PPC is a rare diagnosis in medicine, and even more rarely described in forensic medicine, probably due to the low proportion of traumatic origins in the etiologies described [1,2,3,4, 6, 7]. It can be complicated by cardiac tamponade when PPC is under high pressure “tension PPC”, and is called “low-pressure cardiac tamponade” when hemorrhagic shock develops concurently with lower gaz accumultation (the volume of gas in the pericardial cavity is not as substantial as in high-pressure pneumopericardium however, even this smaller volume of gas can contribute to cardiac tamponade, especially when combined with hemorrhagic shock, leading to lower pressure in cardiac cavity) [6, 8].
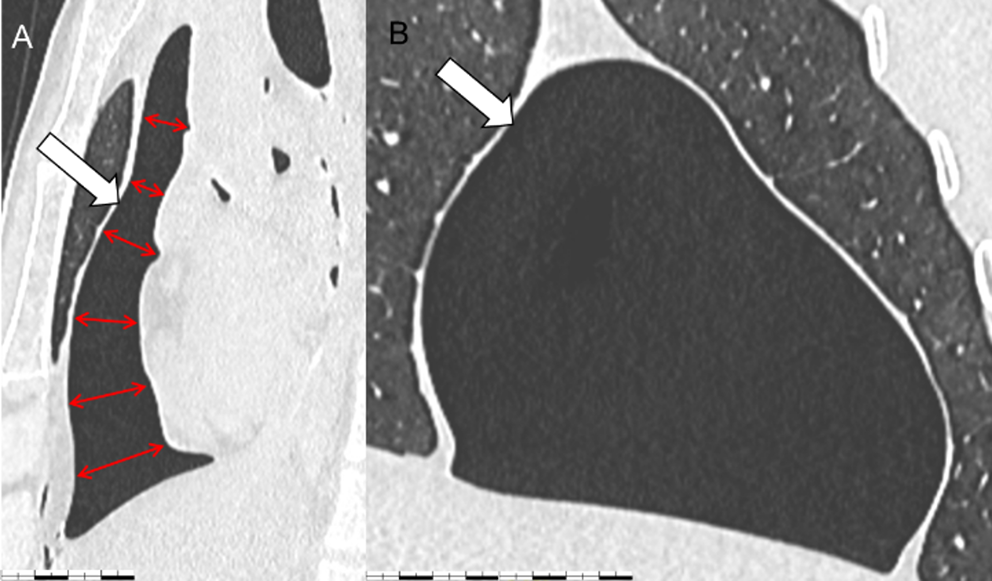
In their case of PPC with tamponade, Heimer et al. showed radiological abnormalities in favour of the compressive nature of the pneumopericardium: the CT scan revealed the so-called “small heart” sign due to compression of the right ventricle, and the pericardium appeared bulging into the right pleural cavity [3]. “Small heart” sign was first described by Mirvis et al. in 1986 during PPC with a decrease in the cardiothoracic index [9]. In 1996, Hernandez-Luyando et al. first described the “flattened heart” sign in PPC, with flattening of the anterior surface of the heart and reduction in its anteroposterior diameter [10].
Diagnosis of PPC is difficult to establish at autopsy, as the air contained in the pericardial sac escapes when it is opened [3, 6]. However, a post-mortem CT scan can reveal it without difficulty, and can provide arguments in favor of tamponade [7, 9,10,11].
Apart from advanced putrefaction, post-mortem gas production in the pericardial sac is not typical. In our case, there was no evidence of putrefaction, with an RA-Index of 0 [12]. Moreover, given the absence of any reported resuscitation maneuvers and the limited handling of the body after its discovery, iatrogenic origin can be ruled out.
Ro et al. recently reported a case of suicide by stabbing, with two wounds in the epigastric region. The authors argued in favor of a mixed cause of death, secondary to hypovolemia linked to blood depletion following the aortic wound, and to a compressive pneumopericardium (measured at 133 ml) [6]. The publication of this article was the subject of an exchange with Zivkovic et al. on the question of whether the pneumopericardium was responsible for the death [13]. Ro et al. argued in favor of this imputability by the fact that thoracic movements, associated with the existence of a check valve function with the liver and diaphragm, would allow the formation of a pneumopericardium. In addition, they pointed out that signs of tamponade such as jugular vein turgor were often absent [14].
Indeed, for a pneumopericardium to become compressive, air must accumulate within the pericardial sac with a one-way valve effect through the wound [1, 3, 15]. During inspiration, the descent of the diaphragm lowers intrathoracic pressure, allowing air to enter the pericardium. During expiration, the upward movement of the diaphragm and liver may compress the wound, reducing or preventing the escape of air [6]. Over successive respiratory cycles, this mechanism could result in a gradual increase in intrapericardial pressure. The resulting pericardial distension may further contribute to this valve effect by mechanically sealing the wound margins. Given the similar anatomical location between our case and previous reports, anatomical factors, such as the proximity of the wound to the diaphragm and interaction with the liver, appear to play a role in creating the valve effect.
Other authors have described cases of compressive pneumopericardium, lethal or not, in association with a stab wound, but this entity remains rare in forensic practice, and the origin of death is sometimes subject to controversy [3, 13,14,15,16,17,18,19,20].
The autopsy case we report is, to our knowledge, the first french publication on the subject. Unlike some of the cases described previously, in our case there is little doubt as to the cause of death. Indeed, there was no hemorrhage likely to explain the death [13].
Although the volume of gas accumulated in the pericardial sac may appear significant for suggesting a diagnosis of compressive pneumopericardium (CPP), we believe that the CT scan features such as ‘small heart’ and ‘flattened heart’ are more relevant, as they directly reflect the pressure exerted by the pneumopericardium on the heart. Conversely, the gas volume may vary depending on the individual’s morphology and anatomical particularities, making it a less reliable indicator of clinical impact. In our case, the presence of signs of congestion and a compressed pneumopericardium (flattened heart on PMCT) strongly suggests that the elevated intrapericardial pressure caused significant cardiac compression. This likely impaired diastolic filling, particularly of the right ventricle, reducing cardiac output and leading to acute heart failure. The resulting increase in hydrostatic pressure within the pulmonary vessels explains the observed pulmonary congestion and edema, supporting cardiogenic shock as the probable cause of death. Additionally, the small wound and hemorrhagic infiltration on the heart’s surface could have directly irritated the myocardium, potentially triggering a rhythm or conduction disorder that contributed to the fatal outcome.
Keypoints:
Post-mortem computed tomography is crucial for diagnosing and characterizing PPC, particularly in visualizing its compressive effects, such as a'flattened' or'small' heart, which aid in determining the mechanism of death.
While essential for diagnosing PPC, post-mortem imaging remains a complementary tool. Autopsy remains indispensable for accurately determining the cause of death through comprehensive macroscopic findings and further investigations.









留言 (0)