Study design and population
We conducted a prehospital study with prospective inclusion. A specialized research car of the municipal emergency medical service of Vienna (EMS-V), staffed with a paramedic and a study physician, responded to all cardiac arrest calls within the city. This method and the emergency service has been previously described in detail [24].
In brief, EMS-V covers Vienna, the capital of Austria, with a population exceeding 2 million. It operates a two-tiered, physician-based system that includes first-responders (app-based alert of nearby off-duty medical personnel, police with AEDs, fire engines with AEDs) and responds to approximately 1800 cardiac arrest calls annually. In Vienna, CPR is performed according to the current guidelines of the European Resuscitation Council with at least annual trainings for paramedics. Quality management on scene is performed by designated field supervisors.
The prehospital research team is stationed in the city centre and dispatched to all adult cardiac arrest calls during daytime on weekdays. During the study period, the team simultaneously screened for three studies (2 observational, 1 interventional study). Upon arrival at the scene, in- and exclusion criteria were assessed, and study enrolment commenced. To ensure the quality of data collection, the research car was always dispatched in addition to regular resources, including at least an advanced life support ambulance and a conventional EMS physician response car.
In- and exclusion criteria
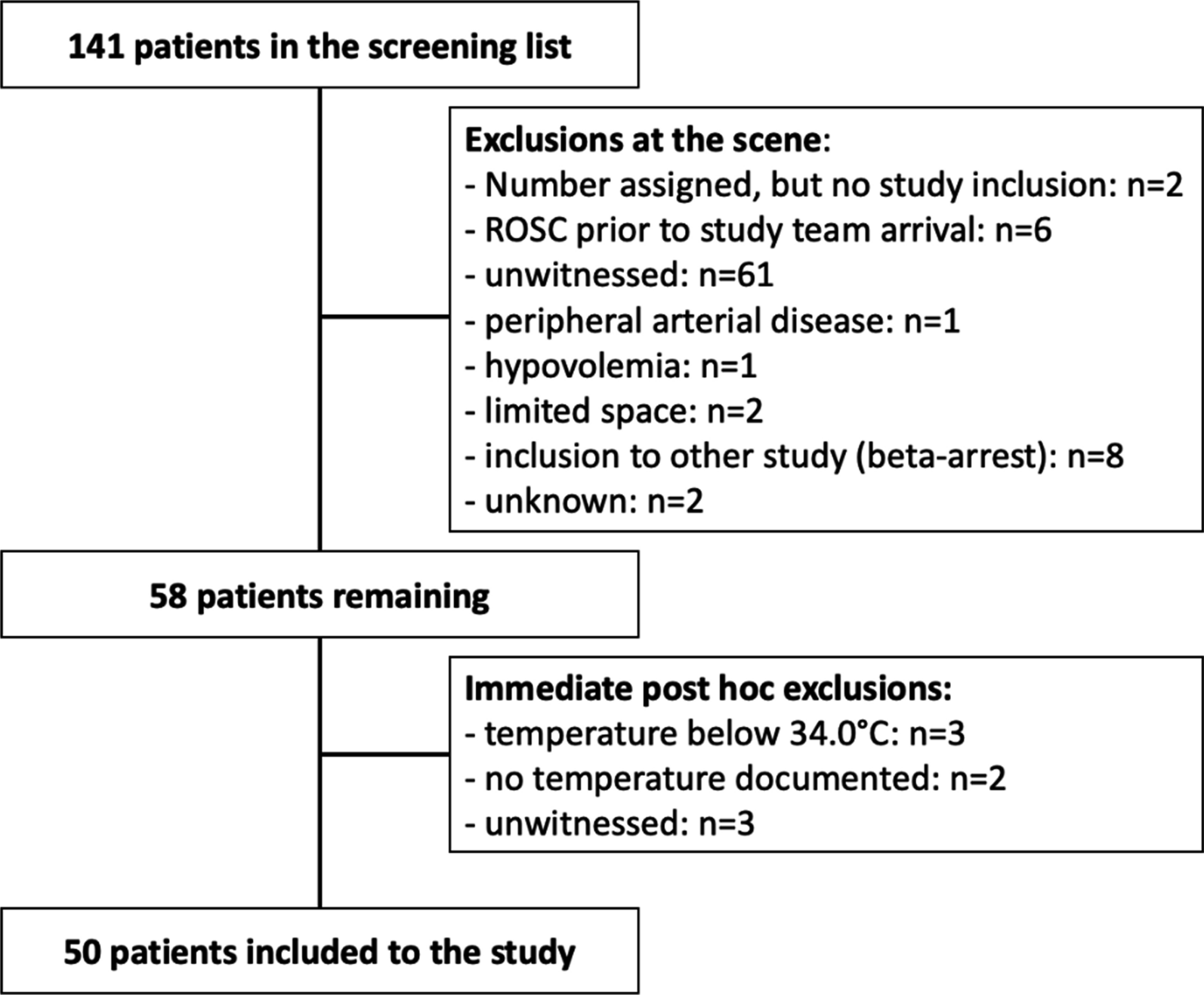
All adult patients (≥ 18 years of age) with witnessed cardiac arrest encountered throughout the study period were candidates for inclusion. Patients with hypovolemia as the presumed cause of arrest, hypo- or hyperthermia (tympanic temperatures < 34.0°, > 37.5 °C), known Raynaud’s disease or peripheral arterial disease were excluded. We further excluded patients if the study team was involved in the treatment due to insufficient manpower, or if there was a shortage of space at the scene. If resources for parallel inclusion in two studies were insufficient, priority was given to another, interventional study [25].
Measurements
The CRTs of one of the index fingers (CRT-F) and an earlobe (CRT-E) were measured every 2 min using the method described in the ANDROMEDA shock trial until any ROSC was achieved [18]. The finger’s palmar surface and the earlobe were compressed with a microscopal glass slide until the skin blanched, with pressure maintained for 10 s. Upon release, the time taken for baseline skin colour to return was registered with a chronometer. Ambient air and skin surface temperatures were measured at study inclusion with a thermohygrometer (Testo 810, Testo SE & Co KgaA, Titisee-Neustadt, Germany) with an emissivity of ϵ = 0.98 for the skin [26]. Skin surface temperature measurements were performed on the radial side in the middle of the forearm. Body temperature was measured with an ear thermometer (BRAUN Thermoscan 7, Kronberg im Taunus, Germany) equipped with hygiene caps (BRAUN, Kronberg im Taunus, Germany) at study inclusion.
