
記住我

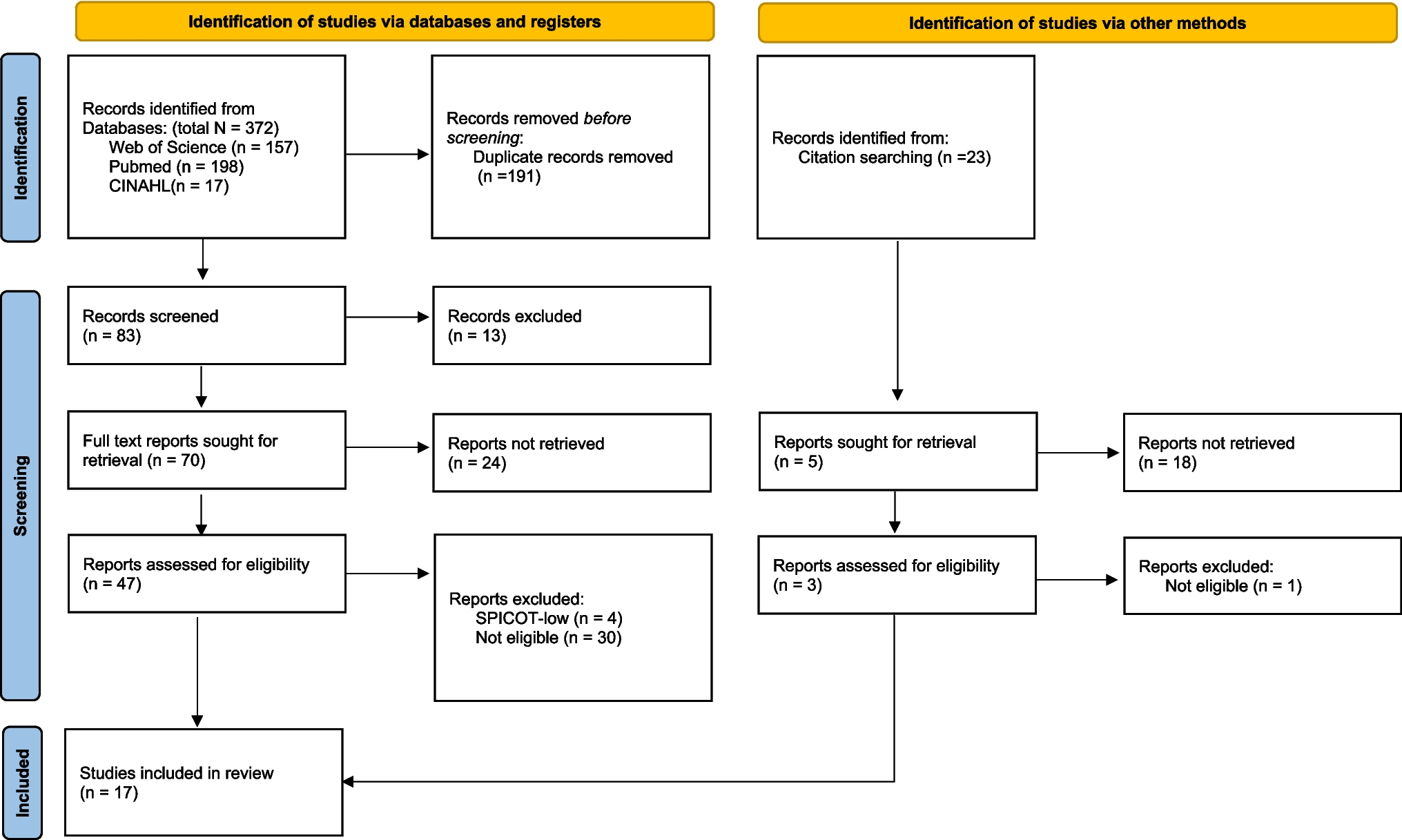


In Finland, a death needs to be reported to the police if there is a suspicion of homicide, suicide, accidental death, medical/surgical adverse event, occupational disease, or if the death is sudden and unexpected [6]. In most cases, the police orders a medico-legal autopsy to be performed by the governmental forensic medicine authority (Forensic Medicine Unit, Finnish Institute for Health and Welfare). Currently, the medico-legal autopsy rate is approximately 15% of all deaths.
