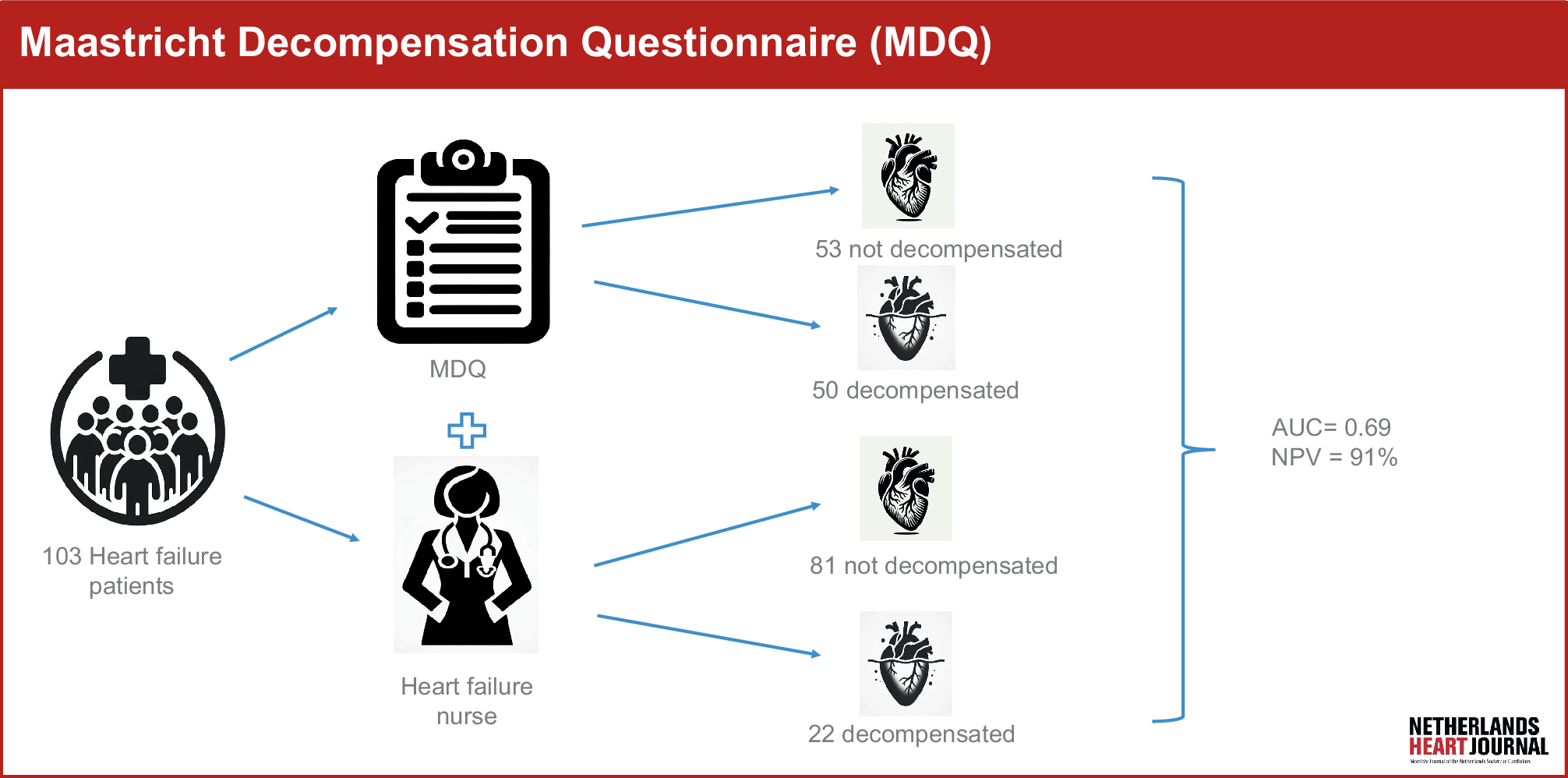
Our study suggests that the self-administered MDQ can assist in distinguishing between decompensated and non-decompensated HF patients, which may be a crucial step in identifying those at risk and preventing further deterioration.
Comparable risk models
Berge et al. assessed the prognostic accuracy of the National Early Warning Score 2, a clinical risk score incorporating various physiological measurements, for predicting mortality in HF patients [23]. They reported an AUC score of 0.65, which was comparable to the prognostic accuracies of high-sensitivity cardiac troponin T (AUC 0.65) and NT-proBNP (AUC 0.67) within their cohort. Kerexeta et al. developed an AI model to predict decompensation in HF patients, utilising signs, symptoms and vital parameters from 488 consecutive HF patients over an average follow-up period of 12.6 months [22]. Their model achieved an AUC score of 0.69, a result that aligns with our findings. In another study, Larburu et al. developed an AI model to identify decompensated HF outpatients, using telemonitoring data including signs, symptoms, vital parameters and clinical data collected from 242 HF patients over a 44-month period [24]. Their model’s performance was also similar to that of ours, with an AUC of 0.67.
