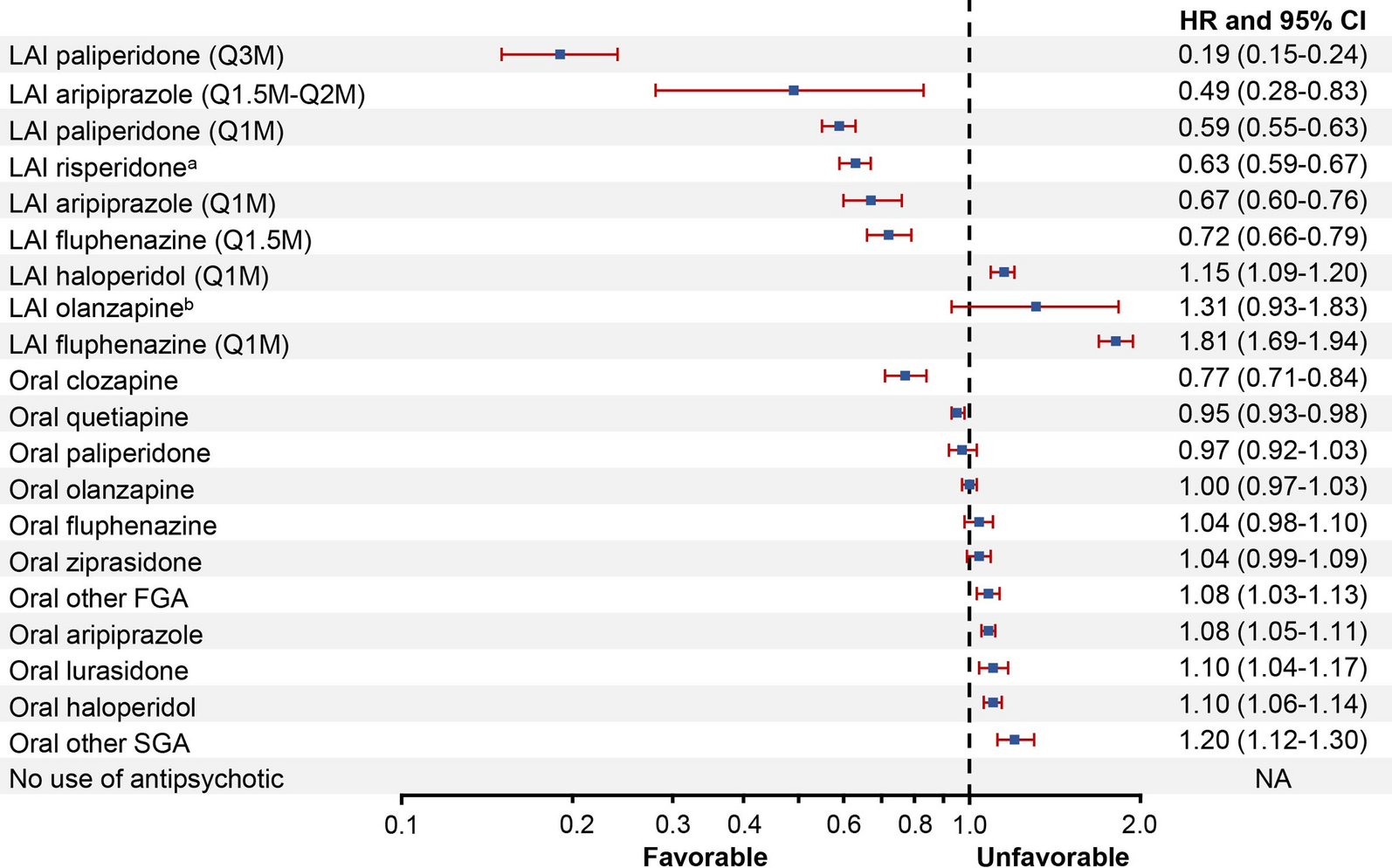
This national study represents the first comparative effectiveness analysis of LAIs with varying dosing intervals vs. OAPs, overall and by type of antipsychotic agent, among Medicare Part D beneficiaries with schizophrenia. We found that among 152,835 Medicare beneficiaries with schizophrenia, LAIs when grouped by dosing intervals generally fared better than OAPs with respect to antipsychotic discontinuation, psychiatric hospitalization, and treatment failure. Across LAIs grouped by dosing intervals, this translated to a 26–45% lower risk of treatment failure relative to OAPs. Our results are consistent with a prior study of antipsychotic treatments using within-individual analyses, which found that LAIs were associated with the lowest risk (20–35%) of treatment failure in a cohort of 29,823 Swedish patients with schizophrenia [11]. In addition to being the first to generate similar evidence in the US Medicare population, our analysis was able to build on this prior Swedish study [11] given the availability of more recent data covering the period when LAIs of longer than monthly dosing intervals were available.