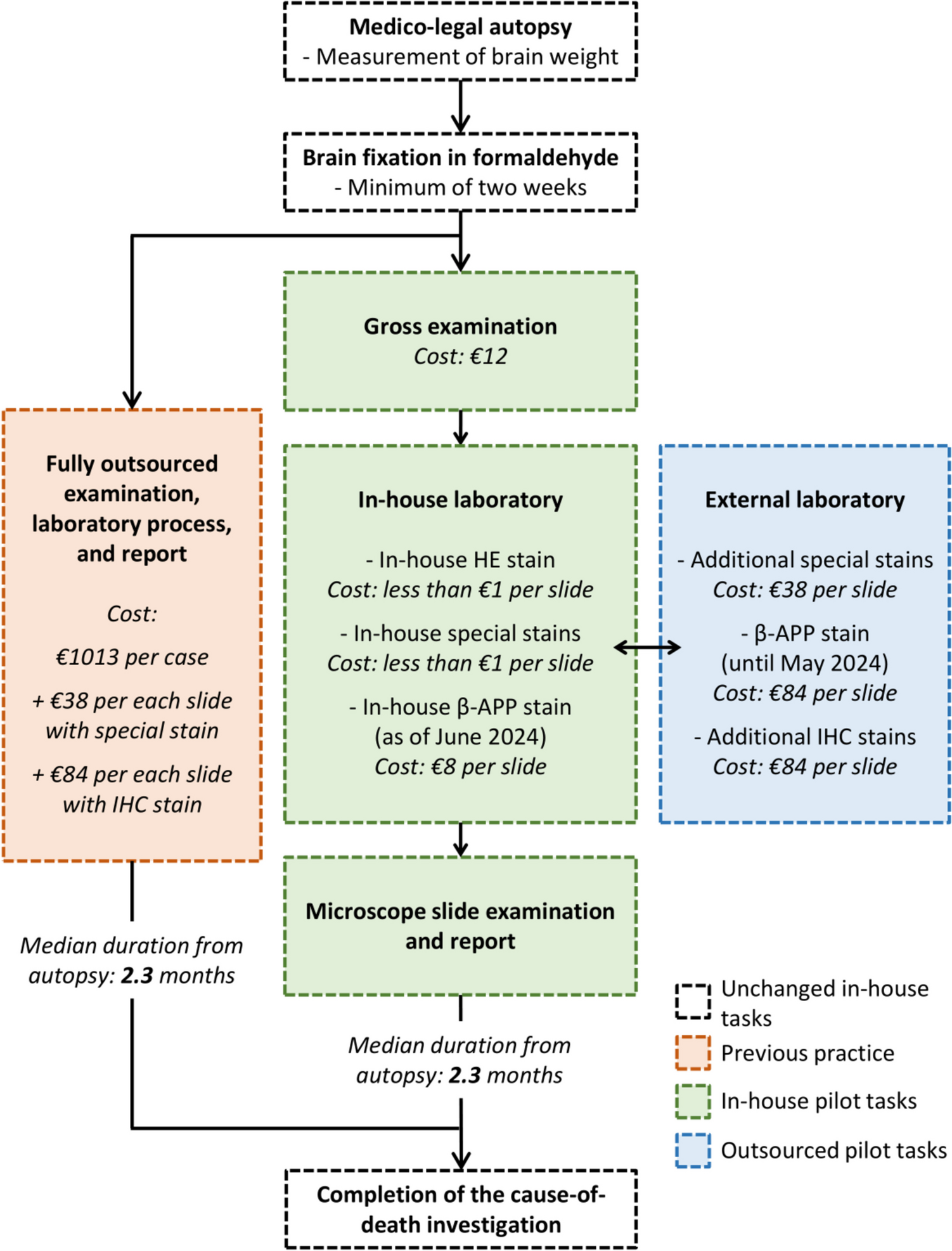
Previously, all neuropathology consultations at the Helsinki office of the Forensic Medicine Unit were outsourced to a large pathology department of a tertiary-level hospital (Fig. 1). The formaldehyde-fixed brain and other possible central nervous system (CNS) samples of the medico-legal autopsy cases that required a neuropathology consultation were delivered to the external provider. Gross examination, laboratory work, and microscopic examination of the samples were performed by a hospital neuropathologist.
