Most of the recommendations were not amended and were endorsed by the working group.
Tab. 2 shows a brief overview of the changes/additions to and clarifications of some amended recommendations of the ESC guidelines for cardiac pacing and CRT. The following text provides details and justifications for any changes made.
Table 2 Changes and additions to/clarifications of the recommendations in the European Society of Cardiology (ESC) guidelinesCRT in patients with persistent or permanent atrial fibrillation
The suggestion that CRT may be considered in patients with heart failure with preserved ejection fraction (HFpEF) from Chapter 6.3 ‘Cardiac therapy in patients with persistent or permanent atrial fibrillation’ has been clarified by the addition of: ‘Placing a CRT device has complications (the risk of complications is higher than with a 1-chamber or 2‑chamber device). It is important to make the decision regarding the installation of a CRT device through shared decision making.’ It has been demonstrated that the complication rate is higher in CRT than conventional pacing [3] and battery life is substantially shorter [4]. This needs to be balanced with the potential benefit of CRT and discussed with the patient. No prospective studies are available on CRT or CSP in patients with HFpEF. It has, however, been demonstrated in a subgroup analysis from the prospective PROSPECT trial that patients with an EF > 35% might benefit from CRT [5]. In addition, the APAF-CRT trial included patients with severely symptomatic permanent atrial fibrillation > 6 months, narrow QRS (≤ 110 ms) and at least one heart failure (HF) hospitalisation in the previous year [6]. Atrioventricular junction (AVJ) ablation plus CRT was superior to drug therapy in reducing both all-cause mortality and the secondary combined endpoint of death of any cause or HF hospitalisation. A benefit in all-cause mortality was observed in patients with preserved EF with no interaction between patients with EF > 35% and those ≤ 35%. Although this was not a comparison to right ventricular (RV) pacing, no previous trial or meta-analysis of AVJ ablation and RV pacing has shown a mortality benefit. Based on the findings of the APAF-CRT trial, it seems that patients fulfilling the inclusion criteria of the APAF-CRT trial should be considered for CRT irrespective of their LVEF.
Upgrade from RV pacing to CRT
Regarding the recommendation from Chapter 6.4 ‘Upgrade from right ventricular pacing to cardiac resynchronisation therapy’, the working group would like to emphasise that the recommendation has now been confirmed by the results from the Budapest CRT trial [7]. This is the first RCT demonstrating the reduction of hard endpoints such as mortality, HF hospitalisation and reverse remodelling by upgrading from a conventional implantable cardioverter defibrillator (ICD) to CRT‑D in patients with significant RV pacing. The recommendation has not been adjusted.
Benefit of adding an ICD in patients with an indication for CRT
A separate Dutch indication guideline has been published for primary prevention during ICD placement in patients with non-ischaemic cardiomyopathy. A reference to this guideline has been added to the recommendation from Chapter 6.6. The rationale of this guideline has been described in detail previously [8]. In summary, there is little evidence in favour of adding defibrillator therapy to CRT in patients with a non-ischaemic aetiology of heart failure. This has also been demonstrated in a recent meta-analysis [9].
Conduction system pacing
The following two recommendations have been added to Chapter 7.2 ‘His bundle pacing’:
1.
A proposed treatment with CSP versus conventional RV or CRT pacing should be discussed with the patient, weighing the advantages and disadvantages, including potential other short- and long-term complications (see Table 5 ‘Advantages and limitations of HBP and of LBBAP’ [EHRA clinical consensus statement on conduction system pacing implantation: endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS) | Oxford Academic (oup.com)] from the EHRA consensus document [10]).
2.
The recommendations on the practical application of CSP as stated in the Table of advice chapter from the EHRA Consensus document [10] have been adopted by the working group.
The current ESC guideline ‘Cardiac pacing and cardiac resynchronisation therapy’ [1] makes limited recommendations on His bundle pacing (HBP) and no recommendations are given on left bundle branch area pacing (LBBAP) given the lack of sufficient data on this modality at the time. However, since 2021, numerous predominantly observational studies on these forms of CSP have been published. In 2023, (1) a European Heart Rhythm Association (EHRA) clinical consensus statement on CSP implantation was published [10] and (2) a document was drawn up by non-European international heart rhythm societies with recommendations on CSP based on this recent literature [11]. An EHRA expert consensus document on when to use CSP is expected in 2025, providing more guidance on the use of this emerging technique.
In the Netherlands, CSP (and LBBAP in particular) has been increasingly applied in clinical practice in recent years, despite the lack of results from ongoing large RCTs. The field therefore needs advice on applying LBBAP pending these results (and an update in the ESC guideline). Given the planning published on the ESC website, an update of the current 2021 guideline is not expected before 2027.
Taken together, the working group has decided to extend the current recommendations from the ESC guideline (where possible) for Dutch practice. The working group wanted to provide scope for applying LBBAP. Consideration has been given to conducting a literature analysis. However, current evidence comes mainly from observational studies. In order to be able to draw up recommendations about LBBAP with any certainty, the results from ongoing RCTs are needed.
Leadless pacing
The recommendations from Chapter 7.4 have been endorsed by the working group. It should be noted that the Netherlands Heart Rhythm Association published an i implementation guideline in 2016 that provides conditions for implanters and the implanting centre under which this technique may be safely used [Intracardiale pacemaker (www.nvvc.nl)]. It formulates recommendations on training and the minimum number of procedures per operator and centre but also recommends the presence of on-site cardiothoracic surgical backup.
Pacing after cardiac surgery and heart transplantation
The recommendation from Chapter 8.2 ‘Pacing after cardiac surgery and heart transplantation’ has been clarified by the addition of: RV pacing is not necessarily the preferred option for permanent epicardial leads.
