
記住我
Spinal tuberculosis (TB), or Pott's disease, remains a substantial worldwide health concern, especially in areas with elevated TB prevalence, including several developing countries. Globally, TB affects more than 10 million individuals, and annually, around 150,000 new cases of spinal TB are reported (1). India, China, Nigeria, Pakistan, Indonesia, and South Africa comprise 64 percent of all documented cases (2). The incidence rate of TB increased by 3.6% in 2021 compared to 2020 (3). Subsequently, the burden of drug-resistant TB rose by 3% from 2020 to 2021, with 450,000 recorded cases of rifampicin-resistant TB in 2021. Russia and other nations in Eastern Europe and Central Asia documented the most significant percentages (>50%) of multidrug-resistant or rifampicin-resistant TB among persons previously treated (3). In addition, spinal TB represents <1% of all TB cases (4, 5). This disease can also lead to debilitating consequences, including severe deformities, neurological deficits, and even paraplegia if not managed appropriately (6). While antitubercular drug therapy is the cornerstone of treatment, its limitations become evident in advanced cases, particularly when there is deformity, spinal instability or neurological complications (7, 8). The incidence of neurological complications varies between 10% and 43% (4). Medical therapy alone may be insufficient in such scenarios, necessitating surgical intervention (9, 10).
Surgical management, particularly within the orthopaedic and neurosurgery disciplines, plays a crucial role in managing spinal TB, especially when conservative treatment fails (10). Although the roles of each discipline can overlap, surgery is often required to stabilize the spine, decompress neural elements, prevent or correct deformities, alleviate pain, and improve neurological outcomes (11–14). Over the years, advancements in surgical techniques have been reported to be significantly beneficial for patients with spinal TB. Several meta-analyses have been conducted to compare each approach. However, the results are varied because of several factors, including the location of the disease, the patient's comorbidities, the extent of spinal involvement, and others. Additionally, approach consideration is also essential; some studies favour the posterior approach (15–17), some anterior approach (18), and some both the posterior-only approach and combined posterior-anterior approach (19). In addition, recently, several minimal invasive approaches have also been reported, for instance, using video-assisted thoracic surgery (VATS) (20–24), minimally invasive pedicle screw fixation (25–27), and minimally invasive far lateral debridement combined with posterior instrumentation (MI-FLDPI) (28).
Bibliometric analysis, which quantitatively studies scientific publications, offers valuable insights into research trends, key contributors, and emerging areas of interest (29–31). Bibliometric analysis has been performed in the scope of medicine and health, which may provide valuable insights into research trends, key contributors, and emerging areas, aiding in the evolution of medical practices and guiding future research and policy decisions (32, 33). By examining the global research landscape, bibliometric studies can elucidate the evolution of surgical management to spinal TB, guiding future research and informing policy decisions. Therefore, this study aims to perform a comprehensive bibliometric and scientific mapping analysis of worldwide publications on surgical interventions in managing spinal TB. A comparison of the contributions of orthopaedics and neurosurgery in this field is also performed.
2 Methods 2.1 Data sources and search strategyA comprehensive bibliometric analysis was conducted for scientific mapping following procedures from previous studies (34–42). The data was obtained from the Scopus database online. Before selecting Scopus as the primary database, it was compared with other databases, including PubMed and ScienceDirect, to evaluate coverage and relevance. Then, Scopus was chosen because it provides the most comprehensive metadata compatible with Biblioshiny software and includes more relevant publications on spinal TB than other databases. Subsequently, to mitigate the bias introduced by daily database changes, the search process was executed on Saturday, August 31, 2024. Keywords utilized in this study were (“spinal tuberculosis” OR “spinal TB” OR “tuberculous spondylitis” OR “pott's disease” OR “pott disease”) AND (surger* OR surgeo* OR surgical OR operative). The preliminary search identified 2,886 studies. Only literature published in English that had attained the final publication stage was included. Subsequently, the document types included are articles, reviews, conference papers, and book chapters. Then, all the studies that met our requirements based on the title and abstract were screened, and any irrelevant studies were eliminated. Finally, 1,857 studies were included in this study. Additionally, to compare orthopaedics and neurosurgery publications on this topic, the keywords (“spinal tuberculosis” OR “spinal TB” OR “tuberculous spondylitis” OR “pott's disease” OR “pott disease”) AND (orthopedi* OR orthopaedi*) were used for orthopaedics publication searching. After screening, we revealed a total of 274 publications included. Subsequently, (“spinal tuberculosis” OR “spinal TB” OR “tuberculous spondylitis” OR “pott's disease” OR “pott disease”) AND (neurosurge*) were used for neurosurgery publication searching, and a total of 96 publications were included after the screening process.
2.2 Data analysisThe publication output was analyzed using Scopus analysis tools, R package's bibliometrics (Biblioshiny) (43–45), and VOSviewer (version 1.6.18) (46, 47). Scopus analysis tools were used to obtain the top ten most relevant authors, affiliations, countries, funding sponsors, and the most influential publications. The R package's bibliometrics (Biblioshiny) utility was designed for quantitative scientometrics and informetrics. This study used Biblioshiny to describe included studies, annual scientific production, its impacts, and trend topics. In trend topics, the visualization was set for four topics per year. Subsequently, a bibliometric network of keywords co-occurrence for prominent or key topics was analyzed using VOSviewer. In this study, the visualization of prominent or key topics was set on a minimum occurrence of seven and a minimum total link of the strength of 5 using VOSviewer. Inconsistent or evolving terminology over time was addressed by standardizing keywords, replacing synonymous terms, unifying terminology with different spellings, and grouping keywords with similar meanings.