Fig. 1
Flow chart of the forensic neuropathology consultation process illustrating both previous outsourced practice and in-house consultation pilot. β-APP = Beta-amyloid precursor protein, HE = Hematoxylin-eosin, IHC = Immunohistochemistry
Over the recent years, the external neuropathology consultation rate has been 1.4%, corresponding to one consultation per 70 medico-legal autopsies [5]. The main consultation theme has been traumatic brain injury (TBI); the consultant neuropathologist has often been asked to evaluate only the presence of diffuse traumatic axonal injury (dTAI) in the immunohistochemical (IHC) β-amyloid precursor protein (β-APP) stain.
In 2024, the cost of an external neuropathology consultation was €1013, plus an additional cost of €38 for each microscope slide with a special stain (such as Prussian blue or Congo red), plus an additional cost of €84 for each microscope slide with an IHC stain (Fig. 1). The median time from autopsy to a completed neuropathologist’s consultation report was 2.3 (interquartile range [IQR] 1.4—3.5) months.
Overview of the pilotIn the spring of 2023, a team of two in-house neuropathology consultants was compiled within the Helsinki office of the Forensic Medicine Unit, consisting of a neuropathology-oriented forensic pathology resident (PO) and board-certified forensic pathologist (AJH). The in-house team developed a framework and protocol for the pilot together with the forensic pathology team leader of the office (AV). As the initial step, the team systematically reviewed all external neuropathology consultation cases from the previous seven years; a detailed analysis will be published separately.
The pilot commenced in July 2023. Forensic pathologists performing routine autopsies at the Helsinki office were informed of the possibility to refer cases to the in-house consultation team. They had, however, the autonomy to refer any case to the external neuropathologist, as before, if they found it necessary. A flowchart of the pilot is included in Fig. 1. The milestones of the pilot’s first year are summarized in Fig. 2.
Fig. 2
Timeline demonstrating the milestones of the first year of the in-house forensic neuropathology consultation pilot. β-APP = Beta-amyloid precursor protein
Although the project was primarily conducted as operational development, the cases were licensed for scientific use by research permits from the Finnish Institute for Health and Welfare (THL/1802/6.02.00/2023, signature dates 2023-04-21 and 2024-02-20). This study was performed in accordance with the Declaration of Helsinki and national legislation on medical research. As the collection of data for scientific use was retrospective and register-based, ethical approval was not required.
TrainingDuring the years leading up to the pilot, both members of the in-house team underwent several months of neuropathology training as part of their forensic pathology residency. The training was completed at a large pathology department of an academic, tertiary-level hospital; it was the same one that provides external neuropathology consultations for the medico-legal cases. Training involved the examination of both surgical and autopsy-derived CNS samples under the supervision of board-certified neuropathologists. In addition, a member of the in-house team (PO) participated in a forensic neuropathology intensive course organized by the European Confederation of Neuropathological Societies (Euro-CNS) in 2023.
Case selectionAt first, in-house consultations were offered for adult TBI cases that involved only the assessment of dTAI. After the first few cases, the inclusion criteria were extended to cover all TBI and hypoxic-ischaemic encephalopathy cases. In contrast, paediatric cases as well as those in which the consultation question addressed the diagnosis of a CNS disease (e.g., demyelinating disease or tumour) were referred to the external neuropathologist, as before.