Epicardial pacing leads have been used extensively for CRT; they have good longevity and should be placed in the posterolateral region [12]. In addition, it has been shown that pacing from an epicardial position can be performed better from the LV apex in children. Given the better synchronicity it can be hypothesised that this is also true for adults [13].
Pacing in rare diseases (Chapter 8.6)
The indication for a device capable of cardiac pacing for permanent atrioventricular block (AVB) is evident in patients with cardiac sarcoidosis in analogy to patients with a different aetiology of AVB. Therefore, the recommendation from Chapter 8.6.6.1 on cardiac sarcoidosis has been amended to recommend implantation of a device for permanent AVB in patients with cardiac sarcoidosis instead of ‘should be considered’.
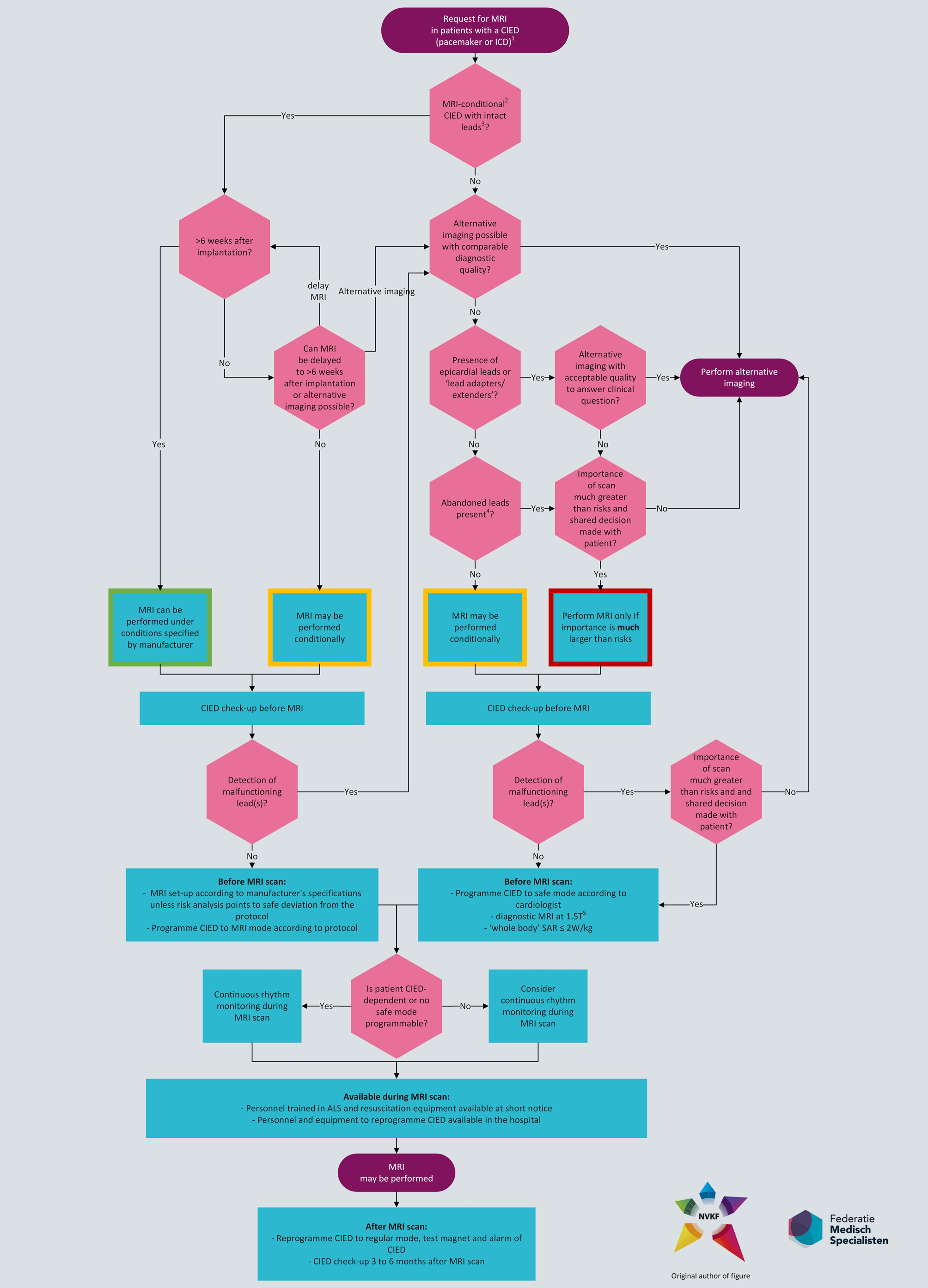
Performing magnetic resonance imaging in patients with a pacemaker or ICD
For recommendations on performing magnetic resonance imaging (MRI) in patients with a pacemaker or ICD, we refer readers to the Dutch guideline module on this subject (authorised by the NVVC in 2024): https://richtlijnendatabase.nl/richtlijn/gebruik_mri_bij_patienten_met_implantaten/mri_bij_elektronisch_cardiaal_implantaat_2024.html. This guideline incorporates more recent literature and gives more detailed practical advice than the current ESC guidelines. There seem to be few contraindications for MRI if the correct precautions are taken. Even patients with abandoned leads or epicardial leads are at low risk when undergoing MRI [14]. The workflow for patients with a pacemaker or ICD where an MRI is requested is summarised in Fig. 1.
The recommendations from Chapter 11.1 will therefore not be applicable for Dutch practice.




留言 (0)