Zhang L et al. identified SII as an independent risk factor for hip fracture complicated with DVT in elderly patients, as well as a novel risk factor for preoperative DVT [15]. Their study, similar to the present one, investigated the association between SII and preoperative DVT. However, the participants in the present study were OA or RA patients undergoing TJA, whose thrombosis formation is mostly chronic. Yao et al. found the independent association between postoperative PLR and the occurrence of DVT in 733 patients after TJA [12]. Xiong et al. found that a higher NLR level was a risk factor for preoperative DVT before TKA [6]. But this study had a small sample size and only studied NLR. Unlike previous studies, it is the first to identify those higher levels of SII, MLR, NLR, and PLR are associated with preoperative DVT in OA and RA patients undergoing TJA.
Association of SII, MLR, NLR, and PLR, with DVTSII
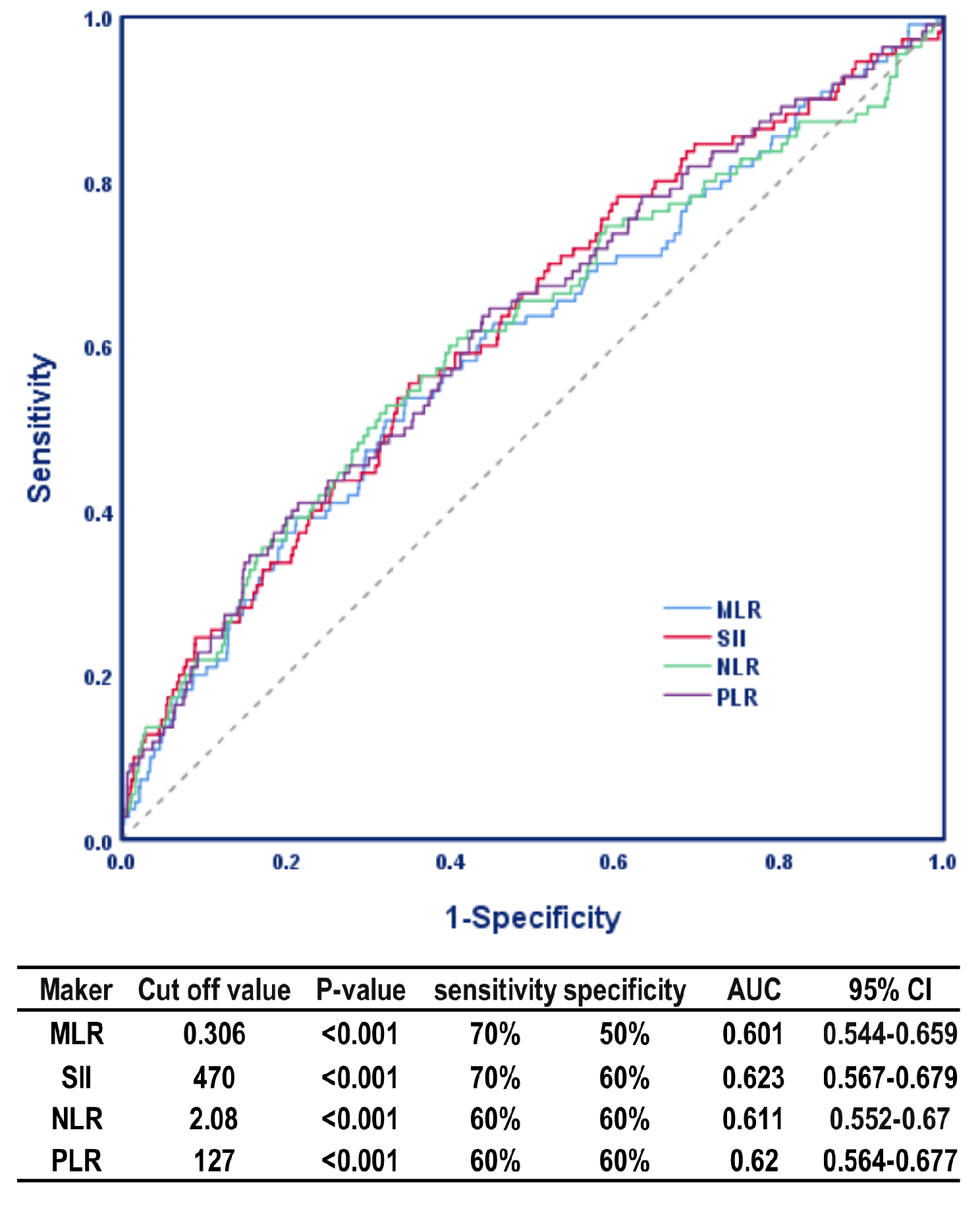
SII, a comprehensive indicator based on peripheral blood neutrophil, PLT and lymphocyte counts, has been reported to be better able to reflect the balance of immune status and host inflammatory [10]. Zhang L et al. observed that SII was an independent risk factor for hip fracture complicated with DVT in elderly patients [15]. Peng et al. observed that SII was elevated in VTE patients and was an independent predictor of VTE following hip fracture in elderly patients. According to the ROC analysis, the cut-off value was 847.78, sensitivity was 53.8%, specificity was 92.3%, and AUC was 0.795 (P < 0.001, 95% CI [0.71–0.88]) [14]. In comparison, the present study revealed a cut-off value of 470*109/L and an AUC of 0.623 (P < 0.001, 95% CI [0.567–0.679]) and identified SII ≥ 470*109 /L as an independent risk factor for preoperative DVT in patients undergoing TJA. The risk of preoperative DVT in patients with SII ≥ 470*109/L was increased by 2.26 times (P < 0.001, 95% CI [1.52–3.37]). The patients with a higher preoperative SII usually have decreased PLTs, neutrophilia, or lymphopenia, suggesting an elevated inflammatory status and weak immune response [10].
MLR