3 Results 3.1 Description of included studiesThis study included 1,857 publications published from 1896 to 2024, sourced from 621 different journals, books, and other academic publications. The average annual growth rate of publications is 3.24%. Each document has an average of 17.67 citations, and there are 33,354 references cited across all documents. The dataset includes 6,659 Keywords Plus terms and 2,441 author-defined keywords. Subsequently, there are 5,699 authors, with 159 single-authored documents and an average of 4.7 co-authors per document. International co-authorship accounts for 5.708% of the total. Last, document types are predominantly research articles (1,599), with additional contributions from 42 book chapters, 48 conference papers, and 168 review articles.
3.2 Annual scientific production and impactsOver the years, the number of published articles in the field has fluctuated significantly. Early periods such as 1896 and 1920 saw only a single article each year with very few citations, reflecting limited research output. However, the volume of publications increased substantially from the mid-20th century onwards, peaking in 2022 with 148 articles. Despite this increase in the number of articles, the mean total citations per article has shown considerable variation. In some years, such as 2006, the average number of citations per article was notably high at 31.68, indicating a period of significant impact and recognition. Conversely, in recent years like 2022, the average number of citations per article decreased to 1.87, suggesting a shift in citation patterns and possibly an increase in the number of articles with fewer citations or due to their recent publication, which means they have had less time to accumulate citations compared to older articles.
The mean total citations per year reflects the average number of citations received by articles published in a specific year. This metric has exhibited notable peaks, such as in 1990, when articles had an average of 56.11 citations per year, indicating strong citation impact. Similar to previous metrics, this figure has declined recently, with 2022 showing an average of only 1.87 citations per year. Subsequently, citable years measures how long articles have been available for citation and provides context for understanding citation longevity. Older articles from the early 20th century have had more time to accumulate citations, while more recent articles have had less time to be cited. This metric highlights articles’ ongoing relevance and potential impact over time, influencing the interpretation of citation data and research trends. All of the details of annual scientific production and its impacts are visualized in Figure 1.
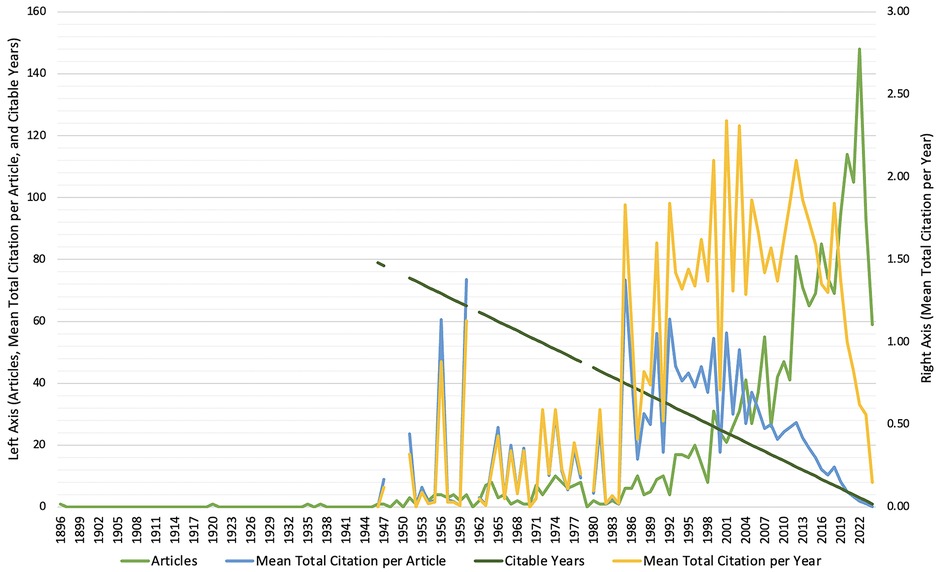
Figure 1. Annual scientific production and impacts on the role of surgery on spinal tuberculosis.
3.3 Most relevant authors, affiliations, countries, and funding sponsorsMost relevant authors, affiliations, countries, and funding sponsors on surgical management for spinal TB are visualized in Figure 2. Wang, X. (34 publications), Jain, A.K. (23 publications), and Zeng, H. (21 publications) as the most prolific authors in the field. Subsequently, the leading affiliations include Xiangya Hospital Central South University (78 publications) and Central South University and Army Medical University, each with 33 publications. In addition, China emerged as the most prominent country, accounting for 509 publications, followed by India with 325 and the United States with 195. Last, the National Natural Science Foundation of China (94 publications) was the top funding sponsor, followed by the Ministry of Science and Technology of the People's Republic of China (13 publications) and Xiangya Hospital, Central South University (10 publications).
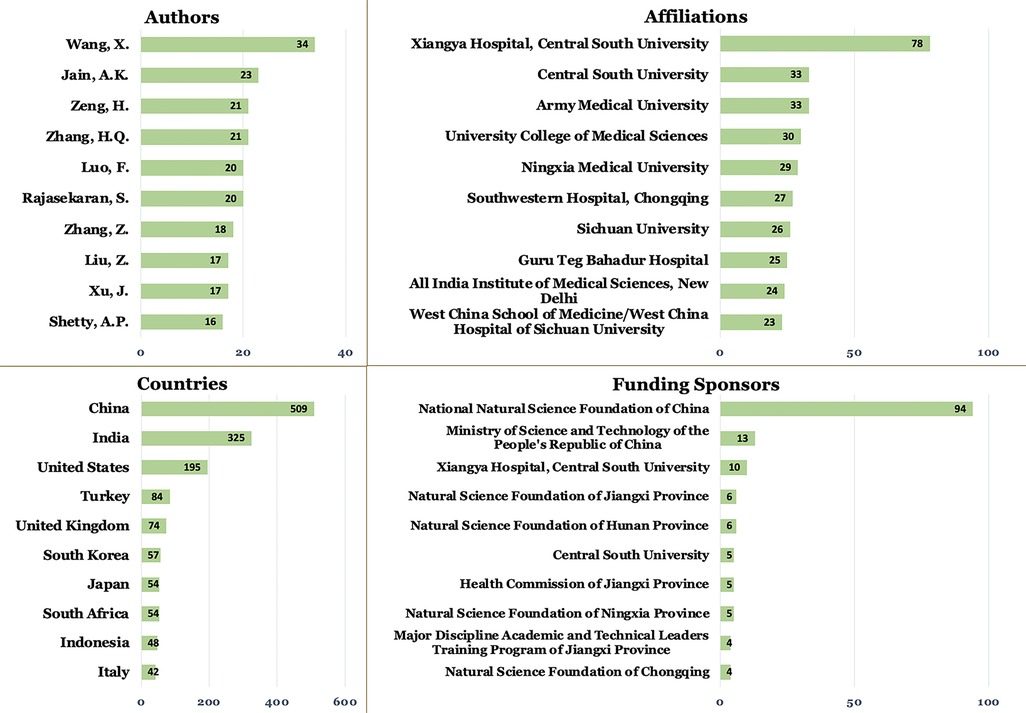
Figure 2. Most relevant authors, affiliations, countries, and funding sponsors on the role of surgery on spinal tuberculosis.
