.mx (Accessed March 22, 2024).
4. Vahratian A J, Blumberg S, Terlizzi E P, Schiller JS. Symptoms of anxiety or depressive disorder and use of mental health care among adults during the COVID-19 pandemic — United states, symptoms of anxiety or depressive disorder and use of mental health care among adults during the COVID-19 pandemic — United. Morbidity Mortality Weekly Rep. (2021) 70:490–4. doi: 10.15585/mmwr.mm7013e2
PubMed Abstract | Crossref Full Text | Google Scholar
5. Lucas-Hernández A, González-Rodríguez VDR, López-Flores A, Kammar-García A, Mancilla-Galindo J, Vera-Lastra O, et al. Stress, anxiety, and depression in health workers during the COVID-19 pandemic. Rev Med Inst Mex Seguro Soc. (2022) 60:556–62.
PubMed Abstract | Google Scholar
7. Wiebenga JX, Eikelenboom M, Heering HD, van Oppen P, Penninx BW. Suicide ideation versus suicide attempt: Examining overlapping and differential determinants in a large cohort of patients with depression and/or anxiety. Aust N Z J Psychiatry. (2021) 55:167–79. doi: 10.1177/0004867420951256
PubMed Abstract | Crossref Full Text | Google Scholar
8. Busby-Grant J, Batterham PJ, McCallum SM, Werner-Seidler A, Calear AL. Specific anxiety and depression symptoms are risk factors for the onset of suicidal ideation and suicide attempts in youth. J Affect Disord. (2023) 327:299–305. doi: 10.1016/j.jad.2023.02.024
PubMed Abstract | Crossref Full Text | Google Scholar
9. Meuret AE, Tunnell N, Roque A. Anxiety disorders and medical comorbidity: treatment implications. Adv Exp Med Biol. (2020) 1191:237–61.
10. Capobianco L, Faija C, Husain Z, Wells A. Metacognitive beliefs and their relationship with anxiety and depression in physical illnesses: A systematic review. PLoS One. (2020) 15:e0238457. doi: 10.1371/journal.pone.0238457
PubMed Abstract | Crossref Full Text | Google Scholar
11. Groen RN, Ryan O, Wigman JTW, Riese H, Penninx BWJH, Giltay EJ, et al. Comorbidity between depression and anxiety : assessing the role of bridge mental states in dynamic psychological networks. BMC Med (2020) 18:1–17. doi: 10.1186/s12916-020-01738-z
PubMed Abstract | Crossref Full Text | Google Scholar
12. Werner-Seidler A, Spanos S, Calear AL, Perry Y, Torok M, O’Dea B, et al. School-based depression and anxiety prevention programs: An updated systematic review and meta-analysis. Clin Psychol Rev. (2021) 89:102079. doi: 10.1016/j.cpr.2021.102079
PubMed Abstract | Crossref Full Text | Google Scholar
13. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
PubMed Abstract | Crossref Full Text | Google Scholar
16. Soto-Balbuena C, Rodríguez-Muñoz MF, Le HN. Validation of the generalized anxiety disorder screener (GAD-7) in Spanish pregnant women. Psicothema. (2021) 33:164–70. doi: 10.7334/psicothema2020.167
PubMed Abstract | Crossref Full Text | Google Scholar
18. Gong Y, Zhou H, Zhang Y, Zhu X, Wang X, Shen B, et al. Validation of the 7-item Generalized Anxiety Disorder scale (GAD-7) as a screening tool for anxiety among pregnant Chinese women. J Affect Disord. (2021) 282:98–103. doi: 10.1016/j.jad.2020.12.129
PubMed Abstract | Crossref Full Text | Google Scholar
19. Pranckeviciene A, Saudargiene A, Gecaite-Stonciene J, Liaugaudaite V, Griskova-Bulanova I, Simkute D, et al. Validation of the patient health questionnaire-9 and the generalized anxiety disorder-7 in Lithuanian student sample. PLoS One. (2022) 17:e0263027. doi: 10.1371/journal.pone.0263027
PubMed Abstract | Crossref Full Text | Google Scholar
20. Byrd-Bredbenner C, Eck K, Quick V. Psychometric properties of the generalized anxiety disorder-7 and generalized anxiety disorder-mini in United States university students. Front Psychol. (2020) 11:550533/full. doi: 10.3389/fpsyg.2020.550533/full
PubMed Abstract | Crossref Full Text | Google Scholar
21. Baños-Chaparro J, Lamas-Delgado F, Ynquillay-Lima P, Jacobi-Romero DJ, Fuster-Guillen FG. Evaluación de síntomas de ansiedad: evidencias psicométricas del Generalized Anxiety Disorder-7 en adultos Peruanos. Duazary. (2022) 19:258–70. doi: 10.21676/2389783X.4986
Crossref Full Text | Google Scholar
22. Hinz A, Klein AM, Brähler E, Glaesmer H, Luck T, Riedel-Heller SG, et al. Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J Affect Disord. (2017) 210:338–44. doi: 10.1016/j.jad.2016.12.012
PubMed Abstract | Crossref Full Text | Google Scholar
25. Wickham H, Averick M, Bryan J, Chang W, McGowan L, François R, et al. Welcome to the tidyverse. J Open Source Software. (2019) 4:1686. doi: 10.21105/joss.01686
Crossref Full Text | Google Scholar
26. Revelle W. psych: Procedures for personality and psychological research. R package version 2.0. Northwestern University, Evanston, Illinois (2020).