Resuscitation circumstances (including first rhythm, location, basic life support, …) were documented following the UTSTEIN template [27]. Defibrillator files were collected and retained for data quality management. The study personnel was not permitted to participate in decisions regarding the continuation or withdrawal of CPR, nor were they allowed to inform the treating team about the results of the study measurements. Patient follow-up was conducted through in-person visits and telephone interviews until either day 30 or hospital discharge, whichever occurred later.
Endpoints
The primary endpoint was any ROSC, defined as palpable pulse in the absence of ongoing chest compressions. Mortality at 30 days and 30-day neurological outcome measured with a dichotomized Cerebral Performance Category (CPC; good neurological outcome: 1–2, bad neurological outcome: 3–5) were used as secondary outcomes.
Sample size considerations
This study was planned for a continuous response variable (CRT-F in seconds) for two independent groups (any ROSC/no ROSC) based on single measurements. According to the numbers from van Genderen et al. in a post-cardiac arrest cohort (survivors: 5.4 ± 0.6 s versus non-survivors: 11.0 ± 1), a sample size of 7 (2 versus 5 patients) would have sufficed to show a difference with a two-sided t-test, an alpha of 0.05, a power of 80% and with an expected fraction of 1:3 (any ROSC to no ROSC) [2]. As there were no CRT-F measurements from intra-arrest, but only post-cardiac arrest available in the literature, we were unsure whether the difference between means would be so prominent like in the data from van Genderen. From a pragmatic and clinical perspective, we decided, that the number of patients within the ROSC group should not come below n = 10, which would have resulted in 40 patients (10 vs. 30 patients). We therefore decided to use the standard deviation from this study together with the smallest possible difference that our measurement method would allow to discriminate (1 s). This finally led to our sample size consideration of 11 versus 33 patients. To account for potential loss to follow up, a practical sample size of 50 individuals was chosen. The sample size considerations were made for the main measurement (CRT-F); CRT-E measurements should be seen of exploratory character.
