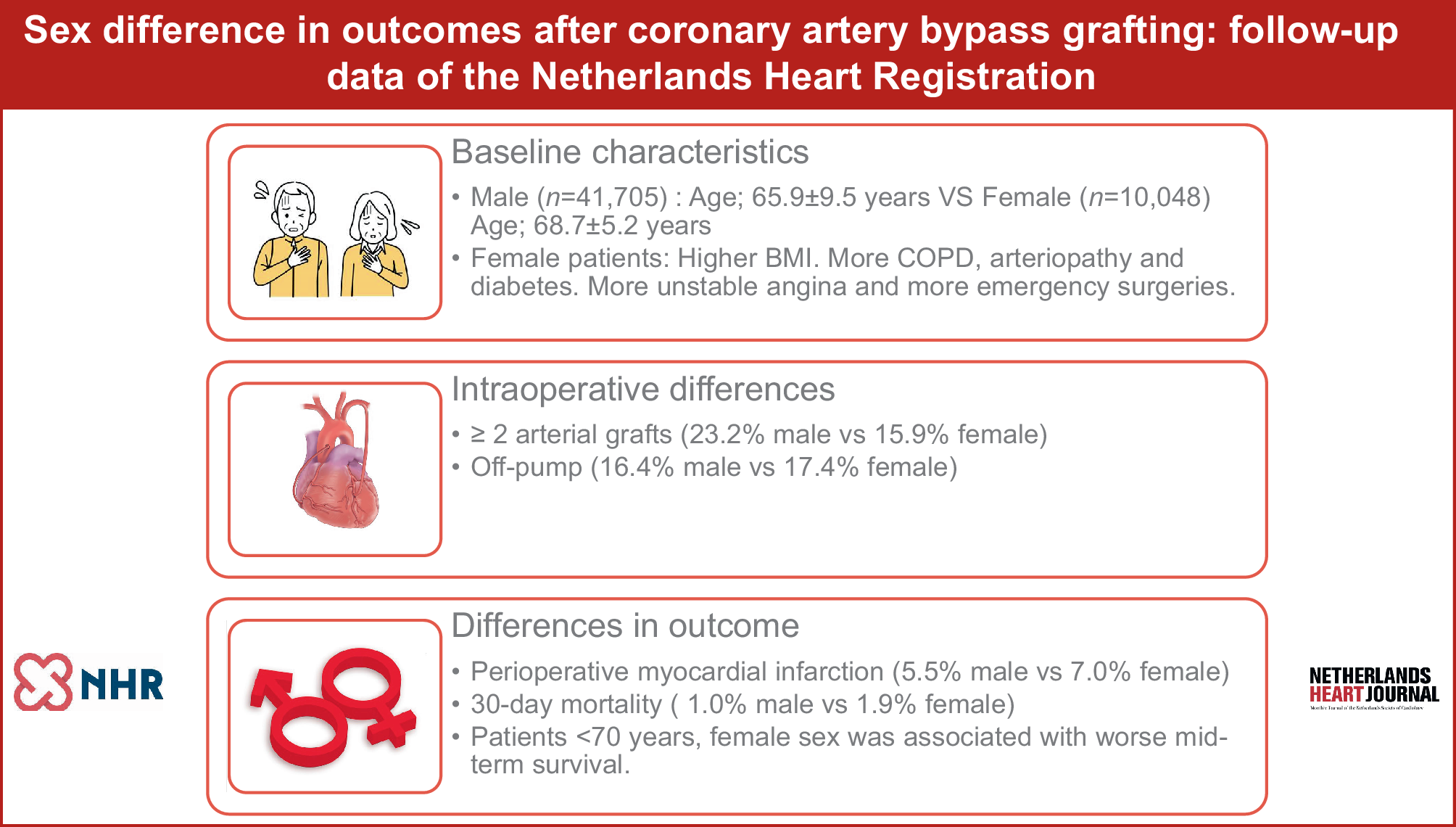
The aim of this study was to assess differences in early and mid-term outcomes between male and female patients undergoing CABG in the Netherlands, thereby determining the factors which contribute to these differences in outcomes. In this large population, we found that women had a higher 30-day and mid-term survival rate after CABG compared to men. Additionally, we found that, in the age subgroup < 70 years, female patients had a worse mid-term mortality. Factors associated with mid-term mortality were: age, chronic lung disease, PVD, DM, serum creatinine > 200 µm/l, recent MI, decreased LVEF and emergency surgery. For patients aged > 70 years, factors associated with worse mid-term survival were the same as the commonly known risk factors for a worse outcome after CABG [9, 10].
Similar results to ours have been described in a study of the national database of the United Kingdom [11]. Our current analysis confirms the considerations of previous studies, which suggested that differences in mortality between sexes may be due to a different preoperative risk profile, presentation of CAD, and in surgical techniques used [12]. The current study shows that the poorer mid-term survival of women is only observed in patients aged < 70 years.