3.4 Most influential publicationsAmong the entire publications in the field of surgery roles on spinal TB, the article “Spinal tuberculosis: A review,” published in the Journal of Spinal Cord Medicine in 2011, stands out with a total of 460 citations and an average of 35.38 citations per year. Another key publication is “Tuberculosis of the spine: A fresh look at an old disease,” which appeared in the Journal of Bone and Joint Surgery in 2010, with 325 citations and an average of 23.21 citations per year. The article “Anterior spinal fusion. The operative approach and pathological findings in 412 patients with Pott's disease of the spine,” published in The British Journal of Surgery, published in 1960, is also highly influential. It has garnered 292 citations, averaging 4.56 citations per year. The ten most influential publications on the role of surgery on spinal TB are displayed in Table 1.
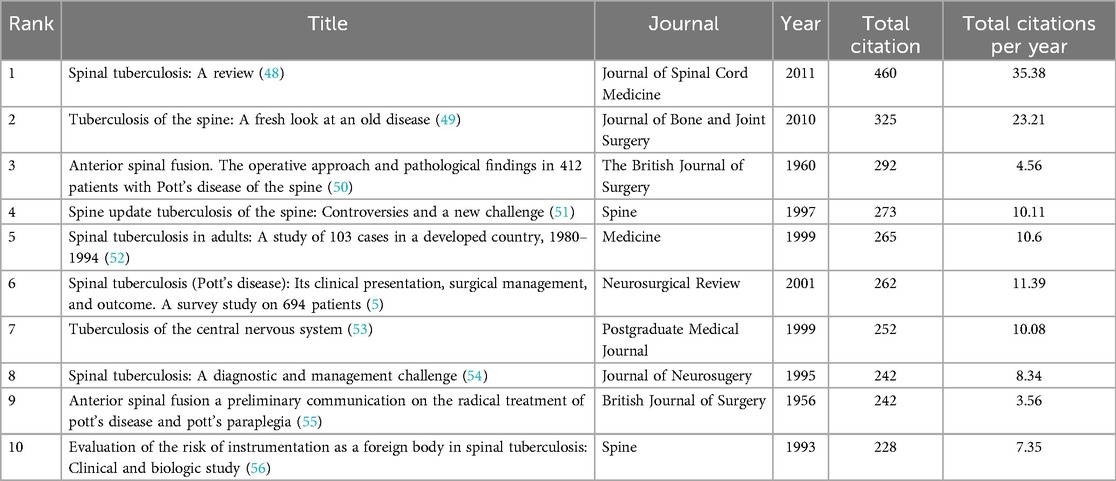
Table 1. Most influential publications on the role of surgery on spinal tuberculosis.
3.5 Trend topicsThis scientific mapping finds that the evolution of spinal surgery management for treating spinal TB publications has progressed from a basic foundation in early surgical methods, the integration of pharmacological approaches alongside surgical techniques, advancing into imaging research, procedure studies with refined surgical methods, and most recently, a technology-driven phase incorporating innovations like artificial intelligence and machine learning. The basic foundation was laid in the 1950s and 1960s when the focus was on early surgical methods, which was evident from terms like “tuberculosis, spinal/therapy” and “surgical procedures, operative.” Subsequently, as the field progressed, there was a significant integration of pharmacological approaches alongside surgical techniques. Terms like “aminosalicylic acid,” “isoniazid,” “rifampin,” “ethambutol,” and “pyrazinamide,” and “drug therapy” highlight the emergence of combining medications with surgery to improve patient outcomes.
The subsequent period marked a shift toward imaging research and procedure research, with increased attention on diagnostic tools like “magnetic resonance imaging (MRI)” and “myelography.” In addition, advancements in “surgical instrumentation” and the development of complex procedures, including “spine fusion,” reflected the ongoing refinement of surgical methods. The field has entered a technology-driven phase in recent years, incorporating cutting-edge tools like “artificial intelligence” and “machine learning.” This latest trend indicates a move towards highly specialized, technology-enhanced approaches in managing spinal TB, reflecting the continuous evolution of the field. The entire trend topics on the role of surgery on spinal TB are visualized in Figure 3.
