
記住我





We read with great interest the recent case report published in the International Journal of Legal Medicine that details the novel description of hemorrhages at the junctions of the posterior intercostal arteries in a single case of suicidal hanging of a 58-year-old male [1]. We would like to corroborate these findings with our own independent observations within a prospective cohort of suicidal hangings. Additionally, we wish to reveal two other morphological signs related to the descending aorta that we have detected in these cases—intimal breaches and subintimal hemorrhages—both of which have not been previously reported in the forensic literature.
The recently identified periadventitial hemorrhages at the origin of the posterior intercostal arteries from the descending aorta may represent a potentially new morphological sign of hanging. The authors of the commented article suggested that these hemorrhages might result from intense respiratory efforts and convulsive body movements during asphyxiation, combined with the excessive stretching of the aorta due to body suspension [1]. We independently observed these hemorrhages in our study of suicidal hangings while also investigating another previously unreported morphological sign—intimal aortic ruptures, which appear to be analogous to Amussat’s breaches in the carotid or vertebral arteries [2, 3]. Furthermore, inspired by a recent publication, we identified another potential aortic lesion associated with hanging: aortic subintimal hemorrhages, analogous to Dominguez-Paez’s sign in the carotid arteries [4].
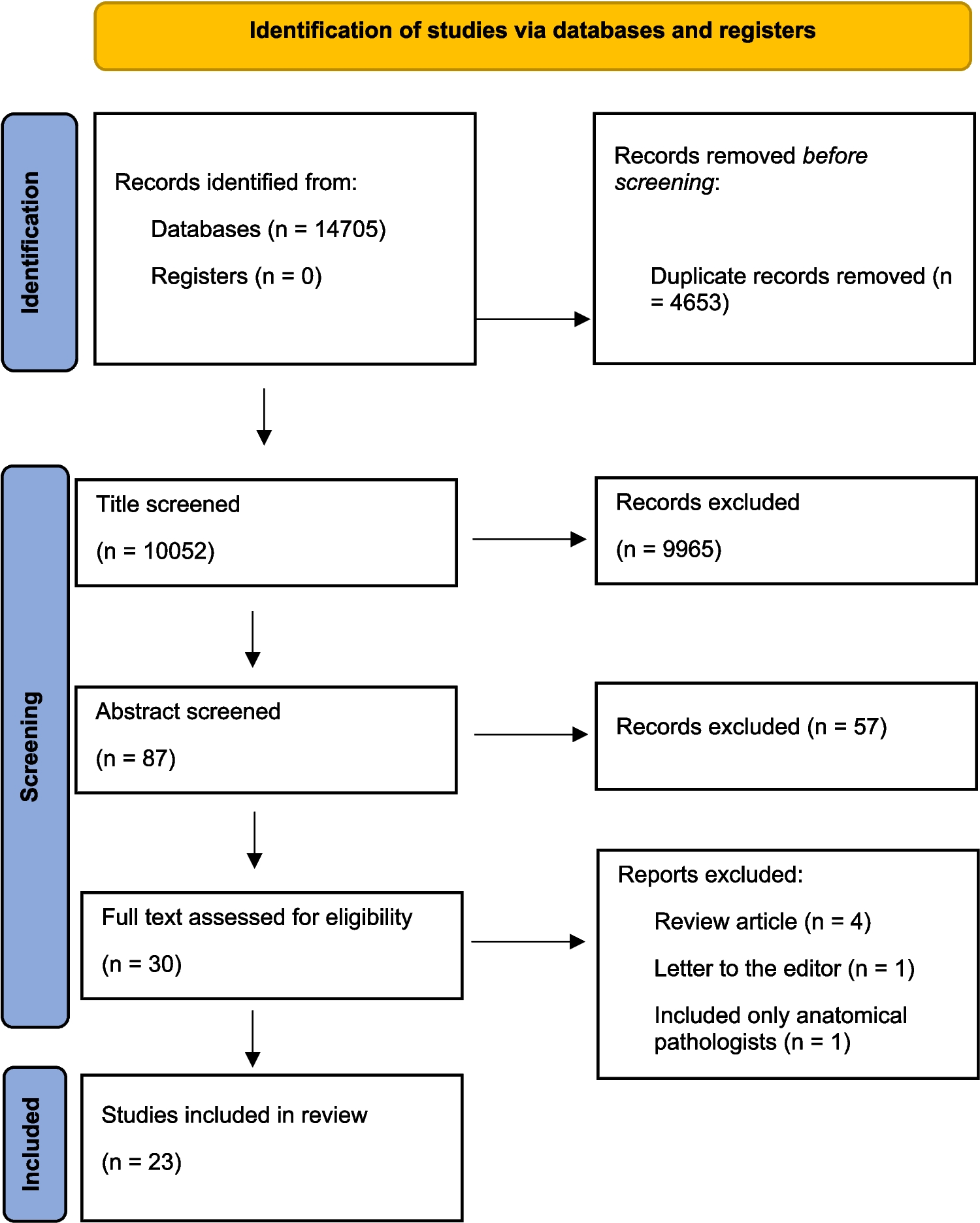
On the basis of our initial observation of intimal breaching of the descending aorta in a suicidal case of complete hanging in 2018, we initiated a prospective investigation of these lesions, which has continued until recently. To date, we have identified six hanging cases with ruptures of the aortic intima within a file of 257 suicidal hanging deaths. Since July 2023, we serendipitously noted the co-occurrence of aortic intimal ruptures and aortic periadventitial hemorrhages at the origin of the posterior intercostal arteries in four cases, three of which were unilocular. Additionally, we