
記住我

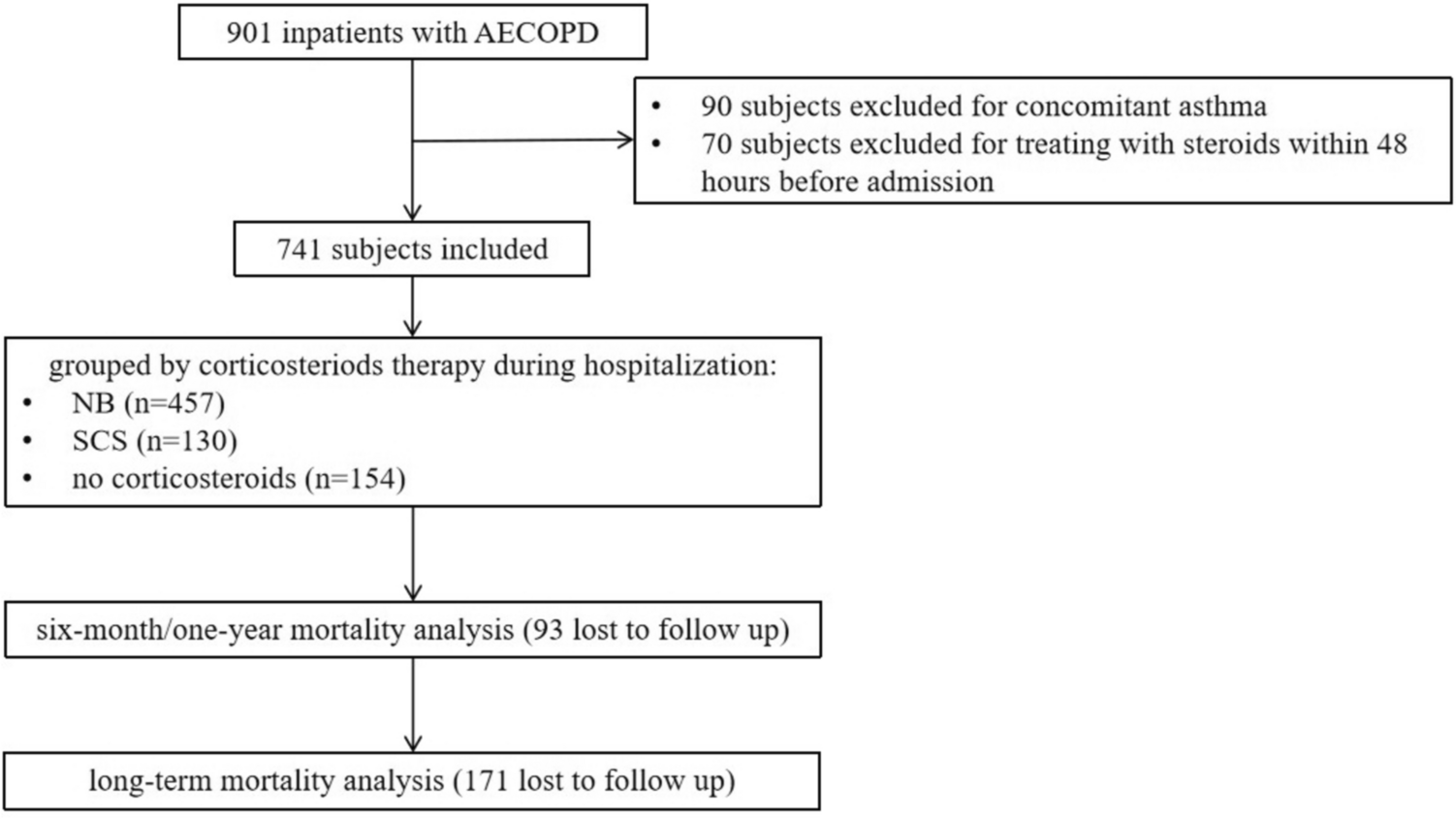






There were 741 patients who met the inclusion criteria finally enrolled the study. The median age was 69 years, and 683 patients were male (92.17%). The median follow-up time in our study was 41 months and the maximum follow-up time was 74 months. A total of 216 patients (37.89%) died during the follow-up period. Among them, 87 (11.74%) died within one year, and nearly half of them (49) died within six months after discharge. There were 457 patients in the NB group, 130 in the SCS group, and 154 in the non-corticosteroid group.