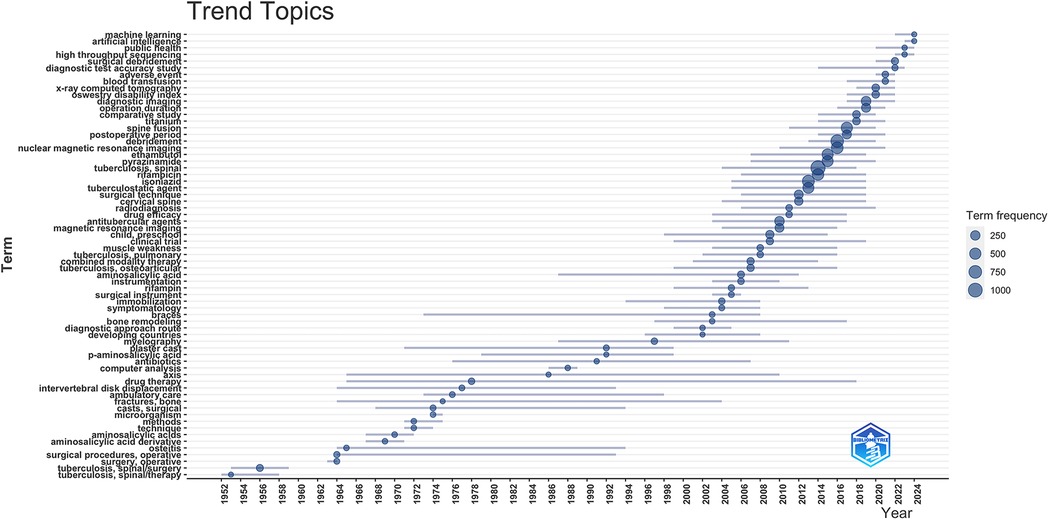
Figure 3. Trend topics on the role of surgery on spinal tuberculosis.
3.6 Prominent/key and underdeveloped topicsIn the context of surgery for spinal TB, there are more common keywords, for instance posterior approach (with occurrence of 38), minimally invasive spine surgery (30), bone graft (27), anterior approach (25), instrumentation (25), posterior approach only (24), spinal fusion surgery (24), titanium mesh cages (24), chemotherapy (20), anti-tuberculosis treatment (14), combined anterior and posterior approach (14), posterior instrumentation (14), meta-analysis (12), anterior debridement (10), anterior decompression (10), and anterior instrumentation (8). These more common keywords, which represent prominent/key topics on the role of surgery on spinal TB, are visualized in Figure 4. We set only keywords with a minimum occurrence of 7 that are visualized in that Figure, and the line between keywords was set on the minimum of 5 strength.
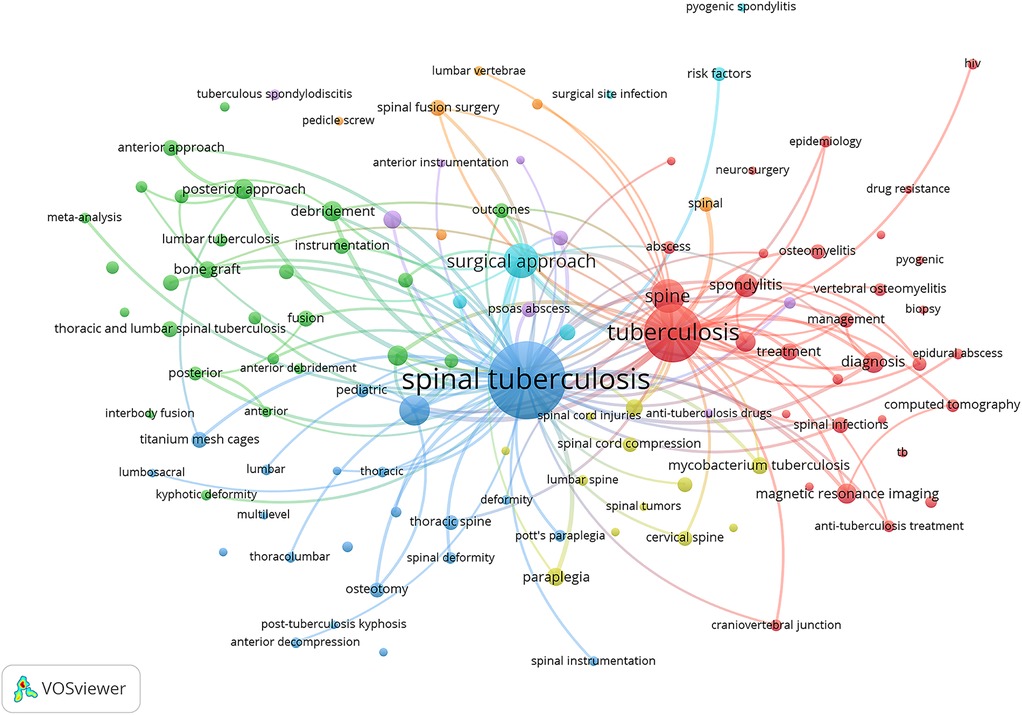
Figure 4. Prominent/key topics on the role of surgery on spinal tuberculosis.
Subsequently, less common keywords, which may suggest emerging or underexplored areas, include arthrodesis (3), machine learning (3), short-segment fixation (3), video-assisted thoracoscopic surgery (3), artificial intelligence (2), biportal endoscopic spine surgery (2), circumferential decompression (2), circumferential fusion (2), closing-opening wedge (2), intraoperative neurophysiological monitoring (2), lateral extracavitary approach (2), oswestry disability index (2), pedicle screw fixation (2), pedicle screw instrumentation (2), pedicle subtraction osteotomy (2), polymethylmethacrylate (2), posterior transforaminal lumbar debridement (2), posterolateral approaches (2), posterolateral decompression (2), retroperitoneal approach (2), revision surgery (2), single-segment fixation (2), thoracolumbar corpectomy (2), transforaminal lumbar interbody fusion (TLIF) (2), transoral surgery (2), transpedicular approach (2), transpedicular corpectomy (2), transpedicular instrumentation (2), two-stage surgery (2), unilateral limited laminectomy (2), and video-assisted thoracic surgery (2).