MLR has been proposed as a surrogate marker of the occurrence of endothelial inflammation and dysfunction in different populations and it also has predictive value for prognosis [16]. Zhu X et al. found that low preoperative and postoperative MLR level was significantly associated with DVT after primary TJA [13]. The present study is the first to analyze the association between SII and MLR with preoperative DVT in patients undergoing TJA. Our study found that MLR ≥ 0.306 was an independent risk factor for preoperative DVT in patients undergoing TJA and the risk of preoperative DVT in patients with MLR ≥ 0.306 increased by 1.92 times.
PLR
PLR, an indicator of innate and adaptive immunity, can be calculated from complete blood count [17]. Akboga YE et al. identified PLR and NLR as independent predictive factors for CVST and proposed that PLR > 115 and NLR > 2.1 were cut-off values [18]. Kuplay et al. found that NLR correlated with thrombus location. Mean NLR was higher in patients with proximal DVT than those with distal DVT [19]. In comparison, the present study revealed a cut-off value of 127 and AUC of 0.62 (P < 0.001, 95% CI [0.564–0.677]), and identified PLR ≥ 127 as an independent risk factor for preoperative DVT in patients undergoing TJA. When PLR ≥ 127, TJA patients had a 2.1 times higher risk for preoperative DVT (P < 0.001, 95% CI [1.4–3.16]).
NLR
NLR is also a marker of systemic inflammation, representing both adaptive and innate immunity [20]. Yao C et al. showed that high preoperative and postoperative NLR levels and low postoperative PLR level were significantly associated with DVT following TJA [12]. Seo et al. observed that VTE occurred in 102 cases at 1 week postoperatively in 264 patients after TKA and identified preoperative NLR ≥ 1.90 as the only independent predictor of postoperative VTE [21]. A high preoperative NLR (1.90) was an independent predictor of VTE after TKA, which suggests that chronic low-grade systemic inflammatory response could lead to hyper-coagulation and increase the risk of VTE [21]. Barker et al. identified a positive relationship between increased NLR level (day 1 and day 2, pre- and postoperative) and the risk of VTE after TKA [20]. Yao C et al. reported that a higher NLR was independently associated with postoperative DVT in TJA [12]. The present study found the cut-off value for NLR of 2.08 and an AUC of 0.611 (P < 0.001, 95% CI [0.552–0.67]), and NLR ≥ 2.08 was an independent risk factor for DVT formation before TJA and the risk of DVT increased by 1.94 times (P = 0.002, 95% CI [1.29–2.92]).