The SCS-Treated Patients had the Worst Baseline Condition at the Beginning of the AE CourseThe baseline characteristics of the participants were showed in Table 1. The non-corticosteroid group showed the best overall condition compared with the other two groups. The proportion of patients with inhaler therapy during stable stage was also the lowest in the non-corticosteroid group compared to the NB group and the SCS group (50.6% vs. 60.4% vs. 72.3%, P = 0.014). Most patients were administered NB (61.7%) as steroid therapy. Physicians tended to use SCs to treat patients with the worst lung function, shortest 6 MWD, most severe dyspnea with the lowest PaO2, lowest SaO2, highest PaCO2 and highest frequency of AEs in the previous year. In terms of comorbidities and complications, patients (52.3%) complicated with respiratory failure were more likely to be treated with SCs and those (26.0%) complicated with cor pulmonale were more likely to be treated with NB.
Table 1 Baseline characteristicsNebulized Budesonide Therapy During Hospitalization was Independent Protective Factor of Six-Month MortalityThe changes in condition during hospitalization and follow-up were showed in Table 2. Patients in the NB group had significant improvement on mMRC (− 1 vs. 0, P = 0.014) and CAT (− 6 vs. − 4, P = 0.018) compared to patients in the non-corticosteroid group. SCS group had the highest proportion of patients treated with triple therapy during stable stage after discharge compare to the other two groups (68.5% vs. 62.1% vs. 50.6%, P = 0.006). Compared to the non-corticosteroid group, NB group showed a lower six-month mortality after discharge (5.9% vs. 13.2%, P = 0.017) (Table 2). Kaplan–Meier survival analysis further compared the impact of NB and SCs during hospitalization on six-month, one-year and long-term mortality over follow-up. Compared to patients treated without steroids, those treated with NB during hospitalization had a significantly lower risk of death over long-term follow-up (P = 0.047) (Fig. 2). SCS group showed a better survival trend than the non-corticosteroid group (Fig. 2). Although the results of the log-rank analysis did not reach statistical significance, the Wilcoxon analysis showed that SCs therapy had a positive impact on survival during the early stage of follow-up (P = 0.038). To eliminate the interference of disturbing factors including age, FEV1/FVC, frequency of AEs in the previous year, respiratory failure, cor pulmonale, mMRC, CAT and inhaler therapy after discharge, we used Cox proportional hazards regression modeling and found that NB therapy was an independent protective factor for six-month mortality afterward compared with treatment without steroid therapy (adjusted HR 0.36; 95% CI 0.15–0.88).