3.7 Comparison of orthopedics surgery and neurosurgery publicationsIn comparing the metrics between orthopaedic surgery and neurosurgery in the context of spinal TB, orthopaedic surgery stands out with a higher total number of publications, totalling 274, compared to 96 in neurosurgery. The leading author in orthopaedic surgery is Wang, X. with ten publications, while Kumar, R. is the most prominent in neurosurgery with three publications. Xiangya Hospital Central South University leads in orthopaedic surgery affiliations with 14 publications, whereas Sanjay Gandhi Postgraduate Institute of Medical Sciences tops neurosurgery with four publications. China is the top country contributing to orthopaedic surgery, with 85 publications, while the United States leads neurosurgery with 20 publications. The National Natural Science Foundation of China is the top funding sponsor for orthopaedic surgery, supporting 18 publications. In neurosurgery, the Education Department of Jiangxi Province and others support two publications. Last, the Spine journal is the leading publication outlet for orthopaedic surgery with 18 articles, whereas World Neurosurgery is the top journal in neurosurgery with 13 articles. Entire comparison metrics can be seen in Table 2.
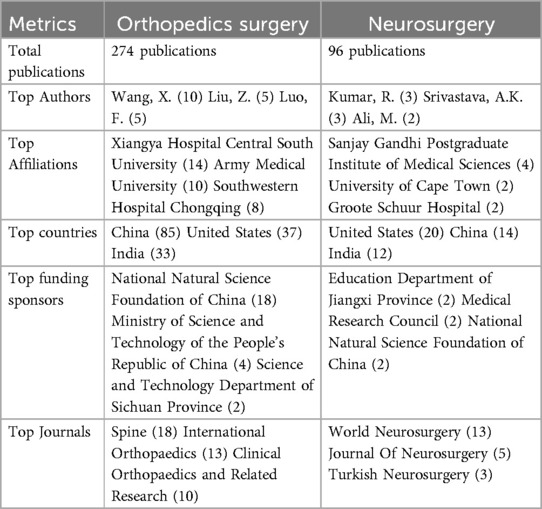
Table 2. Comparison of orthopedics surgery and neurosurgery publications on the role of surgery on spinal tuberculosis.
4 Discussion 4.1 Overview of findingsThis study provides a comprehensive bibliometric analysis of the global research landscape concerning the surgical management of spinal TB, spanning publications from 1896 to 2024. The analysis revealed a steady increase in scholarly output, with a significant surge in the number of publications in recent decades. This growth reflects the increasing recognition of spinal TB as a critical health issue and the evolving role of surgery in its management. Orthopaedic surgery has contributed more to this field than neurosurgery, as evidenced by more publications.
Orthopaedic surgery often focuses on structural stability, deformity correction, and spinal reconstruction, which are critical in addressing the primary manifestations of spinal TB. Conversely, neurosurgery's contributions, though fewer in volume, remain indispensable, particularly in refining surgical strategies to address neurological deficits and optimize outcomes for cases with severe spinal cord involvement. This distinction highlights the complementary expertise of the two specialities and reinforces the importance of multidisciplinary collaboration between orthopaedic surgeons and neurosurgeons. This comparison also holds important global health implications. Spinal TB is a significant burden in low-resource settings, and understanding the dominant and non-dominant contributors can help policymakers and researchers allocate efforts to bridge gaps. These efforts might include increasing neurosurgical training or resources, especially in underserved regions.
China has emerged as a dominant contributor to research in this field, with leading authors, institutions, and funding agencies driving much of the scholarly work. In the entire work, the role of surgery in spinal TB publications from China has gained 5,595 citations and 35 h-index. The reasons behind China's high publication output are possibly due to a multifaceted phenomenon driven by several interconnected factors. First, China faces a significant TB burden. The World Health Organization indicates that China is the second highest among the 22 countries with the most significant TB burden (57), possibly making TB a critical priority. Subsequently, China's centralized healthcare system facilitates large-scale data collection and analysis, and the implementation of integrated TB control models in primary healthcare sectors has enabled comprehensive studies on TB control effectiveness (58, 59). In addition, recent reforms in China's research funding landscape have aimed to improve efficiency and support promising scholars. For instance, the NSFC has implemented measures to curtail personal favours in the review process, reform scoring mechanisms for distinguished young scholars, and initiate funding programs for outstanding doctoral and undergraduate students (60). These policy changes may create a more competitive and productive research environment, potentially contributing to increased publication output.
Additionally, China has been actively fostering international collaborations in medical research. The analysis of collaborative networks between institutions and countries reveals a global “North-South” connection between developed and developing nations (61, 62). These partnerships may not only enhance the quality of research but also increase the likelihood of publications in high-impact international journals. Lastly, applying big data resources in medical research has significantly boosted China's research capabilities. Integrating big data in medical collaborative networks has improved the transaction efficiency of medical services, enabling more sophisticated and comprehensive studies. It has likely contributed to the quantity and quality of publications (63).
Subsequently, the evolution of key topics over time highlights the progression of surgical techniques and the integration of multidisciplinary approaches. Initially, research focused on the basic foundation of surgical methods, such as early spinal procedures and the use of antitubercular drugs. The first publication in this scope in the Scopus database was a case report entitled “Pott's disease. Its surgical treatment, with a report of a case” authored by Punton, J. and published in the Journal of Nervous and Mental Disease in 1896 (64). Over time, the focus shifted toward more advanced procedures, incorporating imaging research and refined surgical techniques like spinal fusion. In recent years, the field has moved towards technology-driven approaches, emphasizing minimally invasive techniques, the incorporation of artificial intelligence, and machine learning to improve surgical outcomes and patient care.
These findings are relatively the same as those of a previous study that describes the timeframe for spine surgery for TB over the last seven decades, which has progressed through the pre-chemotherapy, biological, mechanical, and technological phases (65). Mandar et al. described that most studies discussed debridement and extirpation of the diseased tissue approach in the pre-chemotherapeutic era. Subsequently, the biological era focused on anterior debridement and non-instrumented fusion approaches. In addition, debridement with instrumented (anterior/posterior) fusion has been discussed in the mechanical era. Last, the recent technological era describes minimally invasive techniques, thoracoscopic techniques, local drug delivery systems, and bioactive materials (65).