Neuropathological examination and sampling protocolAs part of the routine medico-legal autopsy, the fresh brain was examined from the outer surfaces and its weight was recorded by the referring forensic pathologist. Once the brain had been suspended in a 10 L bucket containing 10% formaldehyde for a minimum of two weeks, the gross examination was performed by a member of the in-house consultation team. An assistant (HM) was often present to aid with documentation and photography, and also the referring forensic pathologist was offered the possibility to participate in the examination.
In the gross examination, first, the outer surfaces of the formaldehyde-fixed brain were inspected, and the major arteries were dissected. Next, the brainstem and cerebellum were excised from the cerebrum at the level below the mamillary processes, and the brainstem was separated from the cerebellum at the level of the cerebellar peduncles. The brainstem and cerebellum were cut in axial and sagittal slices, respectively, of approximately 0.5 cm in thickness. Then, the cerebrum was divided into an anterior and posterior half by a coronal cut aligned with the mamillary bodies. The anterior and posterior halves were cut into approximately 1 cm thick coronal slices with the help of a standardized cutting tool. Finally, all slices were placed on a board for closer inspection, photography, and sampling.
Photographs were obtained from the external surfaces of the brain (convexities and base) before cutting, as well as from the sectioned cerebrum, cerebellum, brainstem, and potential macroscopic lesions therein before sampling.
Tissue samples were routinely obtained from a total of 23 regions (Supplementary Table 1) as well as from macroscopic lesions at the discretion of the in-house consultant. The samples were placed into standard tissue cassettes with internal dimensions 2.6 × 3.0 × 0.5 cm. The routine sampling sites were selected to cover the regions relevant to the medico-legal framework, most importantly the assessment of dTAI and hypoxic-ischaemic neuronal injury, but also to cover the assessment of common neurodegenerative diseases. The consistency of documentation and sampling were the cornerstones of the protocol.
In the first year of the pilot, a typical case was estimated to consume 3–4 h of the in-house consultant’s working time (~ 1.5 h for gross examination + ~ 2 h for microscopy and report). Of particular note is the fact that the in-house team had the possibility to consult an external board-certified neuropathologist during the process at a low threshold.
Laboratory protocolDuring the first year of the pilot, tissue stains were obtained from two different parties, namely the in-house histology laboratory, and an external provider. As illustrated in Fig. 1, the in-house laboratory provided hematoxylin-eosin (HE) and certain special stains (Prussian blue or Congo red), as well as β-APP IHC as of June 2024. Other special and IHC stains, as well as β-APP until May 2024, were obtained from an external accredited laboratory at a local pathology department.
In the in-house laboratory, HE and special stains were performed on 3–6 μm sections of formaldehyde-fixed, paraffin-embedded tissue blocks, with the help of an automated slide stainer (Sakura Tissue-Tek Prisma, Sakura Finetek Europe B.V, Alphen aan den Rijn, The Netherlands). The procedures followed general guidelines for HE [7], alkaline Congo red technique [8], and Perls’ Prussian blue reaction for ferric iron [9].
The in-house β-APP protocol was as follows: One 4 μm paraffin section on a charged slide from each sample was stained for Alzheimer Precursor Protein (APP) A4. IHC staining was performed using horseradish peroxidase polymer method in a humid chamber with EnVision FLEX, High pH kit (code K8002, Dako, Glostrup, Denmark). Deparaffinization and heat-induced epitope retrieval was performed in 3-in-1 target retrieval solution, high pH (EnVision FLEX Kit) in PT Link machine (Dako, Glostrup, Denmark) for 20 min in 97 °C. After epitope retrieval, endogenous peroxidase activity was blocked using Peroxidase Blocking reagent (EnVision Kit, 5 min), followed by primary antibody (Anti-APP A4 Antibody, a.a. 66–81 of APP , clone 22C11, 1:500, 1 h RT, code MAB348, LOT 4000311; Chemicon, Merck KGaA, Darmstadt, Germany). For detection of the antibody, HRP reagent (EnVision FLEX Kit, 20 min) was applied followed by chromogen-substrate-solution (DAB+, substrate buffer, EnVision FLEX Kit, 10 min) for visualization. Mayer’s hematoxylin was applied for 3 min as a counterstain. Slides were then dehydrated through graded alcohols, cleared with xylene and coverslipped for permanent mounting.