Neutrophil, lymphocyte, monocyte, PLT
Neutrophils are the most abundant blood leukocyte in humans. Together with monocytes, they are the major initiators of the innate immune response. PLTs form heterotypic aggregates with neutrophils as a function of platelet toll-like receptors activation in the circulation [22]. Kushnir et al. found that an elevated neutrophil count was associated with higher risk of VTE and that neutrophilia may be a marker of vulnerability to VTE [23]. Patients with a neutrophil count ≥ 9*109/L had a 2.0 times increased risk of VTE [23]. In our study, the neutrophil count was significantly higher in the DVT group of TJA patients compared to the non- DVT group (P < 0.05). An elevated neutrophil count represents a systemic inflammatory process, while the decrease of lymphocyte indicates ongoing disease-related stress [24]. Apart from its well-known inflammatory functions, the neutrophil can promote thrombus formation. It has been proven to be an essential source of TF in the early phase of thrombus formation [25].
Lymphocytes, as an important subtype of the leucocyte family, are also involved in inflammation [26]. In the present study, the lymphocyte count in DVT group was lower but the PLT count was higher than those in the non-DVT group. Therefore, our PLR count was increased. Horne BD et al. demonstrated the low lymphocyte count was associated with increased cardiovascular disease [26]. An elevated PLR reflects inflammatory status, atherosclerosis, and PLT activation [27]. Unlike higher PLTs promoting the thrombocyte activation, lymphocytes control and suppress the aggravated inflammatory process [17].
Loukov D et al. found that monocytes and neutrophils were the first circulating cells to actively accumulate at the vascular surface during DVT development [28]. Monocytes are not only the main producers of inflammatory cytokines including interleukin-1β and tumor necrosis factor α (TNF-α) [29], but also a major source of tissue factor (TF), a key initiator of DVT formation [30]. According to recent research by Amadio et al., monocytes could directly trigger DVT through PTGI2/ ANXA2/TF pathway [31].
Human PLTs are involved in pathophysiological processes, such as hemostasis and thrombosis, thrombus retraction, inflammation, vessel repair and constriction, tumor growth and metastasis, and host defense [32]. In the present study, the PLT count in the DVT group was higher than that in the non-DVT group. Elevated PLT counts can produce more CD40L and enhance an inflammatory response [33].
Association between inflammation and DVT
There are primarily two mechanisms involved in the formation of DVT in our patients with OA or RA undergoing TJA. First, the neutrophil extracellular trap (NET) mechanism, in which neutrophils, lymphocytes, monocytes, and PLTs contribute to DVT formation [38]. Chronic inflammation in both OA and RA leads to an imbalance in immune cells, with an increase in neutrophils, monocytes, and PLTs, and a decrease in lymphocytes, which promotes the formation of NETs. Second, inflammatory cytokines released in response to OA or RA further contribute to blood hypercoagulability, increasing the risk of thrombus formation. These two mechanisms interact, further increasing the likelihood of DVT before TJA in OA or RA patients. Among various inflammatory markers, those related to this inflammatory state, particularly those affecting immune cell distribution and cytokine release, are more clinically accessible and potentially more useful for predicting preoperative DVT. Therefore, we recommend the clinical application of these markers to improve risk stratification for DVT in these patients.
In addition, we found that corticosteroid use increases the incidence of preoperative DVT in TJA patients. The main mechanism may be that corticosteroids disrupt the balance between procoagulant and antithrombotic factors, increasing prothrombin levels and the concentrations of factors VII, VIII, XI, and fibrinogen, which contribute to a higher VTE risk in patients with chronic use [34,35,36].
The present study investigated the association between inflammatory indices and DVT in patients undergoing TJA by using materials including preoperative medical history, preoperative laboratory examinations, and preoperative auxiliary examinations. But it has certain limitations. For example, as a retrospective study, some data are insufficient. The AUCs for MLR, SII, NLR, and PLR were 0.601, 0.623, 0.611, and 0.62, respectively. Future studies with bigger sample size and more data might be needed to further verify the association between MLR, SII, NLR, PLR and preoperative DVT in TJA patients. Besides, the potential confounding effect of chronic inflammatory conditions in patients using steroids. Since many of the steroid users in our cohort had underlying chronic inflammatory diseases, such as rheumatoid arthritis and osteoarthritis, which are known to increase the risk of DVT, it is possible that the underlying pathology, rather than steroid use itself, contributed to the observed association with preoperative DVT. While we adjusted for key confounders, future studies should further investigate the independent effects of steroid use by stratifying patients based on the presence and severity of these chronic conditions to better isolate the role of steroids in DVT risk.





留言 (0)