A key finding of this study was that across all agents, LAI paliperidone Q3M—the only LAI with the longest dosing interval available during our study period—had the lowest risk of treatment failure. Not only did it have the lowest risk in terms of ranking, but the risk was substantially lower in terms of magnitude; this remained true even when compared to other LAIs. The risk of treatment failure on LAI paliperidone Q3M was 47% lower relative to oral risperidone, the most commonly used antipsychotic agent in our study population, and 33%, 38%, and 45% lower, respectively, when compared to LAI risperidone Q0.5M, LAI aripiprazole Q1M, and LAI haloperidol Q1M.
For the remaining LAIs, however, substantial heterogeneity was observed when the LAIs grouped by dosing intervals were further broken out by type of agent. Even LAIs of the same dosing interval but different antipsychotic agents had diverse results. For instance, second-generation LAI paliperidone Q1M was consistently associated with a lower risk of treatment failure across all reference groups. These results are consistent with a real-world pragmatic trial that compared LAI paliperidone Q1M with OAPs (including oral risperidone and paliperidone) for delaying time to treatment failure [26]. On the other hand, second-generation LAI olanzapine (primarily Q1M) and first-generation LAI fluphenazine Q1M had a higher risk of treatment failure across all reference groups. First-generation LAI haloperidol Q1M also had a higher risk of treatment failure compared to the two second-generation LAI reference groups (LAI risperidone mainly Q0.5M and aripiprazole Q1M) and was only marginally better than oral risperidone. At the same time, first-generation fluphenazine of a longer dosing interval (i.e., Q1.5M) and second-generation risperidone of a shorter dosing interval (i.e., Q0.5M) were consistently associated with a lower risk of treatment failure across all reference groups. These findings suggest that both the antipsychotic agent’s profile (effectiveness and side effects) and its length of dosing interval may influence treatment outcomes.
Another noteworthy finding of this study was that the results of treatment failure during use of each antipsychotic agent were largely driven by the risk for antipsychotic discontinuation while on that agent. Most second-generation LAIs had a lower risk of antipsychotic discontinuation. In fact, the only second-generation LAI that did poorly with respect to the outcome of antipsychotic discontinuation was LAI olanzapine, which requires patient observation for at least 3 h in a registered facility after injection to monitor for post-injection delirium/sedation syndrome [28]. LAI paliperidone Q3M was associated with an 81% lower risk, whereas the remaining second-generation LAIs had a 33% to 51% lower risk of antipsychotic discontinuation compared to oral risperidone. On the other hand, we found that the first-generation agents LAI haloperidol Q1M and LAI fluphenazine Q1M were associated with a greater risk of discontinuation relative to oral risperidone, which is noteworthy given the differing side-effect profiles for first-generation vs. second-generation antipsychotics. However, both of these first-generation LAIs had a lower risk of psychiatric hospitalization relative to oral risperidone despite having a higher risk of discontinuation. This implies that for the time period when patients are receiving these first-generation LAIs, they do prevent hospitalizations, but unfortunately patients are less likely to stay on these treatments and discontinue as a result of adverse events such as extrapyramidal symptoms [5].