observed isolated periadventitial hemorrhages or subintimal aortic hemorrhages in two cases, and solitary aortic intimal ruptures in two others. Histological verification of these lesions was performed in six cases. All the cases involved a rigid ligature (e.g., rope, cable, or plastic tape). Table 1 summarizes the key circumstances and findings in relation to these aortic lesions, while Fig. 1 illustrates representative macroscopic and histological patterns of the discussed aortic lesions.
Table 1 Key circumstances and selected autopsy findings in suicidal hangings with positive detection of aortic lesions (abbreviations: AS = Amussat’s sign, SCM = hemorrhages at origins of sternocleidomastoid muscles, SS = Simon’s sign)Fig. 1
Macroscopic (left column) and histological (right column) patterns of aortic lesions. Upper row: (a) Periadventitial hemorrhages at the origin of the intercostal arteries; (b) Microscopic appearance of periadventitial hemorrhages – dotted circle (H&E, 40x). Middle row: (c) Aortic subintimal hemorrhages near the origin of the left renal artery; (d) Histologically evidenced subintimal and intraintimal erythrocyte extravasations – arrows (H&E, 40x). Lower row: (e) Aortic intimal breaching with evident vital subadventitial bleeding; (f) Histologic presentation of an aortic intimal breach (asterisk) with an underlying subadventitial hemorrhage (H&E, 40x)
In the context of periadventitial hemorrhages at the anatomical origin of the posterior intercostal arteries, we suggest that the complex anatomy of this region makes these junctions particularly vulnerable. The intercostal arteries originating from the upper part of the descending aorta form an acute angle; further caudally, their origin shifts to a more orthogonal position, which likely increases their susceptibility to injury (Fig. 2). Additionally, these small arteries are anchored by surrounding bony structures, unlike the relatively mobile aorta, particularly when unaffected by atherosclerosis. Their vulnerability is further exacerbated by the caliber discrepancy between these small arteries and the aorta, which increases the risk of injury during hanging, especially in cases of complete suspension.