4.2 Main topicsIn this study, the posterior approach emerged as the most frequently discussed surgical technique in treating spinal TB, with 38 occurrences. Closely related is the “posterior approach only” method, which was mentioned 24 times. In comparison, the anterior approach was only mentioned 25 times, and the combined anterior and posterior approach was cited 14 times. More studies on posterior approaches were possible because of the higher prevalence of thoracolumbar spinal TB cases that recommended using the posterior approach.
Several high-level evidence studies, including systematic reviews and meta-analyses, have been discussed about these approaches and their combination. Liu et al. study stated that the posterior approach demonstrated equivalent clinical efficacy while reducing operation time, blood loss, hospital stay, and complications compared to the combined posterior and anterior approach in managing spinal TB (15). Subsequently, another meta-analysis by Muheremu et al. showed that the correction of the Cobb angle by the posterior approach is considerably greater than that achieved through the anterior approach (16). Another study, including comparing anterior, posterior, and combined approaches, concluded that the posterior technique yields superior clinical outcomes compared to the anterior or combination approaches for spinal TB (17). Another study showed a different result, as the anterior approach has been reported to present fewer complications than both the combined and posterior-only approaches (18). Last, a different study showed that both approaches can yield excellent clinical results. The posterior-only approach can reliably and efficiently accomplish lesion debridement, decompression, and the reconstruction and maintenance of stability, offering benefits including reduced invasiveness, diminished bleeding, shorter operative duration and hospital stay, and fewer complications, appearing to surpass the combined posterior-anterior approach (19).
In general, the choice of surgical approach could depend on several factors, including lesion location, extent of bone destruction, deformity correction needs, patient's condition, or surgeon's expertise. The location of the lesion is essential; for instance, cervicothoracic spinal TB may require either a single-stage anterior approach or a combined anterior-posterior approach, depending on the relation between the TB lesion segments and the suprasternal notch (67). Severe destruction of the anterior column may need an anterior or combined approach (68). Subsequently, the posterior-only and combined anterior-posterior approaches have shown higher correction rates for kyphotic deformity than the anterior-only approach (68). In addition, the patient's overall health also matters, as the posterior approach involves shorter surgery and less blood loss, making it a potentially better option for those in poor condition (68, 69). Last, the surgeon's experience with different techniques also plays a significant role in deciding the approach.
The analysis also highlighted the growing focus on advanced surgical techniques, particularly minimally invasive spine surgery (30 occurrences). This approach has gained traction due to its potential for reduced recovery time, decreased postoperative complications, and improved patient outcomes. Alongside these techniques, instrumentation, which was mentioned 25 times and titanium mesh cages (24 occurrences) underscores the advancements in surgical tools that have enhanced the effectiveness of spinal fusion surgeries. Subsequently, bone grafting, mentioned 27 times, remains a cornerstone technique in spinal TB surgery, particularly in reconstructing spinal stability following debridement. These supportive techniques are essential for addressing the structural damage caused by spinal TB, preventing further deformities, and enhancing the patient's quality of life post-surgery.
Additionally, the initial two decades of the 21st century (2001–2020), termed the technological era, featured the advent of diverse treatments, including less invasive techniques for treating spinal TB (70–75). Subsequently, instrumentation has shown that it plays a crucial role in managing spinal TB by providing mechanical stability and enhancing the healing process (65, 76). Various surgical techniques involving instrumentation include, for instance, posterior decompression and fusion with bone autografts, anterior debridement/decompression and fusion with bone autografts, and posterior fusion with instrumentation followed by simultaneous or sequential anterior debridement/decompression and fusion (9). In addition, previous meta-analyses (77, 78), which include several studies (79–89), have been studied about titanium mesh cages and bone grafting. Those studies concluded that both bone grafting and titanium mesh grafting are both effective and safe surgical procedures, with no significant statistical differences in outcomes.
Alongside surgical interventions, the use of chemotherapy (20 occurrences) or anti-tuberculosis treatment (14 occurrences) continues to be a critical component of managing spinal TB. A previous study has discussed the beneficial effect of chemotherapy for spinal TB, especially in mild spinal TB (90), as well as there is no indication for surgery (6). Subsequently, previous meta-analyses (91, 92), which included several studies (93–100), have been discussed to compare the duration of chemotherapy and its effect. Those studies show that short-course chemotherapy (≤6 months) is as effective as standard chemotherapy (≥nine months) in treating spinal TB. Last, emerging techniques such as anterior debridement (10 occurrences), anterior decompression (10 occurrences), and anterior instrumentation (8 occurrences) indicate a growing interest in refining and expanding the surgical toolkit available to clinicians (65).
4.3 Research gaps and future directionsThis study showed several studies need to be conducted in the future. First, even minimally invasive approaches have been studied and included in the main topics; there are no systematic reviews and meta-analyses in this scope. Future research should prioritize such studies to provide high-quality evidence on the comparative benefits of these techniques. Subsequently, areas including the utilization of artificial intelligence, machine learning, and robotics have also emerged recently and potentially can be future directions of studies. A previous study stated that recently, modern spine surgery is a multi-disciplinary endeavour involving not only the surgeon but also possibly artificial intelligence and robotic technologies (65). A study showed that using Artificial Intelligence in the form of computer navigation-assisted minimally invasive direct lateral interbody fusion may substantially decrease intraoperative radiation exposure without extending overall operation duration (101). Subsequently, machine learning could facilitate the prediction of extended hospital stays post-surgery and discover risk factors for tuberculous spondylitis patients with imbalanced data, employing a unique approach utilizing explainable artificial intelligence (XAI). That study employs an XGBoost model, readily accessible via the deployed web application, which can facilitate clinical research (102). Another study employing MVITV2, EfficientNet-B3, ResNet101, and ResNet34 as backbone networks and developing deep learning models demonstrated that sagittal images based on T2WI can effectively differentiate between spinal TB and spinal metastases (SM), achieving diagnostic performance comparable to that of experienced spine surgeons (103). Last, there is a study on developing and validating an innovative predictive model and web-based calculator assessing transfusion risk following spinal fusion for spinal TB (104).