Despite the inclusion of larger and more comprehensive datasets in all three trials, along with the use of sophisticated analysis methods, it is noteworthy that these models did not outperform our approach, which relies on a questionnaire based on patient-reported signs and symptoms, in identifying patients at risk. This suggests that the quality of data used in developing the risk model may be just as critical, if not more so, than the quantity of data [25]. HF is a highly heterogeneous syndrome, and the clinical presentation can vary significantly among patients. It is improbable that a single model, often based on retrospective data, can effectively identify all patients at risk. Instead of adhering to a ‘one size fits all’ approach, it is essential to individualise risk monitoring to accommodate the heterogeneity inherent to the HF syndrome. This individualised approach can significantly enhance the diagnostic accuracy of risk models. This principle extends to HF treatment as well, where numerous efforts have been made to customise HF therapy based on patients’ phenotypic profiles. Recognising and addressing the diversity within the HF patient population is crucial for improving both diagnostic accuracy and treatment outcomes [26, 27].
Individualisation of risk scores
The LINK-HF trial conducted telemedicine-based physiological data collection to predict HF hospitalisation, achieving an AUC of 0.86 for that model [28]. A hundred elderly HF patients with moderate symptoms were enrolled in the study. Initially, patient data, including heart rate, respiratory rate, walking and body posture, among other factors, were collected during a training period to establish individual baselines. Subsequently, alerts were triggered if data deviated from these baselines. This personalised approach yielded promising results.
Despite utilising different input data, our plan includes individualising our model as well. In this context, treating physicians will have the capability to adjust the MDQ according to the patient’s profile. For example, NYHA class III patients often experience dyspnoea during light exercise, leading to higher MDQ scores and potentially more false-positive results. Our findings support this, as patients who were incorrectly classified by the MDQ had significantly higher NYHA classifications compared to those classified correctly. To address these variations, we will conduct an additional trial involving patients with more advanced HF to evaluate the weighting of MDQ questions based on HF severity. Additionally, as the MDQ will be regularly administered, changes in MDQ scores over time will be incorporated into risk determination. These enhancements will be prospectively evaluated in a clinical trial to further refine and validate our approach.
Additional findings
Evaluating the fluid status of patients with HF poses a considerable challenge due to the limited diagnostic accuracy of most signs and symptoms [29]. The discriminative power of fatigue and weight gain was notably disappointing. Fatigue is a frequently observed symptom that is linked with a range of other medical conditions, and it is not exclusive to HF. Weight gain exhibited a poor CITC, indicating a weak association with total MDQ scores, which is in line with previous findings [30]. This phenomenon could be attributed to the tendency of HF patients, during decompensation, to lose their appetite and develop a catabolic state, resulting in the loss of muscle and fat mass while accumulating fluid weight, thereby maintaining overall weight stability. Consequently, weight may not be suitable for assessing fluid status when monitoring patients. Nevertheless, changes in weight could still prove valuable for monitoring weight loss following the initiation of diuretic therapy.
Ultimately, our study has affirmed that the previously selected MDQ cut-off value (≥ 10) was indeed the most suitable choice in terms of achieving optimal sensitivity and specificity. Additionally, the correctness of our item selection was confirmed by the high internal consistency of the instrument. These outcomes provide strong validation for our expert-based approach and underscore the potential of implementing the MDQ as a valuable tool in clinical practice. By incorporating the MDQ into eHealth interventions, risk prediction can be optimised, enhancing the remote monitoring of HF patients.
Limitations
In this study, HF nurses assessed patients’ fluid status using standard clinical evaluations, though more precise methods like right heart catheterisation were not used. Still, it is common practice to evaluate fluid status through clinical evaluation without advanced techniques. Independent evaluation of patients’ fluid status might have improved the diagnosis of decompensation. Nevertheless, we found in an earlier trial that there was excellent interobserver reliability in evaluating the clinical status of HF patients among our group of HF nurses. Additionally, patients self-reported weight changes without verification by wearable devices, which could introduce inaccuracies. The MDQ was administered once for clinical evaluation. However, the intention is for the MDQ to be used regularly. Still, most risk scores used in eHealth products were not evaluated before their introduction. Therefore, this pilot validation provides insights for a more evidence-based approach to risk identification in HF patients. Finally, a limited number of psychometric properties of the MDQ have been evaluated, limiting the conclusions we can make about the reliability and validity of the questionnaire. Future trials are necessary to clarify this.




留言 (0)