Statistical analysis
Continuous variables were presented as median and interquartile ranges (median [25.–75. percentile], categorical variables are depicted with frequencies and percentages (n [%]). The variability between different observers was presented descriptively. Baseline characteristics were compared with Wilcoxon-rank-sum test (continuous variables) or Chi-Square test (categorical variables). In case of an expected cell frequency of less than 5, Fisher’s exact test was used. Based on previous studies regarding CRT after ROSC, we planned to use CRT as a continuous variable and test our hypotheses with two-sided t-tests. During the first patients, it turned out that CRT > 10 s and even no refill phenomena were frequent. As it was practically impossible to distinguish clearly between particularly high CRT values (e.g. 23 vs. 24 s), we decided to cut our scale at > 10 s. However, this meant that we had to deviate from the pre-planned statistical analyses. Instead, all CRT-F and CRT-E measurements, independent from the measurement timepoint, were categorized to allow for efficient analyses whilst optimizing the retained information. Accordingly, we formed quartiles for CRT-F and tertiles for CRT-E (CRT-F: 3–5, 6–8, 9–10, > 10 s; CRT-E: 1–2 3, 4—> 10 s). For CRT-E, we were unable to group quartiles, as 37.4% of the measurements revealed a value of 3 s. The time from cardiac arrest until the first study measurements was similar in both patient groups (any ROSC/no ROSC), thus the measuring timepoints (e.g., 1st measurement vs. 1st measurement; but not the time from cardiac arrest to the measurement) were used for the graphical comparisons.
For the primary outcome, a logistic regression analysis was used to estimate the association of any ROSC as the outcome with CRT-F, or CRT-E. We adjusted these estimates to usual covariates of resuscitation research (time from CA to the measurement in minutes, age in years, sex—female/male, basic life support—yes/no, shockable initial rhythm yes/no) by adding these as independent variables to the models. Owing to the panel data structure with a variable number of repeated measurements across participants, we used cluster robust standard error estimators for the logistic regression models, because random effects models were not stable. For temporal trend analyses, the CRT-F of each patient was classified as decreasing or constant/increasing based on the first and last measurement. Trends were compared with Fisher’s exact test. Correlations were tested with Spearman’s rank correlation coefficient for the first CRT-F measurement grouped in quartiles. In a supplemental analysis, we investigated the association of clinical and environmental factors with CRT-F. We used a random effects linear regression analysis allowing for repeated measurements within patients with CRT-F quartiles as dependent variable and possible influences on CRT-F as independent variables (time from CA to measurement in minutes, age in years, epinephrine already administered, sex, basic life support, shockable initial rhythm, ambient air temperature, tympanic temperature). We tested for multicollinearity with variance inflation factors. All tests were made on a two-sided alpha of 0.05. There was no loss to follow up. No imputations for missing data were made. If not stated otherwise, there was no missing data.
This study was designed and powered to identify differences regarding the primary outcome. All secondary outcomes should be interpreted as hypotheses generating. Analyses were made with SPSS Version 29.0 (IBM Corp., Armonk, NY) and STATA SE 18.0 (StataCorp, College Station, TX), Figures were designed with GraphPad Prism 10 (GraphPad Software Inc., Boston, MA).
Ethical approval and informed consent
This study and related amendments were submitted and approved by the ethics committee of the Medical University of Vienna (EK 2427/2020) and the ethics committee of the City of Vienna (EK 21–050-0321). This trial was pre-registered at clinicaltrials.gov under the number NCT04791995 and conducted in full conformance with the ‘Declaration of Helsinki’ and its amendments.
Initial consent was waived. Post-hoc written informed consent was obtained as soon as possible after neurological recovery. Patients who died prior to a possible informed consent were included in the study.









留言 (0)