Table 2 Condition changes during hospitalization and follow-upFig. 2
Kaplan–Meier survival curves for the impact of NB and SCS on six-month (A), one-year (B) and long-term (C) mortality after discharge in AECOPD patients. A: NB vs. no corticosteroids, P = 0.005, SCS vs. no corticosteroids, P = 0.087, NB vs. SCS, P = 0.824; B: NB vs. no corticosteroids, P = 0.028, SCS vs. no corticosteroids, P = 0.082, NB vs. SCS, P = 0.786; C: NB vs. no corticosteroids, P = 0.047, SCS vs. no corticosteroids, P = 0.160, NB vs. SCS, P = 0.993. NB: nebulized budesonide; SCS: systemic corticosteroid
The Benefit of Nebulized Budesonide Therapy on Survival Prognosis was More Significant in Certain SubgroupsWe conducted subgroup analysis and found that patients with NB therapy during hospitalization, especially in patients aged 65 and older (adjusted HR 0.31; 95% CI 0.11–0.90), patients with BMI of < 25 kg/m2 (adjusted HR 0.33; 95% CI 0.12–0.92), patients with smoking index of > 40 packets/year (adjusted HR 0.17; 95% CI 0.04–0.79), patients with less than 2 AEs in the previous year (adjusted HR 0.05; 95% CI 0.01–0.38), patients with blood eos count < 200 cells/µl (adjusted HR 0.31; 95% CI 0.11–0.82) or patients without concomitant cor pulmonale (adjusted HR 0.31; 95% CI 0.10–0.93) had a more significant reduction in six-month mortality (Fig. 3). Surprisingly, although a larger proportion of physicians chose to use NB to treat patients with concomitant cor pulmonale, NB therapy had a positive effect on survival in those who did not have. Subsequently, we conducted survival analysis for patients with concomitant cor pulmonale and found that treatment with SCs, but not NB, during hospitalization could remarkably reduce long-term mortality during follow-up (P = 0.010) (Supplementary Figure S1).
Fig. 3
Forest plot of Subgroup analysis for mortality within six months of follow-up. Hazard ratio (HR) were adjusted for age, baseline post-bronchodilator FEV1/FVC, frequency of AEs in the previous year, respiratory failure, cor pulmonale, mMRC, CAT and inhaler therapy after discharge. No steroids, patients without corticosteroid therapy; NB, patients with nebulized budesonide therapy; HR, hazard ratio; GOLD, Global Initiative for Chronic Obstructive Lung Disease; AE, acute exacerbation; BMI, body mass index; EOS, eosinophil count
Nebulized Budesonide with Cumulative Dose Less than 60 mg Might be PreferredSubsequently, the total dosage of budesonide was stratified by a gradient of 20 mg: 0 mg, 1–20 mg, 21–40 mg, 41–60 mg, 61–80 mg, 81–100 mg, and > 100 mg. The mortality of the 1–20 mg, 21–40 mg and 41–60 mg groups were significantly reduced within six months of follow-up compared to that of the 0 mg group (P = 0.025, P = 0.037, and P = 0.047, respectively) (Fig. 4). We then used 60 mg as the cutoff point to stratify the population into three groups (0 mg, 1–60 mg, > 60 mg). The clinical admission conditions of patients who received nebulized budesonide were significantly worse than those who did not receive nebulization, while there was no difference between the 1–60 mg group and > 60 mg groups in these aspects (Supplementary Table S1). We further compared the effects of budesonide dosage during hospitalization on mortality among the 0 mg, 1–60 mg and > 60 mg groups and found that patients who received 1–60 mg budesonide had the best sustained survival prognosis during the entire follow-up (1–60 mg vs. 0 mg, P = 0.033, 1–60 mg vs. 60 mg, P = 0.049, respectively) (Fig. 5), which was still significant (adjusted HR 0.39; 95% CI 0.17–0.92) over six months of follow-up after adjustment.
Fig. 4
Kaplan–Meier survival curves for the mortality within six months of follow-up in AECOPD patients, according to the total dosage of budesonide. 1–20 mg vs. 0 mg, P = 0.025, 21–40 mg vs. 0 mg, P = 0.037, 41–60 mg vs. 0 mg, P = 0.047, comparison between the other every two groups, P > 0.05
Fig. 5
Kaplan–Meier survival curves for the impact of steroids therapy on six-month (A), one-year (B) and long-term (C) mortality in AECOPD patients with cor pulmonale. A: 0 mg vs. 1–60 mg, P = 0.004, comparison between the other every two groups, P > 0.05; B: 0 mg vs. 1–60 mg, P = 0.020, comparison between the other every two groups, P > 0.05; C: 0 mg vs. 1–60 mg, P = 0.033, more than 60 mg vs. 1–60 mg, P = 0.049, comparison between the other every two groups, P > 0.05
留言 (0)