Regarding the role of robotics technology, which has also emerged recently, The awarded Surgical Team of the Year was represented by Ravinder Uberoi from Apollo Hospitals in New Delhi. The researchers successfully performed robotic spinal surgery on a ten-year-old kid suffering from bone destruction due to spinal TB, which they characterised as a “world's first” (105). Subsequently, a study about treating thoracolumbar TB using robot-assisted and minimally invasive techniques through a transforaminal expansion method compared with traditional posterior open surgery, robot-assisted minimally invasive access through the transforaminal approach for lesion removal and bone grafting internal fixation in thoracolumbar TB treatment can decrease the operative duration and intraoperative haemorrhage, lessen surgical trauma, and achieve definitive effectiveness (106). Additionally, a study about the accuracy and safety of pedicle screw placement assisted by orthopaedic robot and C-arm fluoroscopy, including 1 case of spinal TB, showed orthopaedic robot-assisted pedicle screw placement offers advantages such as reduced fluoroscopy duration, decreased screw placement time, and enhanced precision, hence augmenting surgical safety and presenting significant potential for application in orthopaedics (107).
Thoracic pedicle screw insertion assisted by the TiRobot system for spinal TB also demonstrates favourable outcomes and holds potential for further analysis (108). In this case, they present the use of robot-assisted navigation in a complex post-tubercular pediatric kyphotic deformity. Subsequently, robotic technology coupled with navigation and integrated intraoperative CT scans could also allow precise instrumentation, reduced complications, lower radiation exposure, and better patient outcomes, especially in complex deformity cases (109). Last, there is a meta-analysis that included 7,379 pedicle screws showed that robotic-assisted surgery demonstrated significantly higher perfect pedicle screw accuracy compared to the freehand technique and also lower complication rates, proximal-facet joint violation, radiation exposure, although not specific to the spinal TB cases (110). Future studies should focus on refining these technologies, exploring their cost-effectiveness, and assessing their scalability, particularly in resource-limited settings where the burden of TB is highest.
Collectively, these advancements enhance the safety, efficiency, and effectiveness of spinal TB surgeries, marking a significant step forward in managing this challenging condition. However, the adoption of these advanced technologies may face several challenges. First, high costs may limit accessibility, particularly in low-resource settings where TB is most prevalent. Secondly, specialized training is required for surgeons and staff to use these tools effectively. Moreover, integrating artificial intelligence and robotics into already overburdened healthcare systems may pose logistical challenges. Last, ethical and legal concerns, such as patient data privacy and liability in artificial intelligence-driven decision-making, may further complicate widespread adoption. Addressing these issues is essential for maximizing the clinical potential of these technologies in spinal TB management. Therefore, future research should also focus on improving access to advanced surgical technologies and specialized care in low-resource settings. This could help address global inequalities in spinal TB management by developing scalable, cost-effective solutions that bridge the gap between high-income and low-resource healthcare systems.
An additional avenue for future research could also involve integrating advanced techniques and materials for managing spinal TB inspired by innovations in related or other fields. For instance, the Neuroendoscopic Parafascicular Evacuation of Spontaneous Intracerebral Hemorrhage (NESICH) technique, which has demonstrated utility in minimizing brain tissue damage and providing effective access for evacuating hematomas (111), may serve as an example model for minimally invasive approaches in spinal infections that may potentially reduce collateral tissue damage during surgical interventions. Similarly, image-guided techniques, such as those employed in corticospinal tract approaches for hematoma evacuation, have been shown to enhance surgical precision and reduce complications in managing delicate neural structures (112). These methods could also be adapted for guiding surgical approaches around the spinal cord in spinal TB, where precision is critical for preserving neurological function. Moreover, integrating regenerative approaches, such as the use of apoptotic bodies derived from 3D-cultured adipose stem cells, which have shown promise in enhancing tissue repair and promoting healing in ischemic flap studies (113), can also be studied for potential in accelerating post-surgical recovery in spinal TB by facilitating tissue regeneration. Last, nanotechnology may also offer a promising frontier, with nanomaterials already proving effective in bone metastasis treatment (114). These materials could be explored further for their applications in spinal TB to improve drug delivery, enhance infection control, and support bone tissue regeneration.
5 LimitationsDespite the comprehensive nature of this bibliometric analysis, several limitations must be acknowledged. First, the study relied solely on the Scopus database for data retrieval, which, although extensive, may not capture all relevant publications. Second, the analysis focused primarily on quantitative metrics such as the number of publications, citations, and author affiliations, which, while informative, may not fully capture the qualitative aspects of the research, such as the clinical impact or real-world applicability of the findings. However, to address this, the discussion section incorporates qualitative insights summarizing key advancements, such as minimally invasive techniques and the integration of artificial intelligence, to provide context and relevance to the findings. Additionally, the reliance on publication and citation counts as an indicator of influence or importance, which may introduce a bias towards more recent works, potentially overlooking less cited but still significant contributions to the field. Another limitation is categorizing publications into orthopaedic and neurosurgical domains based on explicit mentions, which may not fully capture the multidisciplinary nature of spinal TB treatment, where collaboration between orthopaedic surgeons, neurosurgeons, and other specialists is common. Future studies are necessary to explore and document interdisciplinary practices better, especially in employing qualitative methods, such as expert interviews or case reviews.
6 ConclusionThis bibliometric analysis of worldwide publications on surgical management for spinal TB reveals a significant evolution in the field, marked by advancements in surgical techniques and the increasing integration of technology. Over the years, there has been a steady increase in research output, reflecting the growing recognition of the importance of surgical intervention in managing spinal TB, particularly in cases of spinal instability or neurological complications. Subsequently, the comparison between orthopaedic surgery and neurosurgery publications reveals that orthopaedic surgery has a higher volume of research output in this field, indicating its predominant role in spinal TB management. However, both disciplines contribute valuable insights and advancements to the surgical treatment of this challenging condition.