The β-APP protocol was implemented by an in-house laboratory scientist (RR) with the help of a member of the consultant team (PO). Validation was completed by means of a head-to-head comparison of slides stained at the external accredited laboratory (“gold standard”) and at the in-house laboratory. The comparison was based on a total of ten cases, with positive and negative findings in the diagnostically relevant brain regions for axonal injury (i.e., pons, internal capsule, corpus callosum).
DatabaseA tailored electronic database was developed by an in-house expert (MR) as a platform to prepare consultation reports and collect data for research use. It was used in all stages of the consultation and also allowed potential delays to be monitored. Most importantly, the database included details of samples and findings, most data being recorded in a structured form; a breakdown of the variables is provided in Supplementary Table 2. The database was built on Microsoft Access 2016 (Microsoft Corporation, Redmond, WA, USA) and located on a secure in-house network drive with regular back-ups (Fig. 3).
Fig. 3
Snapshots from the interface of the electronic database that was developed for the in-house forensic neuropathology consultation pilot. Top: General view of a case. Middle: Samples and stains subform. Bottom: Findings subform
In the gross examination stage, details of samples, stains, and macroscopic findings were entered into the database. Microscopic findings were added when the microscope slides were examined, and the previous macroscopic findings were amended if necessary. Finally, the in-house consultant formulated and signed an open-ended report summarizing the relevant findings and conclusions for the referring forensic pathologist. Once the case was completed, all documents (i.e., the report accompanied by a structured list of samples and findings; photographs; and the physical microscope slides) were handed over to the referring forensic pathologist. These were later stored in the official medico-legal case files and physical microscope slide archive.
Costs and durationCosts were defined as additional expenses for the Forensic Medicine Unit resulting from the in-house consultation practice. These included identifiable material costs in the gross examination and laboratory stages but not personnel costs as they would have remained unchanged regardless of the pilot. It is essential to note that the cost estimates are approximate and intended to offer a general view of the cost perspective.
In the gross examination stage, the costs comprised a disposable sponge, knife blade, tissue cassettes, and formaldehyde solution, summing up to €12 per case in total (Fig. 1). As for the laboratory work, the costs depended on the number and type of stains required. HE and special stains (Prussian blue and Congo red) were performed in-house at the cost of less than €1 per slide; in cost calculations these were rounded to €1 per slide. If other special stains or IHC stains were required, they were obtained from an external provider (€38 and €84 per slide, respectively). For the first 25 pilot cases, also β-APP was acquired from an external provider, as the in-house laboratory had not yet implemented it into its range of services. The implementation was successfully completed in June 2024; after implementation, the cost of a β-APP slide reduced significantly from €84 to €8 per slide.
Duration of the consultation was defined as the difference (months) between the autopsy and: (1) gross examination of the formaldehyde-fixed brain; (2) examination of microscope slides; and (3) completion of the consultation.
Statistical analysisThe statistical analysis was descriptive and aimed to briefly characterize the first 25 cases subjected to the in-house consultation. Key variables, extracted from the electronic database and the medico-legal case files, included the following: sex (male/female), age (years), brain weight (grams), consultation questions (TBI/hypoxic-ischaemic encephalopathy/other; multiple-choice), frequencies of samples and stains, frequencies of findings.
The distributions of categorical variables were presented using percentages (%) and frequencies (n), and those of continuous variables were presented using medians, IQRs, and full ranges (minimum—maximum). Statistical analysis was performed in IBM SPSS Statistics version 27 (IBM Corporation, Armonk, NY, USA).
留言 (0)