Fig. 2
The partially mobilized descending aorta showing the anatomical arrangement of posterior intercostal arteries, illustrating the gradual change in their origins from an angled to a perpendicular position
Morphologically, the aortic intimal ruptures we detected in hanging cases closely resemble the intimal breaches of the carotid and vertebral arteries known as Amussat’s sign. The primary mechanism behind these lesions involves the forceful elongation and stretching of cervical vessels due to body suspension, with the upper vascular sections being fixed by a ligature to deeper anatomical structures. Direct pressure from the ligature on these vessels serves as a secondary and less common causative mechanism for these lesions [2]. The aorta is anchored at two key fixation points: one at the origin of the aortic arch arteries (thoracic portion) and the other at the origin of the renal arteries (abdominal portion). The predominant occurrence of intimal aortic lesions below these fixation points strongly suggests that the dynamic act of body suspension is the primary pathogenetic factor responsible for these intimal lesions.
Additionally, intense respiratory efforts, forceful body movements during the convulsive phase of asphyxiation, and/or hyperextension of the trunk during decorticate or decerebrate rigidity may also contribute to the formation of aortic intimal lesions [5]. Moreover, complete suspension amplifies both the body’s initial movements when the ligature tightens and the subsequent involuntary body excursions. This idea is supported by the predominance of aortic intimal lesions in full-body hangings and their apparent coincidence with other signs associated with complete suspension, such as Amussat’s sign, hemorrhages at the origin of the sternocleidomastoid muscles, and Simon’s sign (Table 1) [6]. Atherosclerosis may hypothetically serve as a protective factor against the development of intimal aortic lesions by reducing the elasticity of the intercostal arteries and aorta, thereby preventing overstretching and subsequent injury.
The development of aortic intimal lesions is likely influenced by several other factors, including the dynamics of suspension, particularly in long drop hangings (such as slipping, falling, or even jumping into the loop), the type of hanging (complete or incomplete), and individual body parameters, especially body weight. The nature of the ligature also plays a crucial role in these scenarios as a rigid ligature can cause sudden, rapid deceleration (jerk) of the body at the moment of tightening, leading to more pronounced stretching and elongation of the aorta [7]. Consequently, full-body suspension of a robust individual who freely falls or jumps into the loop represents an ideal scenario for breaching the aortic intima or even damaging the inferior vena cava. We hypothesize that subintimal hemorrhages may represent precursor lesions to aortic intimal ruptures, whose appearance is influenced by the same biomechanical variables.
A comprehensive forensic investigation of hanging, including confirmation of its intravital origin and reconstruction of its mechanism, requires meticulous assessment of all internal signs associated with hanging and comparisons with external findings [8, 9]. This thorough evaluation becomes especially critical in cases involving advanced decomposition, survivors of attempted hanging, individuals found in modified positions (e.g., after a ligature rupture, resuscitation attempts), bodies subjected to thermal damage (e.g., complex suicides), cases involving the dissimulation of hanging (e.g., autoerotic fatalities), or situations where other violent mechanisms are camouflaged by postmortem hanging (e.g., manual or ligature strangulation).
The authors would like to highlight the diagnostic and reconstructive benefit of identifying aortic intimal lesions in hanging deaths. These lesions may serve as valuable indicators, particularly pointing to instances with full-body suspension. Furthermore, the detection of aortic periadventitial hemorrhages during organ evisceration should prompt forensic pathologists to consider the potential presence of other aortic lesions while also providing evidence of the lesions’ vitality. This dual significance enhances the utility of these findings in forensic examinations.
We posit that the presented aortic lesions have the potential to be recognized as significant morphological signs of hanging. However, their diagnostic and forensic application requires careful validation through a prospective autopsy study with a larger sample size, including a representative control group. The validation should consider these lesions in the context of other established morphological indicators of hanging, particularly those resulting from body suspension, and evaluate their relationships and potential occurrence in other forms of violent death, especially those involving suffocation. Given the nature of the observed aortic findings, future research may benefit from prospective examinations of similar changes, including subintimal hemorrhages in other aortic branches—such as the subclavian, renal, or iliac arteries—as well as other vascular structures.
留言 (0)