In fact, our results for psychiatric hospitalization showed that during periods when patients were receiving LAIs, regardless of whether first-generation or second-generation LAIs (except LAI olanzapine) or short or long dosing interval, the risk of hospitalization was somewhat similar across all LAIs and was significantly lower relative to oral risperidone. These findings suggest that when patients are administered LAIs, the agents are effective and prevent negative outcomes such as psychiatric hospitalizations, but negative outcomes are more likely to occur because these patients discontinue treatment. The outcome of antipsychotic discontinuation would trigger a new treatment exposure period of “no antipsychotic” use in our study (i.e., ≥ 60-day period without any antipsychotic medication after the last antipsychotic prescription’s days’ supply was exhausted) and, indeed, these periods of no antipsychotic use were associated with a 11% to 32% higher risk of psychiatric hospitalization compared to periods with use of oral risperidone or other LAI reference groups.
It is worth noting that among OAPs, oral clozapine had the lowest risk of antipsychotic discontinuation and psychiatric hospitalization, albeit it was associated with a much higher risk for negative outcomes than other second-generation LAIs, especially paliperidone Q3M. The better outcomes for clozapine may be explained by the frequent contact with medical staff necessitated by regular monitoring of blood cell count [29], thus providing a similar touchpoint that injections provide for patients who receive an LAI.
These findings are important to providers, payers, and policymakers. While our study confirms that LAIs are indeed more effective at preventing treatment failure than OAPs, the fact remains that very few Medicare beneficiaries are receiving these treatments. Fewer than 20% of patients in our sample had evidence of LAI use during follow-up, despite the fact that 80% of the sample had experienced at least one period of ≥ 60 days without any antipsychotic use and 72% had at least one psychiatric hospitalization over the same time frame. This is consistent with prior research, which has shown that LAIs are not prescribed as often as OAPs [3, 30, 31]. Furthermore, LAIs of longer dosing intervals had the lowest rates of use in our sample. Hence, efforts should be made to ensure that LAIs, especially LAIs with longer dosing intervals, are not underutilized among appropriate candidates. For instance, the cost of LAIs (particularly newer, second-generation LAIs) has been cited by physicians as a reason for not prescribing these treatments [3]. However, providers should note that most Medicare beneficiaries with schizophrenia receive low-income subsidies to cover their cost sharing and, hence, would face minimal out-of-pocket costs for their LAI treatment [32]. Payers should also note that the increased drug costs of LAI use may be offset by lower medical costs resulting from fewer psychiatric hospitalizations [33].
Our study has strengths and limitations. A key strength of our study was the use of national data, with 100% capture of all fee-for-service Medicare beneficiaries with schizophrenia, allowing for a larger and more generalizable sample than previous analyses. While fee-for-service Medicare beneficiaries represented the majority of the overall Medicare population during our study period (2006–2019), enrollment in Medicare Advantage plans has increased considerably in recent years. Hence, future research should extend these analyses in the Medicare Advantage population. Furthermore, our results are not generalizable to patients with other sources of insurance coverage such as Medicaid and commercial insurance; thus, future studies are also needed in these populations. Though our study benefited from the large sample size permitted by 100% Medicare claims data, such administrative claims databases do not permit an accurate examination of the incidence of common antipsychotic adverse effects (e.g., anticholinergic effects, weight gain, insomnia) and how they impacted treatment discontinuation and psychiatric hospitalization. Future analyses with access to real-world clinical data should examine how the incidence of adverse effects impact these outcomes. Another strength of our study was the use of within-individual analyses, in which each person serves as his or her own control. This robust analytic approach has been used in prior observational studies of psychotropic drugs [11, 22, 23] since it adjusts for both the observed confounders (e.g., demographics) as well as unobserved confounders (e.g., genetic makeup, childhood environment) that remain constant within each patient during follow-up [11]. However, it cannot control for time-varying unobserved confounders. While our analyses controlled for key time-varying confounders (temporal order of the antipsychotic, schizophrenia-related hospitalization or emergency room visits within 3 months before the starting date of the subperiod, etc.), we cannot rule out the possibility of unobserved time-varying confounders (e.g., changes in non-psychiatric or psychiatric symptoms and severity, consumption of co-medications) that our analyses did not control for and could still bias our study results. Finally, the CIs for the risk for some outcomes for LAIs of longer dosing intervals (e.g., LAI aripiprazole Q1.5M–Q2M) were quite wide, given smaller sample sizes due to low rates of use in our study population.




留言 (0)