Differences between women and men in the presentation of CAD have been extensively described in earlier studies. Chest pain is more common in women than in men. In women this pain is less frequently caused by atherosclerotic lesions in the major epicardial coronary arteries [13, 14]. Men more frequently suffer from three-vessel and left main disease. Due to the more diffuse character of CAD in women, with less obstructive CAD and more single-vessel disease, non-invasive tests are less accurate in diagnosing CAD [15]. This, then, could lead to a delay in referral, diagnosis and intervention for women and might cause women to present with unstable angina and in emergency settings. Further research is needed on this correlation.
In agreement with other studies, women in our population presented at an older age, and with more comorbidities. It has been suggested that this ‘more complex risk profile’ is explanatory for the worse outcomes after CABG observed in women [16, 17]. Contrary to this claim, several studies found that female sex is a predictor of worse outcome after CABG, even after risk adjustment and propensity-matched analysis [18, 19]. We found female sex to be an independent predictor of worse mid-term mortality, only in the subgroup of patients aged < 70 years. Younger women having a worse outcome after CABG compared to younger man has been described by Vaccarino et al. [19]. Hypothetically, younger women presenting with premature CAD could have sex-related risk factors or be lacking protective factors normally present in women [6]. The protective effect of oestrogen on the cardiovascular system has been thoroughly researched; it is thought to decrease atherosclerotic lesion formation and to improve endothelial function [13]. More diffuse CAD and coronary microvascular dysfunction in women could explain why CABG leads to a higher mortality rate in younger women, as older women have disease patterns more similar to the disease pattern of men and, therefore, they benefit equally from CABG [17].
An important finding of this study is that women were less likely than men to receive ≥ 2 arterial graftsn. Additionally, we found that the use of ≥ 2 arterial grafts was associated with better mid-term outcome after CABG. This finding is in line with a recent review article in which the use of multiple arterial grafts was associated with a better outcome as compared to the use of venous graft material in addition to a single arterial graft [20]. However, in our study population, the use of ≥ 2 arterial grafts was only associated with improved outcomes in patients aged < 70 years.
Women receiving fewer arterial grafts is a phenomenon that has been described in several other studies [21, 22]. An explanation for this observation could be that women are more likely to present in an emergency setting. Mickleborough et al. have demonstrated a decreased use of the left internal mammary artery and decreased multi-arterial use in emergency settings [21]. Arguments against using the radial artery in women include the possibility that their radial artery might be smaller [23]. Lawton et al. found that there was a significant difference in the size of the radial artery of women and men, even when indexed for a difference in body surface area [23]. A recent systemic review and meta-analysis did not find a difference in vein graft patency between men and women, which indicates that the use of arterial grafts in women is as important as it is in men, assuming that the incidence of saphenous vein graft failure is the same in men and in women because it has been shown that the patency is the same [24].
In agreement with earlier studies [25], the present study shows that women received fewer distal anastomoses than men. Complete revascularisation has been associated with a better long-term outcome after CABG [25]. It might be assumed that complete revascularisation is less frequently achieved in women because women have smaller and more diffusely diseased coronary arteries. This then could lead to a worse mid- and long-term outcome. Our findings confirm that the incidence of coronary reintervention is higher in women than in men, which could indicate that, before the reintervention, there is ongoing ischaemia from non-revascularised arteries. However, reintervention data of the NHR are not corrected for competing risks.
The use of the OPCAB technique is correlated with an improved mid-term survival, in both age subgroups. In both subgroups, OPCAB was used more frequently in women than in men. Several studies have described the benefit of OPCAB over ONCAB in women [26, 27]. Evidence for the benefits of OPCAB hase especially been shown in high-risk patients of both sexes [28]. Consequently, one of the reasons why women seem to benefit more from OPCAB might be that they have a higher preoperative risk when presenting for surgery. These findings call for further research into OPCAB surgery in women.
In addition to a higher late mortality rate, women also have a higher reintervention rate than men in our study population. This difference was particularly significant for unplanned PCI reinterventions. This finding is in line with the observations of Guru et al. [29]. However, after propensity matching and risk adjustment, the difference in the number of reinterventions between the sexes was no longer seen in their study. Other investigators have reported that women are more likely to present with recurrent angina pectoris postoperatively and that postoperative MI occurs more frequently in women [19, 30]. Unfortunately, recurrent postoperative angina is not included as an outcome in the registry data of the NHR. On the other hand, we found that postoperative MI occurred more often among women than among men.
Limitations
The current study has some limitations mostly due to the retrospective nature of the study. Additionally, some variables, such as ECC and cross-clamp time, were missing in a relatively large proportion of our study population. The primary endpoint of the study is all-cause mortality. The registry does not include the cause of death, which could be relevant for the interpretation of mortality rates.




留言 (0)