27. Rosseel Y. lavaan : an R package for structural equation modeling. J Stat Softw. (2012) 48:1–36.
28. Epskamp S, Stuber S, Nak J, Veenman M, Lemmens M. semPlot: Path diagrams and visual analysis of various SEM packages’ output. R package version 1.1. Northwestern University, Evanston, Illinois (2019).
29. Jorgensen TD, Pornprasertmanit S, Schoemann AM, Rosseel Y. semTools: Useful tools for structural equation modeling. R package version 0.5-3. Northwestern University, Evanston, Illinois (2020).
30. Kelley K. MBESS: Methods for the Behavioral, Educational, and Social Sciences R package version 4.9.3. (2020). Available online at: https://rdrr.io/cran/MBESS/ (Accessed August 08, 2024).
32. Johnson SU, Ulvenes PG, Øktedalen T, Hoffart A. Psychometric properties of the general anxiety disorder 7-item (GAD-7) scale in a heterogeneous psychiatric sample. Front Psychol. (2019) 10. doi: 10.3389/fpsyg.2019.01713
PubMed Abstract | Crossref Full Text | Google Scholar
33. Sapra A, Bhandari P, Sharma S, Chanpura T, Lopp L. Using generalized anxiety disorder-2 (GAD-2) and GAD-7 in a primary care setting. Cureus. (2020) 12:e8224. doi: 10.7759/cureus.8224
PubMed Abstract | Crossref Full Text | Google Scholar
34. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
PubMed Abstract | Crossref Full Text | Google Scholar
36. Villarreal-Zegarra D, Paredes-Angeles R, Mayo-Puchoc N, Arenas-Minaya E, Huarcaya-Victoria J, Copez-Lonzoy A. Psychometric properties of the GAD-7 (General Anxiety Disorder-7): a cross-sectional study of the Peruvian general population. BMC Psychol. (2024) 12:183. doi: 10.1186/s40359-024-01688-8
PubMed Abstract | Crossref Full Text | Google Scholar
37. Romano I, Ferro MA, Patte KA, Leatherdale ST. Measurement invariance of the GAD-7 and CESD-R-10 among adolescents in Canada. J Pediatr Psychol. (2022) 47:585–94. doi: 10.1093/jpepsy/jsab119
PubMed Abstract | Crossref Full Text | Google Scholar
38. Niwenahisemo LC, Hong S, Kuang L. Assessing anxiety symptom severity in Rwandese adolescents: cross-gender measurement invariance of GAD-7. Front Psychiatry. (2024) 15. doi: 10.3389/fpsyt.2024.1346267
PubMed Abstract | Crossref Full Text | Google Scholar
39. Bolgeo T, Di Matteo R, Simonelli N, Dal Molin A, Lusignani M, Bassola B, et al. Psychometric properties and measurement invariance of the 7-item General Anxiety Disorder scale (GAD-7) in an Italian coronary heart disease population. J Affect Disord. (2023) 334:213–9. doi: 10.1016/j.jad.2023.04.140
PubMed Abstract | Crossref Full Text | Google Scholar
41. Caldichoury N, García-Roncallo P, Saldías C, Zurita B, Castellanos C, Herrera-Pino J, et al. Impacto psicológico del COVID-19 en los trabajadores sanitarios durante el segundo año de pandemia en Latinoamérica: estudio de encuesta transversal. Rev Colomb Psiquiatr. (2023). https://linkinghub.elsevier.com/retrieve/pii/S0034745023000355 (Accessed May 15, 2024).
42. Monteiro RP, Nascimento BS, Monteiro TMC, da Silva PDG, Ferreira AJC. Psychometric evidence of the 7-item generalized anxiety disorder questionnaire in Brazil. Int J Ment Health Addict. (2022) 20:1023–34. doi: 10.1007/s11469-020-00423-9
Crossref Full Text | Google Scholar
43. Cardoso da Silva DJ, Dias Lopes LF, Amaral L, Bortoluzzi Balconi S, Ramser CA, Pereira da Veiga C, et al. Concern over anxiety disorder among young students in Latin America. Int J Health Promot Educ. (2022) 62(6):608–63. doi: 10.1080/14635240.2022.2086897
Crossref Full Text | Google Scholar
45. Sequeira SL, Morrow KE, Silk JS, Kolko DJ, Pilkonis PA, Lindhiem O. National norms and correlates of the PHQ-8 and GAD-7 in parents of school-age children. J Child Fam Stud. (2021) 30:2303–14. doi: 10.1007/s10826-021-02026-x
PubMed Abstract | Crossref Full Text | Google Scholar
46. Petit-Breuilh Padilla S. Evaluación de las propiedades psicométricas de la escala de ansiedad GAD-7 en gestantes y madres residentes en Chile de hijos e hijas menores de 6 meses entre los años 2020-2021. Concepción, Chile: Universidad de Concepción (2022). Available at: http://repositorio.udec.cl/jspui/handle/11594/9946 (Accessed August 08, 2024).
47. Nyongesa MK, Mwangi P, Koot HM, Cuijpers P, Newton CRJC, Abubakar A. The reliability, validity and factorial structure of the Swahili version of the 7-item generalized anxiety disorder scale (GAD-7) among adults living with HIV from Kilifi, Kenya. Ann Gen Psychiatry. (2020) 19:62. doi: 10.1186/s12991-020-00312-4
PubMed Abstract | Crossref Full Text | Google Scholar
48. De Man J, Absetz P, Sathish T, Desloge A, Haregu T, Oldenburg B, et al. Are the PHQ-9 and GAD-7 suitable for use in India? A psychometric analysis. Front Psychol. (2021) 12. doi: 10
留言 (0)