The study highlights key trends in the evolution of surgical methods, from basic early techniques to the adoption of minimally invasive procedures and the recent incorporation of artificial intelligence and machine learning into surgical practice. The posterior approach remains the most frequently discussed surgical method, but there is also significant interest in anterior approaches, minimally invasive techniques, and the use of advanced instrumentation. The combination of surgical intervention with chemotherapy and anti-TB treatment further underscores the importance of a multidisciplinary approach to managing spinal TB. This study provides a detailed overview of the global research landscape on surgical management for spinal TB, offering valuable guidance for future research and clinical practice development in managing this debilitating disease.
Data availability statementThe raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributionsRR: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing. MI: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Software, Visualization, Writing – original draft. AL: Conceptualization, Formal Analysis, Methodology, Visualization, Writing – review & editing. DS: Conceptualization, Formal Analysis, Methodology, Visualization, Writing – original draft. DD: Conceptualization, Formal Analysis, Methodology, Visualization, Writing – original draft. EB: Conceptualization, Formal Analysis, Methodology, Visualization, Writing – original draft.
FundingThe author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statementThe author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References1. Pawar UM, Kundnani V, Agashe V, Nene A, Nene A. Multidrug-resistant tuberculosis of the spine—is it the beginning of the end? Spine (Phila Pa 1976). (2009) 34:E806–10. doi: 10.1097/BRS.0b013e3181af7797
PubMed Abstract | Crossref Full Text | Google Scholar
4. Kiran NAS, Vaishya S, Kale SS, Sharma BS, Mahapatra AK. Surgical results in patients with tuberculosis of the spine and severe lower-extremity motor deficits: a retrospective study of 48 patients. J Neurosurg Spine. (2007) 6:320–6. doi: 10.3171/spi.2007.6.4.6
PubMed Abstract | Crossref Full Text | Google Scholar
5. Turgut M. Spinal tuberculosis (Pott’s disease): its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurg Rev. (2001) 24:8–13. doi: 10.1007/PL00011973
PubMed Abstract | Crossref Full Text | Google Scholar
8. Dartois VA, Rubin EJ. Anti-tuberculosis treatment strategies and drug development: challenges and priorities. Nat Rev Microbiol. (2022) 20:685–701. doi: 10.1038/s41579-022-00731-y
PubMed Abstract | Crossref Full Text | Google Scholar
10. Pandita A, Madhuripan N, Pandita S, Hurtado RM. Challenges and controversies in the treatment of spinal tuberculosis. J Clin Tuberc Other Mycobact Dis. (2020) 19:100151. doi: 10.1016/j.jctube.2020.100151
PubMed Abstract | Crossref Full Text | Google Scholar
11. Alam MS, Phan K, Karim R, Jonayed SA, Munir HKM, Chakraborty S, et al. Surgery for spinal tuberculosis: a multi-center experience of 582 cases. J Spine Surg. (2015) 1:65–71. doi: 10.3978/j.issn.2414-469X.2015.07.03
PubMed Abstract | Crossref Full Text | Google Scholar
12. Kilinc F, Setzer M, Behmanesh B, Jussen D, Geßler F, Prinz V, et al. Surgical management and clinical outcome of cervical, thoracic and thoracolumbar spinal tuberculosis in a middle-European adult population. Sci Rep. (2023) 13:7000. doi: 10.1038/s41598-023-34178-9
PubMed Abstract | Crossref Full Text | Google Scholar
13. Kumar V, Salaria AK, Aggarwal A, Dhatt SS. Surgical approaches in management of spinal tuberculosis. Ann Natl Acad Med Sci. (2021) 57:214. doi: 10.1055/s-0041-1731596
Crossref Full Text | Google Scholar
14. Tang Y, Wu W, Yang S, Wang D-G, Zhang Q, Liu X, et al. Surgical treatment of thoracolumbar spinal tuberculosis—a multicentre, retrospective, case-control study. J Orthop Surg Res. (2019) 14:233. doi: 10.1186/s13018-019-1252-4
PubMed Abstract | Crossref Full Text | Google Scholar
15. Liu J, Wan L, Long X, Huang S, Dai M, Liu Z. Efficacy and safety of posterior versus combined posterior and anterior approach for the treatment of spinal tuberculosis: a meta-analysis. World Neurosurg. (2015) 83:1157–65. doi: 10.1016/j.wneu.2015.01.041
PubMed Abstract | Crossref Full Text | Google Scholar
16. Muheremu A, Niu X, Wu Z, Tian W. Study on anterior and posterior approaches for spinal tuberculosis: a meta-analysis. Eur J Orthop Surg Traumatol. (2015) 25:69–76. doi: 10.1007/s00590-014-1508-y
Crossref Full Text | Google Scholar
17. Yang P, Zang Q, Kang J, Li H, He X. Comparison of clinical efficacy and safety among three surgical approaches for the treatment of spinal tuberculosis: a meta-analysis. Eur Spine J. (2016) 25:3862–74. doi: 10.1007/s00586-016-4546-9
PubMed Abstract | Crossref Full Text | Google Scholar
18. Arifin J, Biakto KT, Johan MP, Anwar StFZ. Clinical outcomes and surgical strategy for spine tuberculosis: a systematic review and meta-analysis. Spine Deform. (2023) 12(2):271–91. doi: 10.1007/s43390-023-00785-9
PubMed Abstract | Crossref Full Text | Google Scholar
19. Zhong Y, Yang K, Ye Y, Huang W, Liu W, Luo J. Single posterior approach versus combined anterior and posterior approach in the treatment of spinal Tuberculosis: a meta-analysis. World Neurosurg. (2021) 147:115–24. doi: 10.1016/j.wneu.2020.12.023
留言 (0)